Young Man With Multiple Partially Septated Cysts in the Hepatoduodenal Ligament and Retropancreatic
The differential diagnosis of cystic liver changes includes multiple dysontogenetic cysts, liver abscesses and amoebic abscesses. Cystic changes in the abdomen with partly necrotic lymph nodes should also suggest tuberculosis, even in young and immunocompetent patients. In tuberculosis hepatoduodenal lymphadenopathies can be observed, and necrotic lymph nodes might mimic other thin-wall cystic lesions. Unexplained weight loss with clinical signs of severe infection and septicaemia also includes a differential diagnosis of consumption, i.e. miliary tuberculosis and treated immediately.
Introduction
The differential diagnosis of cystic lesions involving the liver, the hepatic portal and the hepatoduodenal ligament includes multiple dysontogenetic cysts, which also occur in the kidneys and pancreas, cystic echinococcosis, liver abscesses and amoebic abscesses [1, 2]. Cystic changes in the upper abdomen are often diagnosed as an incidental finding or as part of the imaging clarification of non-specific upper abdominal complaints. Liver cysts often do not cause any symptoms. Exceptions are very large cysts, which can exert localized pressure and cause upper abdominal discomfort. They can bleed in spontaneously or open up in the event of minor abdominal trauma and lead to spontaneous pain. Echinococcal cysts, in which a wall is clearly recognizable in imaging examinations, can be considered for differential diagnosis. Caroli syndrome, a sac-like dilatation of an intrahepatic bile duct, can occasionally be considered as a cystic fluid accumulation in the differential diagnosis but usually only occurs intrahepatic. An abscess (e.g. an amoebic abscess) in the hepatoduodenal ligament is conspicuous sonographically due to internal reflexes and is usually easy to distinguish from a congenital liver cyst; in addition, an amoebic abscess is usually associated with episodes of fever. A cystadenoma or cystadenocarcinoma is very rarely considered. Their borders are irregular; sometimes septations are recognizable and the cyst wall is accentuated.
Cystic changes in the abdomen with partly necrotic lymph nodes should also suggest tuberculosis, even in young and immunocompetent patients. Unexplained weight loss with clinical signs of severe infection and septicaemia also includes a differential diagnosis of consumption, i.e. miliary tuberculosis and treated immediately [3].
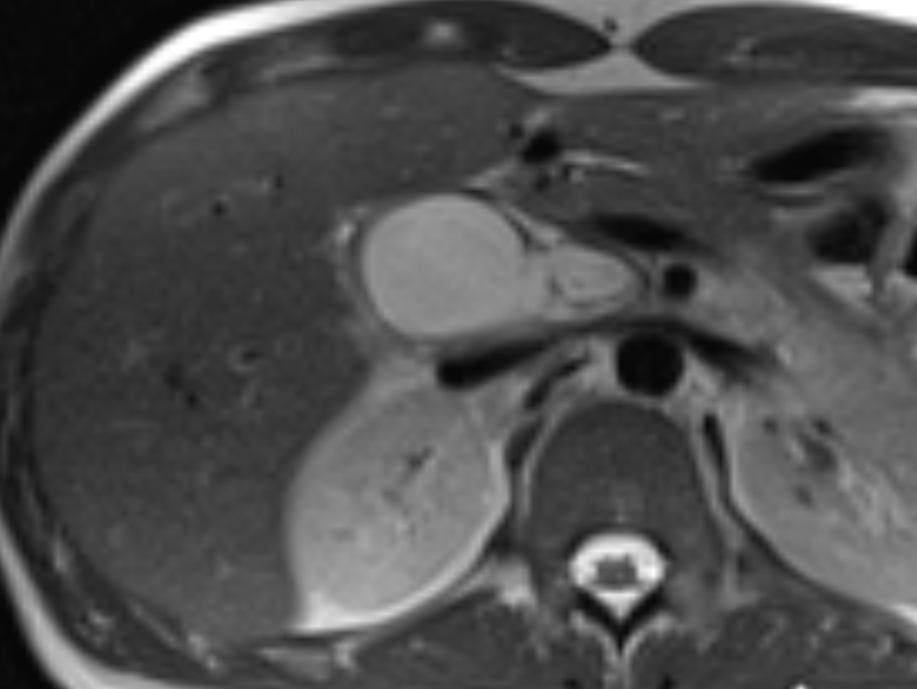
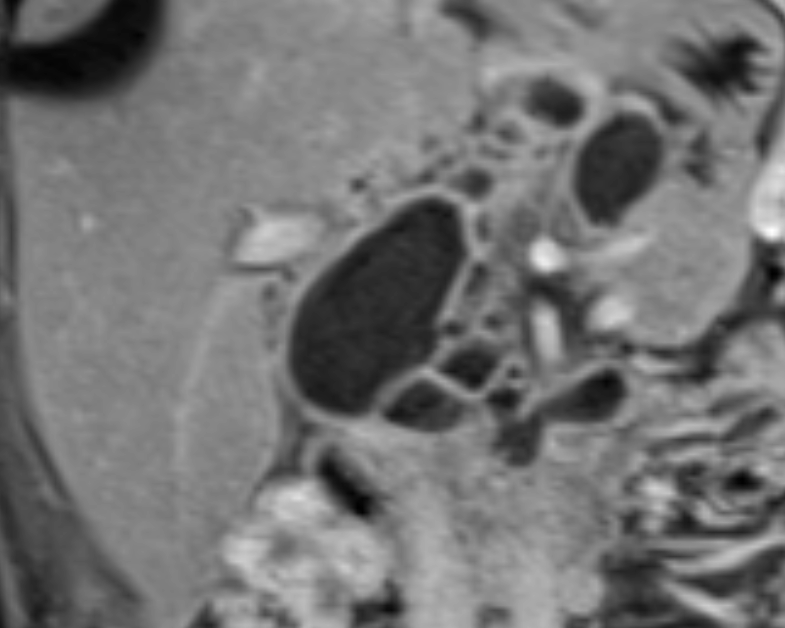
A 24-year-old patient of Pakistani origin, born and raised in Germany, presented to the outpatient clinic of a university hospital with nausea and inappetence. The student, who lived at home with his parents, denied having spent a long period of time abroad and any drug abuse. He had smoked until three years ago (3 packyears) and was now using e-cigarettes. He complained a weight loss of approximately 15 kilograms over the past six months. A subsequent external MRI scan of the abdomen showed numerous cystic structures located retropancreatic, in the liver portal and in the hepatoduodenal ligament (Figure 1 and 2). The central cyst conglomerate was located at the level of the splenic hilus. The cysts had contrast-affine walls and were rich in protein. Ultrasound and MRI showed a small amount of perihepatic ascites and increased, borderline large retroperitoneal lymph nodes.
Physical examination revealed a slender, almost lean patient with a soft abdomen and brisk intestinal peristalsis. The peripheral acres were hypothermic and the patient reported subfebrile temperatures over the past few weeks. Percussion and auscultation of the lungs and abdomen were unremarkable. There was no evidence of pulmonary consolidations or caverns in the chest X-ray examination in two planes. Laboratory chemistry revealed a high CRP, elevated ferritin and mild anemia. HIV serology was negative and chronic hepatitis was ruled out. The echinococcus titer was normal, the amoebic titer increased to 1:160 initially and one week later.
In the assumption of extensive amoebic abscesses, the patient was treated with metronidazole at a dose of 3 x 10 mg/kg body weight/day orally for 10 days/d and followed up with paromomycin for a further 10 days. This caused the CRP to drop from 63 to 24 mg/l. In the control MRI, some cysts had decreased in volume. However, the overall extent of the changes had only improved slightly. Although the clinical symptoms improved, the patient continued to lose weight and developed night sweat and a slight cough. This was followed by an amoebic titer check, which was normal, and a CT scan of the thorax (Figure 3 and 4).


After 2-3 weeks of therapy, there was a slow clinical and laboratory improvement, with a decrease in fever, CRP, and ferritin as well as a slow increase in appetite and body weight. As the clinical and serological signs of inflammation improved only very slightly, the amoebic serology was checked in the BNITM, the largest institute for tropical medicine in Germany. After a negative amoebic serology in this reference laboratory, the diagnostics were extended. High resolution computed tomography of the thorax showed calcified lymph nodes in the left hilum and disseminated miliary nodules with homogenous distribution in both lungs, typical findings of miliary tuberculosis. A tuberculosis specific interferon-gamma release assay of the whole blood showed tuberculosis antigen 1 and 2 at 1.33 resp. 1.7 IU/ ml [4]. Following the CT morphological diagnosis, the patient was treated with a quadruple therapy (isoniazid, ethambutol, pyrazinamide and rifampicin) in accordance with the international guidelines [5].
Based on a meta-analysis, the WHO previously recommended a standardised treatment duration of at least 20 months [6]. It is recommended that the initial intensive therapy phase should be carried out for at least 7 - 8.5 months [5].
The patient had worked as a baggage handler at Frankfurt Airport until three years before falling ill. An index patient could not be identified.
Discussion
The differential diagnosis of cystic liver changes includes multiple dysontogenetic cysts, which also occur in the kidneys and pancreas, cystic echinococcosis, liver abscesses and amoebic abscesses [1, 2]. With negative echinococcus serology and no abdominal pain, echinococcosis and abscesses were quickly ruled out in this case. The amoebic titer was elevated several times to 1:160, as a result of which the patient was treated with metronidazole for 10 days [7].
If pulmonary tuberculosis is clinically suspected, the chest X-ray examination plays a decisive role [8]. In the present case, tuberculosis was retrospectively ruled out too quickly due to the initially absent cough and the unremarkable X-ray examination of both lungs. Medical history, origin and lifestyle of the patient also did not give rise to any suspicion of tuberculosis. After sufficient treatment of an amoebiasis that was subsequently questionable, the cystic masses in the abdomen improved reasonably, the clinical symptoms improved only slightly and, above all, the weight loss progressed. With the onset of night sweats and intermittent coughing, we arranged for a CT scan of the thorax despite an unremarkable chest X-ray [9].
The most common manifestation of abdominal tuberculosis is certainly lymphadenopathy. The mesenteric, omental and peripancreatic lymph nodes are most frequently affected. Due to the portal disposal of venous blood in the intestinal area, these lymph nodes are most frequently infected. The altered lymph nodes are usually large and numerous, and show a peripheral enhancement with central areas on contrast-enhanced CT images [10]. Other cystic lesions, including pseudocysts, fused necrotic tumours and cysts of the pancreas and/or adjacent organs, must be differentiated from tuberculous abscesses in the hepatoduodenal ligament. In the present case, there was no typical history of tuberculosis. However, the patient suffered from epigastric pain, fever and weight loss and finally night sweats.
The thoracic CT showed the typical aspect of miliary tuberculosis. The sputum was preserved, and TBC specific IFN-γ was detected by immunoassay. The patient was admitted to hospital with immediate initiation of quadruple anti-tuberculosis therapy. In addition to microscopy and culture which were negative in the present case, the targeted use of molecular biological methods (nucleic acid amplification tests; e.g. PCR) can detect tuberculosis bacteria in test material very quickly and more sensitively than microscopy. Therefore, a species PCR should always be carried out for diagnosis, at least from one sample [11].
References
-
Mortelé KJ, Peters HE (2009) Multimodality imaging of common and uncommon cystic focal liver lesions. Semin Ultrasound CT MR 30(5): 368-386.
-
Dietrich CF, Douira-Khomsi W, Gharbi H, Sharma M, Cui XW, et al. (2020) Cystic and alveolar echinococcosis of the hepatobiliary tract - the role of new imaging techniques for improved diagnosis. Med Ultrason 22(1): 75-84.
-
Chiang SS, Graham SM, Schaaf HS, Marais BJ, Sant’Anna CC, et al. (2023) Clinical standards for drug-susceptible TB in children and adolescents. Int J Tuberc Lung Dis 27(8): 584-598.
-
Buonsenso D, Seddon JA, Esposito S, Barcellini L (2023) QuantiFERON-TB Gold Plus Performance in Children: A Narrative Review. Pediatr Infect Dis J 42(5): e158-e165.
-
Nahid P, Dorman SE, Alipanah N, Barry PM, Brozek JL, et al. (2016) Executive Summary: Official American Thoracic Society/Centers for Disease Control and Prevention/ Infectious Diseases Society of America Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis. Clin Infect Dis 63(7): 853-867.
-
Ahuja SD, Ashkin D, Avendano M, Banerjee R, Bauer M, et al. (2012) Multidrug resistant pulmonary tuberculosis treatment regimens and patient outcomes: an individual patient data meta-analysis of 9,153 patients. PLoS Med 9(8): e1001300.
-
Cohen R, Minodier P, Hau I, Filleron A, Werner A, et al. (2023) Anti-infective treatment of gastro-intestinal tract infections in children. Infect Dis Now 53(8S): 104784.
-
Hoog AV, Viney K, Biermann O, Yang B, Leeflang MM, et al. (2022) Symptom- and chest-radiography screening for active pulmonary tuberculosis in HIV-negative adults and adults with unknown HIV status. Cochrane Database Syst Rev 3(3): CD010890.
-
Alsowey AM, Amin MI, Said AM (2017) The Predictive Value of Multidetector High Resolution Computed Tomography in Evaluation of Suspected Sputum Smear Negative Active Pulmonary Tuberculosis in Egyptian Zagazig University Hospital Patients. Pol J Radiol 82: 808-816.
-
Yang ZG, Min PQ, Sone S, He ZY, Liao ZY, et al. (1999) Tuberculosis versus lymphomas in the abdominal lymph nodes: evaluation with contrast-enhanced CT. AJR Am J Roentgenol 172(3): 619-623.
-
Choudhury A, Dhillon J, Sekar A, Gupta P, Singh H, et al. (2023) Differentiating gastrointestinal tuberculosis and Crohn’s disease- a comprehensive review. BMC Gastroenterol 23(1): 246.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient