Isolated Hepatosplenic Sarcoidosis- An Unusual Presentation
Sarcoidosis is a rare autoimmune condition with appearance of non-caseating granulomas in multiple sites most commonly involving pulmonary sites and hilar lymph nodes. Females are more commonly affected than males with peak age of diagnosis between 20 to 40 years. Hepatic Sarcoidosis occurs in 11% to 80% of cases and is mostly asymptomatic. Symptoms include jaundice, nausea, vomiting, abdominal pain, fatigue, pruritus, fever, arthralgias and hepatosplenomegaly. Herein, we report an unusual case of isolated hepatosplenic sarcoidosis encounterd in our routine practice.
Introduction
Sarcoidosis is a disorder of unknown etiology with multisystem involvement and has histological hallmark of non-caseating granuloma. There is predilection for lung tissue. Isolated extra-pulmonary disease is rare. The liver is the most common affected organ system after lungs and lymph nodes. There is limited data about isolated hepatic involvement in the Indian population. We would like to report such an unusual case we came across in our practice of isolated liver and spleen involvement sparing the target lungs, and presenting with fever, abdominal pain and pruritus.
Case History
A middle aged female, previously disease free, presented with a complaint of low grade fever of prolonged duration (more than a year). Patient was treated at multiple health facilities for fever and loss of weight. She was taking antipyretics on sos basis. Being from a high endemic zone for Tuberculosis, patient had been treated with antitubercular regimen, at one of the health facility she had attended previously. When she reported to our institute, her condition was worsening, with appearance of new symptoms in the form of right hypochondrial discomfort and pruritus. On evaluation, the investigations revealed hepatosplenomegaly. Suspecting disseminated Tuberculosis, she was subjected to the relevant laboratory and imaging investigations showing, normal hemogram, S. bilirubin= 0.67mg/dl, Alkaline phosphatase =280 U/ml, AST=24, ALT=23, GGT=196 IU/ ml. Triple viral markers Hepatitis B, Hepatitis C and HIV were non-reactive. Her abdominal ultrasonography showed liver size 20 cm, altered echotexture, prominent portal vein, Spleen size 15 cm, splenic vein dilated. Multiple discrete ill-defined hypodense lesions seen throughout the splenic parenchyma- likely granulomas. Other fever profile did not show any abnormality. Her CECT abdomen was done which showed gross hepatosplenomegaly with multiple ill-defined hypodense lesions, seen throughout the spleen and liver with altered echotexture of liver parenchyma (Figure 1), and possibilities of tuberculosis, primary biliary cholangitis or lymphoproliferative disorder. Although, there was no respiratory complaint, her HRCT chest was done to rule out primary lesion of tuberculosis which showed normal study. Possibility of primary biliary cholangitis was ruled out by AMA which showed negative result. Keeping in view the peculiar hepatic and splenic lesion, liver biopsy was planned. The biopsy (Figure 2) report showed multiple non necrotising epithelioid granulomas interspersed in fibrous tissue, Langhans and Foreign body giant cells with occasional asteroid body (Figure 3). Mild fibrous expansion of portal triads with moderate lymphoplasmacytic infiltrates granulomas rich in reticulin fibres, with possibility of sarcoidosis. It was an unusual finding as she had no other systemic involvement which could support the diagnosis of sarcoidosis. Her ACE level was found to be 104 IU/L (normal = 5-46 IU/L). After summing up the whole picture, with a strong diagnostic backup of liver biopsy, we came to a final diagnosis of hepatosplenic sarcoidosis with intrahepatic cholestasis. Patient was started on Tab Prednisolone 30 mg o.d with Ursodeoxycholic acid 300 mg twice a day and was followed up on two monthly bases. On follow up, her ALP was reduced, pruritus was relieved (Figure 4).
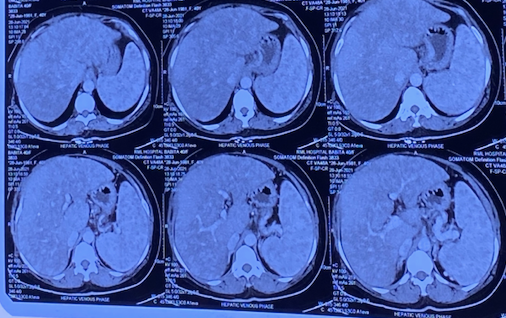
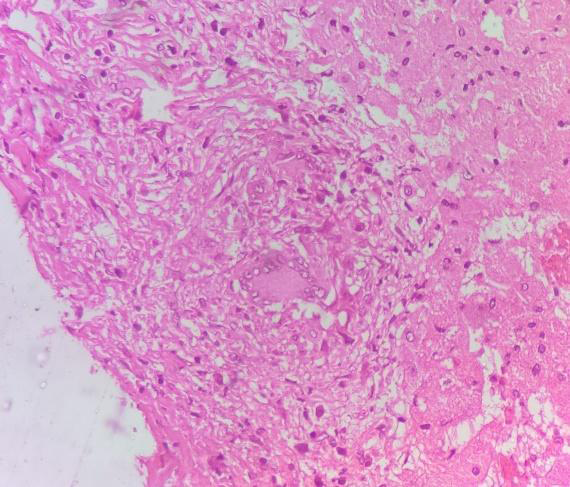
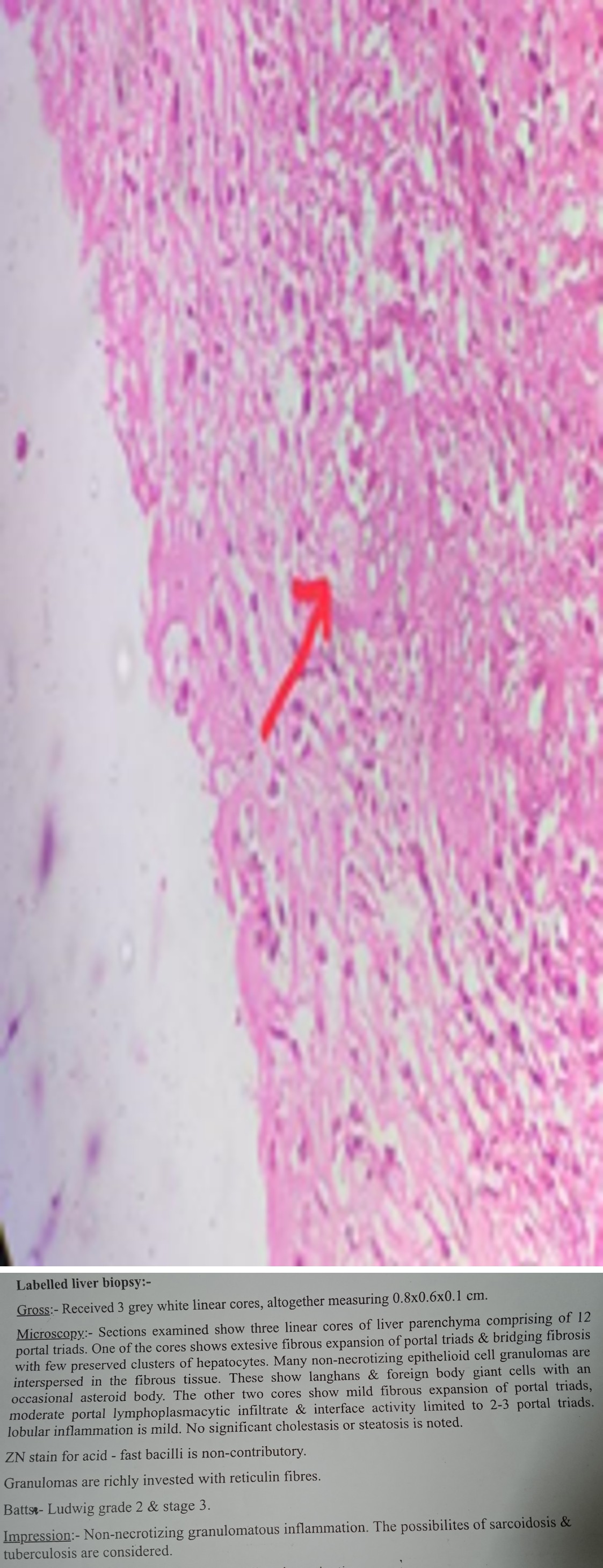
Figure 4
Discussion
Sarcoidosis primarily targets lung and hilar lymph nodes. Extrapulmonary sites like Liver, spleen, heart, bone marrow and less often eye, skin and salivary glands are documented [1, 2, 3]. Females are affected more than males, with peak age between 20 and 40 years. Hepatic sarcoidosis occurs in 11% to 80% of cases and is mostly asymptomatic [4].
Sarcoidosis should be considered as a cause of liver disease in patients presenting for the first time with derangement of liver function. In cases of chronic liver disease, where a clear underlying aetiology has not been identified, hepatic sarcoid must be excluded irrespective of the absence of pulmonary or other extrahepatic manifestations.5% to 30% of patients present with symptoms of jaundice, nausea, vomiting, abdominal pain, hepatosplenomegaly, fatigue, pruritus, fevers, and arthralgia [5].
Imaging is less sensitive for diagnosing Hepatic Sarcoidosis. Liver biopsy is the most definitive diagnostic tool.
The non-caseating granulomas in the patient were scattered all throughout the lobules and portal tracts as opposed to being centered on the bile ducts as seen in primary biliary cholangitis therefore supporting our diagnosis.
Histologically, there is a close resemblance of intrahepatic cholestasis in hepatic sarcoid and primary sclerosing cholangitis, with few differentiating features like less conspicuous bile duct damage in sarcoidosis and abundant well-formed granulomas [6, 7].
For clinical concerns such as cholestasis, first- line treatment is most often corticosteroids to reduce inflammation, granulomas, and liver size [8].
The starting dose is usually 20 to 40 mg prednisone daily or the equivalent with gradual tapering over time [9].
In countries with high prevalence of TB, differentiating sarcoidosis and tuberculosis is a tedious process, combination of clinical, radiologic, and laboratory tests are useful in reaching final diagnosis of Sarcoidosis [10].
Conclusion
Considering the rarity of the condition, isolated organ involvement in sarcoidosis is an unrecognised entity and a diagnostic challenge. Hepatosplenic sarcoidosis is a rare possibility in the evaluation of abdominal discomfort with raised ALP. Histopathological examination is the most reliable modality to reach the final diagnosis. Steroids are the mainstay of treatment. Being close mimic, patients are often mistreated with Anti tubercular treatment. The aim of this case report is to make the physicians aware about possibility of a rare, isolated involvement of hepato-splenic sarcoidosis without the involvement of any other organ.
References
-
Newman LS, Rose CS, Maier LA (1997) Sarcoidosis. N Engl J Med 336: 1224-1234.
-
Statement on Sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, (1999). Am J Respir Crit Care Med160: 736-755.
-
Baughman RP, Lower EE, du Bois RM (2003) Sarcoidosis. Lancet 361: 1111-1118.
-
Tadros M, Forouhar F, Wu GY (2013) Hepatic sarcoidosis. J Clin Transl Hepatol 1: 87-93.
-
Kumar M, Herrera JL (2019) Sarcoidosis and the liver. Clin Liver Dis 23: 331-343.
-
Lima JP, Schaffner F (1987) Chronic cholestasis in hepatic sarcoidosis with clinical features resembling primary biliary cirrhosis. Am J Med 83: 144-148.
-
Esfeh JM, Culver D, Plesec T, J Binu (2015) Clinical presentation and protocol for management of hepatic sarcoidosis. Exp Rev Gastroenterol Hepatol 9: 349-358.
-
Ghoneim S, Williams SD (2019) Hepatic Sarcoidosis: An uncommon cause of cirrhosis. Cureus. 11: 6316.
-
Sedki M, Fonseca N, Santiago P, Leige D, Mehdi M, et al. (2019) Hepatic Sarcoidosis: natural history and management implications. Front Med 6: 232.
-
Babu K (2013) Sarcoidosis in tuberculosis-endemic regions: India. J Ophthal Inflamm Infect 3**:** 53.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient