Orlistat-Resveratrol Combination Improves Elastography Parameters Over and Above Weight Loss in Overweight/Obese Patients
This 12-week, real-world, prospective, multicentre, randomized, controlled trial aimed to assess the safety and efficacy of combining Orlistat and Resveratrol compared to Orlistat alone in individuals with obesity or overweight, with or without metabolic syndrome. Both treatment groups demonstrated significant weight reduction from baseline, with the Orlistat-Resveratrol (O-R) combination group exhibiting higher weight loss than the Orlistat (O) alone group (-3.31 vs -2.92 Kg). Over 80% of participants in both groups achieved clinically significant weight loss (>5% of baseline weight). Assessment of liver health using Controlled Attenuation Parameter (CAP) scores indicated a significant reduction in hepatic steatosis in the O-R combination group compared to the O group (Δ -24.78 dB/m vs Δ -11.78 dB/m), suggesting potential benefits of Resveratrol on liver health. Although the reduction in fibrosis scores was numerically higher in the O-R group, further research is needed to confirm these findings. This combination therapy shows promise in managing metabolic-dysfunction associated steatotic liver diseases (MASLD), warranting further investigation into its long-term efficacy and safety.
Introduction
Orlistat, a well-established therapy for weight management, acts by inhibiting pancreatic lipase, thereby reducing the absorption of dietary fat. Its efficacy in promoting weight loss has been demonstrated in numerous clinical trials [1, 2]. However, studies show suboptimal weight loss attributed to either GI adverse events of orlistat or to lack of adherence to lifestyle modifications (both diet and exercise) [3].
Resveratrol, a polyphenolic compound found in red grapes and other plant sources, has gained attention for its potential role in weight management. As an antioxidant, resveratrol may exert beneficial effects on weight loss by enhancing energy expenditure through the activation of SIRT-1, a key regulator of metabolism and energy balance [4, 5, 6]. By combining orlistat and resveratrol in a fixed dose, the synergistic effects of these two compounds on weight reduction and metabolic health can be harnessed [7]. Energy expenditure mediated by resveratrol can complement the caloric restriction derived from orlistat showing a synergistic effect [4].
Sustained body weight loss has been associated with incremental benefits on liver health particularly leading to improvement in hepatic steatosis and fibrosis which are hallmarks of metabolic-dysfunction associated steatotic liver diseases (MASLD) [8, 9]. Hepatic steatosis and fibrosis, characterized by the accumulation of fat and fibrous tissue in the liver, are common consequences of obesity and can lead to serious complications including MASLD. Weight reduction has been consistently shown to ameliorate hepatic steatosis and fibrosis, highlighting the importance of effective weight management strategies in liver health [8, 9]. Liver elastography (e.g. Fibroscan) has emerged as a valuable tool in monitoring obesity-related liver disease as it assesses severity of steatosis and liver stiffness. Elastography monitoring aids in early detection of progression, guiding treatment decisions, and predicting outcomes. Its non- invasive nature makes it particularly valuable for frequent monitoring in obese individuals prone to liver complications and also avoids the need for biopsy in some patients [10].
The combined impact of nutritional therapy and medical management on weight management and its influence on liver health has not been previously investigated. Hence, this study was planned to explore the efficacy and safety of this combination (orlistat and resveratrol) as compared to orlistat alone for improving both weight management outcomes and its impact on liver health measured using elastography.
Methods
This investigation constitutes a 12-week, real-world, prospective, multicentre, randomized, controlled trial conducted in resource-limited settings between March 2022 and January 2023. The primary objective was to evaluate the safety and effectiveness of a combination of Orlistat and Resveratrol (120 mg and 100 mg, respectively) compared to Orlistat alone (120 mg) in individuals aged 18 years or older with obesity or overweight (BMI greater than or equal to 25 kg/m²). Approval for the study protocol was obtained from the Defence Services General Hospital Ethics Committee in Yangon, Myanmar, prior to initiation, and written informed consent was acquired from all participants in adherence to local regulations. The trial was registered under the ISRCTN registry (ISRCTN10642495).
Participants included individuals of all genders aged 18 years or older with a BMI of ≥25 kg/m², whether overweight or obese, with or without metabolic syndrome. Exclusion criteria encompassed prior use of orlistat or the orlistat- resveratrol combination, ongoing treatment with orlistat or orlistat-resveratrol, concurrent participation in other clinical studies within the last three months (except for survey- based studies), and a history of severe illness or conditions deemed unsuitable for the study by the investigator (such as poorly controlled psychiatric disease, HIV infection, or severe coronary artery disease).
Eligible patients were randomly assigned to either the orlistat (O) group (control group) or the orlistat-resveratrol (O-R) group (test group) in a 1:1 ratio using an online tool for random sequence generation. The control group received orlistat 120 mg thrice daily, while the test group received a combination of orlistat 120 mg and resveratrol 100 mg thrice daily for 12 weeks. The study did not integrate lifestyle interventions, and medication adherence was monitored through pill counts.
Primary efficacy endpoints included changes in weight compared to baseline and the percentage of patients achieving a weight loss of more than 5% from baseline in both the O and O-R groups. Secondary efficacy endpoints comprised of liver elastography measurements conducted with the help of FibroScan - Controlled Attenuation Parameter (CAP) for steatosis and Liver Stiffness measured as kilopascals. Based on the steatosis and liver stiffness scores, each patient was categorized from S0-S3 and F0-F4. The grades are assigned as follows: S0, no steatosis (0%–10% fat; 0–237 dB/m); S1, mild steatosis (11%–33% fat; 238–259 dB/m); S2, moderate steatosis (34%–66% fat; 260–292 dB/m); and S3, severe steatosis (>67% fat; ≥293 dB/m). F0—no fibrosis, F1—portal fibrosis, F2—periportal fibrosis, F3—bridging fibrosis, F4— cirrhosis.
All recorded adverse events and serious adverse events throughout the study were analyzed and reported according to the Medical Dictionary for Research Activities (MedDRA). Adverse event frequencies were monitored through subject interviews at each visit. Data collected were consolidated in a Microsoft Excel spreadsheet and then transferred for statistical analysis using SPSS (version 25) software. Primary and secondary endpoint results were reported with two-sided 95% confidence intervals, calculated using the paired t-test, with a p-value of <0.05 considered statistically significant.
Results
Baseline Characteristics
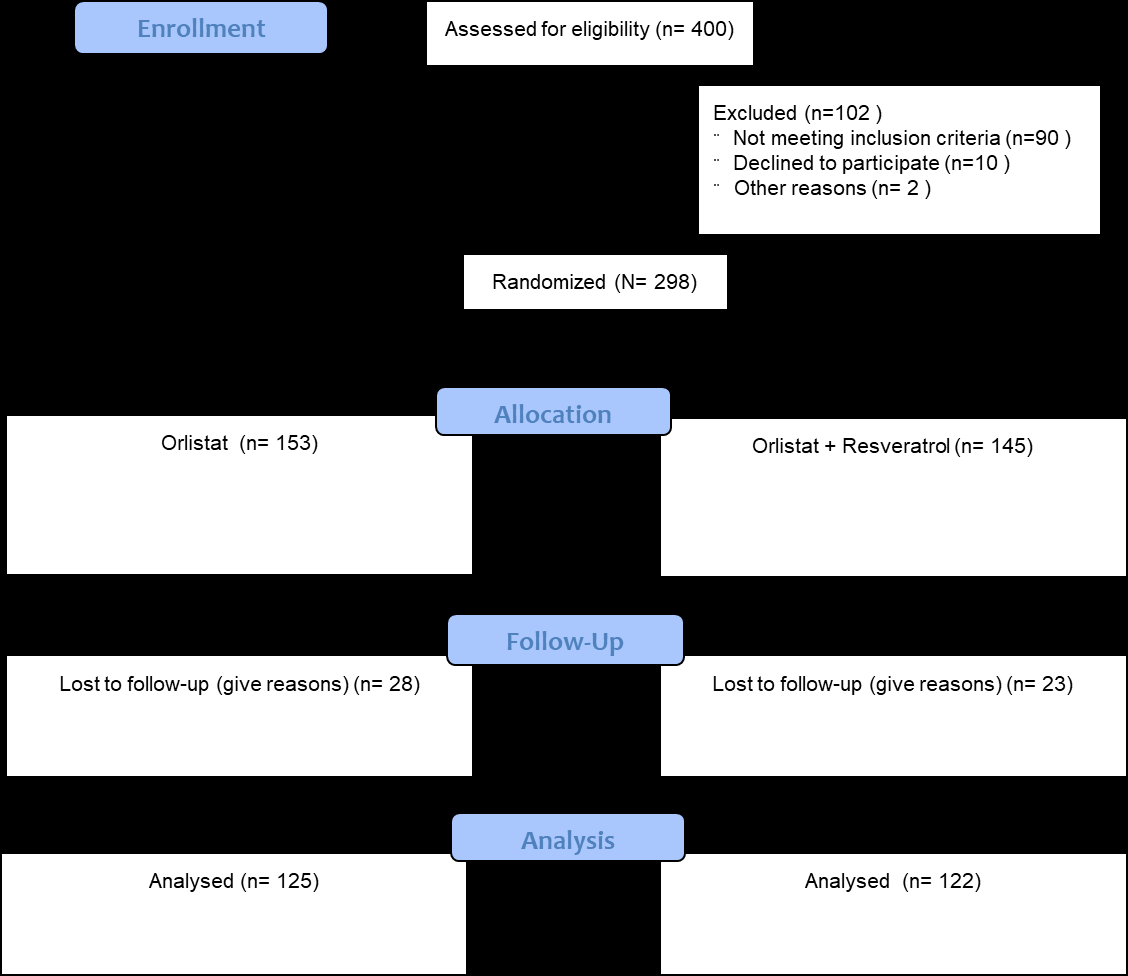
Patient disposition is illustrated in Figure 1. Of the 400 patients that were screened 298 patients were enrolled in the study and randomized to the two treatment groups.
The study included 153 participants in the Orlistat (O) group and 145 participants in the Orlistat-Resveratrol (O-R) group. 125 participants in the O and 122 participants in the O-R group respectively completed the study. Both groups had similar gender distributions, with approximately two-thirds being female. Mean weights and BMI were similar between the groups (O-R weight: 79.44 kg, BMI: 31.20 kg/m² and O weight: 80.39 kg, BMI: 31.52 kg/m²). No significant difference was recorded in the baseline elastography parameters in both the groups.
Primary Efficacy Endpoints
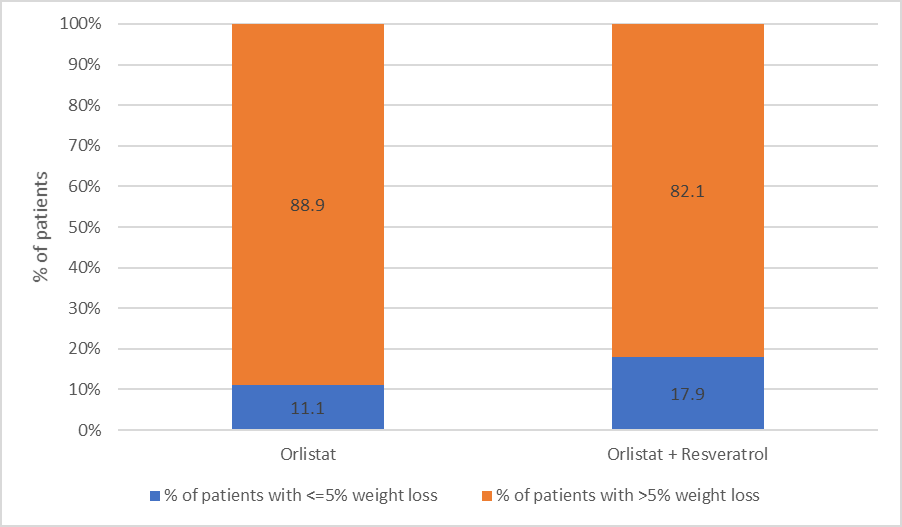
Both study groups demonstrated statistically significant weight reduction from baseline after 12 weeks of treatment. In the O-R group, a weight loss of -3.31 kg (p<0.001) was observed, which was higher than the -2.92 kg (p=0.001) observed in the O group. Additionally, at the 12-week mark, over 80% of patients in both groups (Figure 2) experienced a weight loss exceeding 5% of their initial body weight (p=0.09).
Secondary Efficacy Endpoints
The CAP scores demonstrated more favourable outcomes with the O-R combination (∆ -24.78 dB/m) than with Orlistat alone (∆ -11.78 dB/m). This suggested a significant reduction (p<0.05) and potential positive impact of resveratrol on liver health, as evidenced by the reduction in CAP scores (Figure 3A). The fibrosis scores also demonstrated a numerical reduction in the O-R combination group (∆ -0.89 KPa) as compared to orlistat alone (∆ -0.20 KPa). This change in fibrosis score was not found to be statistically significant (Figure 3B).
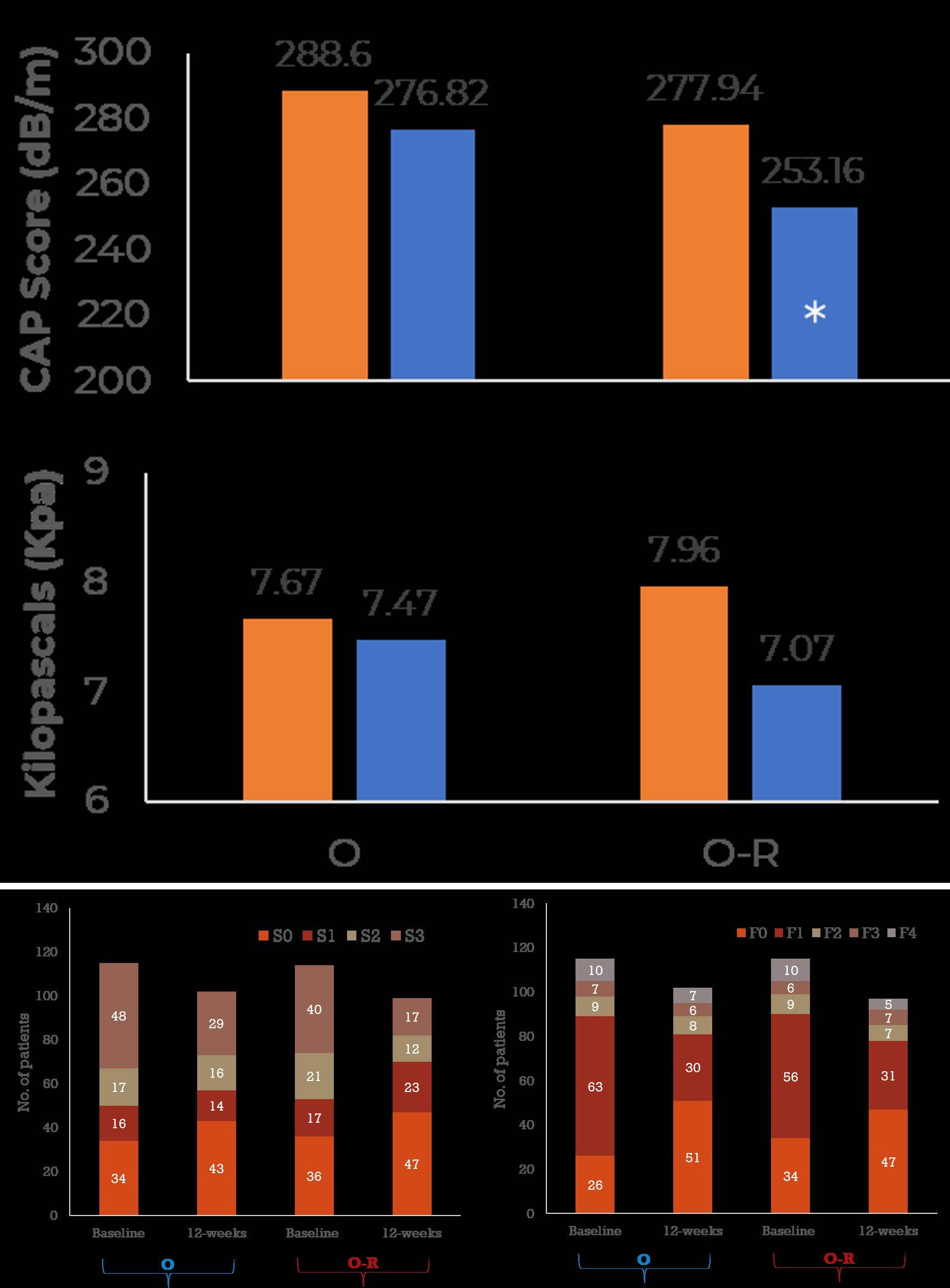
Further analysis of graded staging scores of steatosis (S0-S3) and fibrosis (F0-F4) revealed interesting insights into the effect of incremental resveratrol addition to orlistat. More patients in the O-R combination group moved towards lower steatosis grades as compared to orlistat alone. Similar effect was not observed for fibrosis grades (Figure 4A & 4B). The subgroups were not powered for calculation of statistical significance.
Figure 4A & 4B: Similar effect was not observed for fibrosis grades.
Adverse Events
Overall, the incidence of adverse events was low in this study. Steatorrhea and loose motion diarrhea were two TEAE reported during the study. Incidence of diarrhea was only reported in the O group (7 patients) suggesting a potential favorable effect of resveratrol on GI motility.
Discussion
This study contributes to the growing body of literature assessing novel therapeutic approaches for managing obesity-related liver diseases such as metabolic-dysfunction associated steatotic liver diseases (MASLD). The 12-week, real-world, prospective, multicentre, randomized, controlled trial conducted in resource-limited settings aimed to evaluate the safety and efficacy of combining orlistat and resveratrol compared to orlistat alone in individuals with obesity or overweight, with or without metabolic syndrome.
The formulation combining 120 mg orlistat with 100 mg trans-resveratrol has been previously reported in the literature.7 This formulation employs low dose resveratrol (≤500 mg/d) which is based on the phenomenon of hormesis [11]. According to this premise, resveratrol at doses less than 500 mg/d offers a protective effect but an adverse effect at higher dose.
Consistent with previous studies, both treatment groups demonstrated statistically significant weight reduction from baseline, with the Orlistat-Resveratrol (O-R) combination group exhibiting a higher magnitude of weight loss compared to the Orlistat (O) alone group. These findings corroborate the results of a study conducted in Mexico which demonstrated the efficacy of orlistat + resveratrol in promoting weight loss [7]. Moreover, a substantial proportion of participants in both groups achieved clinically significant weight loss (>5% of baseline weight), underscoring the potential clinical relevance of this combination therapy. This aligns with the findings from previous studies which highlighted the importance of achieving at least a 5% reduction in body weight for improving liver histology in patients with fatty liver disease [8, 9].
Elastography emerges as a crucial tool for monitoring liver health in obesity, providing non-invasive assessment of fibrosis severity [10]. Elastography is not recommended for patients with morbid obesity (BMI >40 kg/m2) as increased presence of fat may interfere with ultrasound capabilities of FibroScan. Fortunately, most of the patients in the present study had a BMI less than 40 kg/m2. Patients with BMI >40 kg/m2 did not undergo FibroScan without effecting the statistical power of the study.
Weight loss interventions, could positively contribute to reducing the severity of steatosis and fibrosis of the liver, emphasizing the significance of lifestyle modifications in managing obesity-related liver disease. On these lines, assessment of liver health using Controlled Attenuation Parameter (CAP) scores from FibroScan revealed a more favourable outcome in the O-R combination group, indicating a significant reduction in hepatic steatosis compared to the O group. This finding is consistent with preclinical studies suggesting the antioxidant and anti-inflammatory properties of resveratrol, which may contribute to its beneficial effects on liver health [12]. A clinical study by Theodotou et al (2019) also supports the effects of low-dose trans-resveratrol (150 mg/d) in reversing hepatic steatosis and preventing liver damage [13]. For the first time, we demonstrate that combining low dose resveratrol with orlistat can not only cause significant weight loss but also consequently lead to reduced liver fat in overweight/obese subjects. It is important to note that all these observations are based on liver elastography conducted by FibroScan and not biopsy.
Although the reduction in fibrosis scores was numerically higher in the O-R group, the difference did not reach statistical significance. This may be attributed to the short duration of the study and the relatively low baseline fibrosis scores in the study population. Further research with longer follow-up periods and larger sample sizes is warranted to elucidate the potential impact of this combination therapy on liver fibrosis.
The strengths of this study include sufficient sample size to draw meaningful conclusions on the effect of weight loss on liver health. Limitations of the study include short duration of follow up which may not capture the long-term effects of this combination on liver health.
Conclusion
In conclusion, the combination of Orlistat and Resveratrol shows promise as a therapeutic option for managing obesity-related liver diseases such as MASLD. This combination therapy not only facilitates weight loss but also exerts beneficial effects on liver histology, particularly in reducing hepatic steatosis. Given the rising prevalence of MASLD worldwide, further research exploring the long- term efficacy and safety of this combination therapy is warranted. Incorporating lifestyle interventions, such as dietary modifications and physical activity, may also enhance the therapeutic benefits of this combination in managing obesity-related liver diseases.
Financial Support
The study received financial support from Zydus Lifesciences Ltd.
Conflicts of Interest
HG is an employee of Zydus Lifesciences Ltd. All other authors have no conflicts of interest.
References
-
Anderson JW (2007) Orlistat for the management of overweight individuals and obesity: a review of potential for the 60-mg, over-the-counter dosage. Expert Opinion on Pharmacotherapy 8(11): 1733-1742.
-
Tchang BG, Aras M, Kumar RB, Aronne LJ, Feingold KR, et al. (2000) Pharmacologic Treatment of Overweight and Obesity in Adults.
-
Larson-Meyer DE, Redman L, Heilbronn LK, Martin CK, Ravussin E (2010) Caloric restriction with or without exercise: the fitness versus fatness debate. Med Sci Sports Exerc 42(1): 152-159.
-
Guerrieri D, Moon HY, Praag H (2017) Exercise in a Pill: The Latest on Exercise-Mimetics. Brain Plast 2(2): 153- 169.
-
Bird JK, Raederstorff D, Weber P, Steinert RE (2017) Cardiovascular and Antiobesity Effects of Resveratrol Mediated through the Gut Microbiota. Adv Nutr 8(6): 839-8 49.
-
Batista-Jorge GC, Barcala-Jorge AS, Silveira MF, Lelis DF, Andrade JMO, et al. (2020) Oral resveratrol supplementation improves Metabolic Syndrome features in obese patients submitted to a lifestyle-changing program. Life Sci 1:256:117962.
-
Arzola-Paniagua MA, López ERG-S, Calvo-Vargas CG, Guevara-Cruz M (2016) Efficacy of an orlistat-resveratrol combination for weight loss in subjects with obesity: A randomized controlled trial. Obesity 24(7): 1454-1463.
-
Brunner KT, Henneberg CJ, Wilechansky RM, Long MT (2019) Nonalcoholic Fatty Liver Disease and Obesity Treatment. Curr Obes Rep 8(3): 220-228.
-
Hsu CC, Ness E, Kowdley KV (2017) Nutritional Approaches to Achieve Weight Loss in Nonalcoholic Fatty Liver Disease. Adv Nutr 8(2): 253-265.
-
Mikolasevic I, Orlic L, Franjic N, Hauser G, Stimac D, et al. (2016) Transient elastography (FibroScan®) with controlled attenuation parameter in the assessment of liver steatosis and fibrosis in patients with nonalcoholic fatty liver disease - Where do we stand?. World J Gastroenterol 22(32): 7236-7251.
-
Calabrese EJ, Mattson MP, Calabrese V (2010) Resveratrol commonly displays hormesis: occurrence and biomedical significance. Hum Exp Toxicol 29(12): 980-1015.
-
Ding S, Jiang J, Zhang G, Bu Y, Zhang G, et al. (2017) Resveratrol and caloric restriction prevent hepatic steatosis by regulating SIRT1-autophagy pathway and alleviating endoplasmic reticulum stress in high-fat diet- fed rats. PLoS One 12(8): e0183541.
-
Theodotou M, Fokianos K, Moniatis D, Kadlenic R, Chrysikou A, et al. (2019) Effect of resveratrol on non- alcoholic fatty liver disease. Exp Ther Med 18(1): 559- 565.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient