Child-Pugh Score as a Predictor of Esophageal Varices in Liver Cirrhosis
Background: Child-Pugh score is used as a prognostic tool while managing a patient with liver cirrhosis. It will be helpful to grade esophageal varices (EV) in cirrhotic patients by noninvasive predictors like Child-Pugh score without doing endoscopy in high risk patient or where endoscopic facilities is not available. Objective: To evaluate the Child-Pugh Score as a predictor of esophageal varices in liver cirrhosis patients. Method: This cross-sectional study was carried out at the epartment of Medicine, Gastroenterology and Hepatology of Rangpur Medical College Hospital, Rangpur from June 2023 – November 2023 over a period of six months. By purposive sampling technique total 138 liver cirrhosis patients were included in the study. Data regarding age, sex, educational status, occupational status, marital status, monthly income, history of complications and investigations we reevaluated from patients’ history sheet and documented Investigation result sheet. Collected data were analyzed with the help of SPSS software version 22. Results on continuous measurements were presented as mean & SD (min-max) and results on categorical measurements were presented as frequency & percentage. Significance will be assessed at 5% level of significance (p<0.05). Results: Mean age of the study subjects was 42.16±12.68 years with a range of 19 to 72 years. Male to female ratio was 3.1:1. Ascites was mild in 54.3% cases and marked in 20.3% cases. Hepatic encephalopathy was mild in 23.9% cases and marked in 6.5% cases. Serum albumin was <2.8g/dl in 27.5% cases, 2.8-3.5g/dl in 71.0% cases and >3.5g/dl in 1.4% cases. Serum bilirubin was <2.0mg/dl in 55.1% cases, 2.0-3.0mg/dl in 29.7% cases and >3.0mg/dl in 15.2% cases. Prothrombin time prolongation was <4 sec in64.5% cases, 4.0 -6.0sec in29.0% cases and >6 sec in 6.5% cases. Twenty-three (16.7%) study subjects had no varices. Grading of oesophageal varices were 29.7% grade I, 37.0% grade II and 16.7% grade III. Child-Pugh classes were observed 3.6% class A, 74.6% class B and 21.7% class C. Area under ROC of Child Pugh score in predicting Oesophageal varices is 0.898. Child-Pugh score at a cutoff 8 was significant in prediction of oesophageal varices with sensitivity of 0.852, specificity of 0.826, positive predictive value (PPV) of 0.961 and negative predictive value of 0.528. Nineteen (13.8%) study subjects had variceal bleeding. Conclusion: Non-invasive Child-Pugh Score can predict the presence of EV in patients with cirrhosis. Hence, its application may decrease the burden of endoscopy.
Introduction
Gastro esophageal varices are one of the most common and severe complications of cirrhosis, and the presence of gastro esophageal varices is often correlated with severity. The overall prevalence of esophageal varices is 80% to 90% among the liver cirrhosis patients [1]. Gastric varices are present in 5% to 33% of patients with portal hypertension, with a lower incidence of hemorrhage but higher mortality [2]. Hemorrhage occurs at a yearly rate of 5% to 15% and is associated with a mortality of at least 20% at 6weeks despite significant improvements in its early diagnosis and treatment [3]. Although this complication is not included in the classical CTP score, variceal hemorrhage remains the main cause of hospitalization [4].
The Child–Turcotte–Pugh (CTP) score was developed in 1964 to evaluate the severity of liver dysfunction and predict survival in cirrhotic patients [5]. Initially, CTP score was proposed by Child and Turcotte to predict the operative risk in patients undergoing portosystemic shunt surgery for variceal bleeding. The primary version of Child–Pugh score included ascites, hepatic encephalopathy (HE), nutritional status, total bilirubin, and albumin. Pugh et al modified the Child–Pugh classification by adding prothrombin time or international normalized ratio (INR) and removing nutritional status. Child–Pugh score, due to its briefness and fairly good predictive value, has been used worldwide to evaluate liver function, predict outcomes, and optimize organ allocation for cirrhotic patients [6].
There have been few reports on predictive scores that include variceal status for outcome prediction in cirrhosis patients [7]. Cirrhotic patients were categorized according to Child-Pugh score [8]. The cirrhosis class is based on the total score. The prognosis is directly related to the score [5]. Esophageal varices were classified as small, medium and large according to World Gastroenterology Organization [9].
Materials and Method
This cross-sectional observational study was conducted on patients admitted in the department of medicine, gastroenterology and Hepatology of Rangpur Medical College Hospital, Rangpur from June, 2023 to November 2023. A total of 138 patients were selected through purposive sampling.
Inclusion criteria: a) Diagnosed patients of Liver cirrhosis b) Both male & female c) Age more than 18 years d) Participants and / or legally accepted guardians who gave consent and willing to comply with study procedure. Exclusion criteria: a) Haemodynamically unstable cirrhotic patients b) Patients taking propranolol and/or has Endoscopic band ligation (EBL) for esophageal varices c) Unwilling to participate in the study. Computer based statistical analysis were carried out with appropriate techniques and systems with the help of professional statistician. All data were recorded systematically in preformed data collection form (questionnaire) and quantitative data were expressed as mean and standard deviation and qualitative data were expressed as frequency distribution and percentage. Statistical analysis was performed by using window-based computer software devised with Statistical Packages for Social Sciences (SPSS-22) (SPSS Inc, Chicago, IL, USA). 95% confidence limit was taken. The summarized data was interpreted accordingly and was then presented in the form of tables.
Results
Table 1 shows distribution of the study subjects according to age. Mean age of the study subjects was 42.16 ± 12.68 years with a range of 19 to 72 years. Maximum patients were in age group 29–38 years (26.8%) followed by 49–58 years (23.9%), 39– 48years (21.7%), 19– 28years (16.7%) and above 58 years (10.9%).
| Age(years) | Frequency(n) | Percentage (%) |
|---|---|---|
| 19-28 | 23 | 16.7 |
| 29-38 | 37 | 26.8 |
| 39-48 | 30 | 21.7 |
| 49-58 | 33 | 23.9 |
| >58 | 15 | 10.9 |
| Mean± SD | 42.16±12.68 | |
| Min-max | 19–72 |
Table 1: Distribution of the study subjects according to age (n=138). Males (n=104) (75.4%) were predominant than females (n=34)
Figure 1 shows maximum patients were illiterate (n=49) (34.8%) followed by Secondary level (n=33)(23.9%), primary level (n=29)(21.0%), graduate (n=14) (10.1%) and Higher secondary level (n=13)(9.4%) of education.
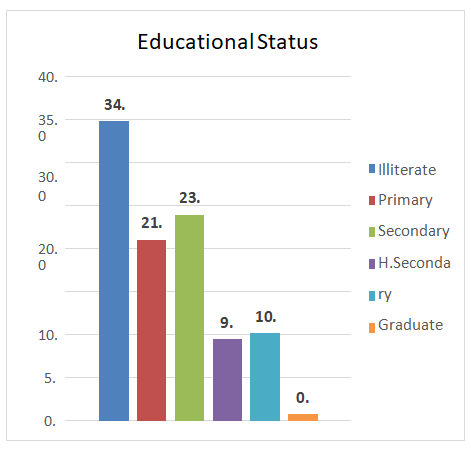
Table 2 shows distribution of the study subjects according to marital status. Maximum patients were married (83.3%) followed by widow (9.4%) and unmarried (7.2%).
| Marital status | Frequency(n) | Percentage (%) |
|---|---|---|
| Married | 115 | 83.3 |
| Unmarried | 10 | 7.2 |
| Widow | 13 | 9.4 |
Table 4: Distribution of the study subjects according to marital status (n=138).
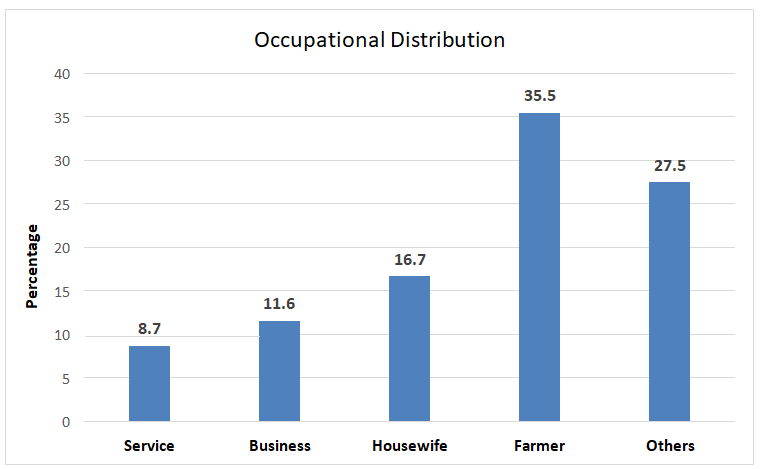
Figure 2 shows study subjects according to occupational status. Most are farmers (35.5%) (n=49).
Table 3 shows distribution of the study subjects according to monthly income. Maximum patients had monthly income <Tk. 20,000 (63.8%) followed by 29.7%had Tk.20,000 – Tk.40,000 and only 6.5% had >Tk. 40,000.
| Monthly income | Frequency(n) | Percentage (%) |
|---|---|---|
| <20,000 | 88 | 63.8 |
| 20,000-40,000 | 41 | 29.7 |
| >40,000 | 9 | 6.5 |
Table 2: Distribution of the study subjects according to monthly income (n=138).
Table 4 shows clinical and laboratory findings regarding Child-Pugh score. Ascites was mild in 54.3% cases and marked in 20.3% cases. Hepatic encephalopathy was mild in 23.9% cases and marked in 6.5% cases. Serum albumin was <2.8g/ dl in 27.5% cases, 2.8-3.5g/dl in 71.0% cases and >3.5g/dl in 1.4% cases. Serum bilirubin was<2.0mg/dl in 55.1% cases, 2.0-3.0mg/dl in 29.7% cases and >3.0mg/dl in 15.2% cases. Prothrombin time prolongation was <4 sec in 64.5% cases, 4.0 - 6.0 sec in 29.0% cases and >6 sec in 6.5% cases.
| Frequency(n) | Percentage (%) | |
|---|---|---|
| Ascites Absent | 35 | 25.4 |
| Mild | 75 | 54.3 |
| Marked | 28 | 20.3 |
| Hepatic encephalopathy | ||
| Absent | 96 | 69.6 |
| Mild | 33 | 23.9 |
| Marked | 9 | 6.5 |
| Serum albumin | ||
| <2.8g/dl | 38 | 27.5 |
| 2.8-3.5g/dl | 98 | 71 |
| >3.5g/dl | 2 | 1.4 |
| Serum bilirubin | ||
| <2mg/dl | 76 | 55.1 |
| 2-3mg/dl | 41 | 29.7 |
| >3mg/dl | 21 | 15.2 |
| Prothrombin time prolongation | ||
| <4sec | 89 | 64.5 |
| 4-6sec | 40 | 29 |
| >6sec | 9 | 6.5 |
Table 3: Clinical and laboratory findings regarding Child- Pugh score (n=138).
- Figure 3 shows twenty-three (16.7%) study subjects had no varices. Grading of oesophageal varices were 29.7% grade I,
- 37.0% grade II and 16.7% grade III.
- Table 5 shows distribution of the study subjects according to
- Child-Pugh classed. Child-Pugh classes were observed 3.6% class A, 74.6% class B and 21.7% class C.
- Child Pugh’s score
- No varices
- Oesophageal varices p-value
- Grade I
- Grade II
- Grade III
- Class A
- 4(17.4%)
- 0(0.0%)
- 1(1.9%)
- 0(0.0%)
- <0.001
- Class B
- 19(82.6%)
- 37(90.2%)
- 36(70.6%)
- 11(47.8%)
- Class C
- 0(0.0%)
- 4(9.8%)
- 14(27.5%)
- 12(52.2%)
- Total
- 23
- 41
- 51
- 23
Table 5: Association of grading of oesophageal varices with Child Pugh’s score (n=138).
| Child Pugh’s score | Frequency(n) | Percentage (%) |
|---|---|---|
| Class A | 5 | 3.6 |
| Class B | 103 | 74.6 |
| Class C | 30 | 21.7 |
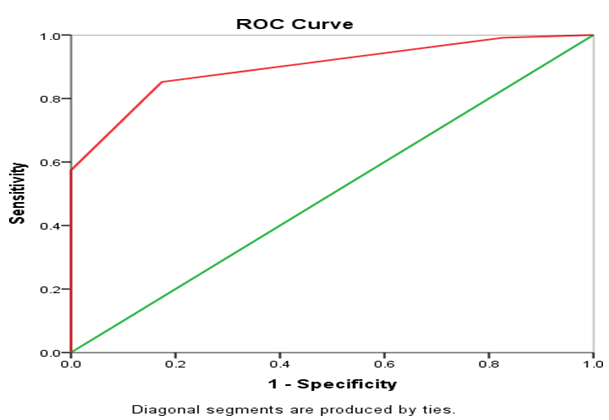
Table 6: Area under ROC of Child Pugh score in predicting Oesophageal varices is 0.898. Child-Pugh score would be considered to b
| Asymptotic 95% CI | ||||
|---|---|---|---|---|
| Area | SE | p-value | Lower Bound | Upper Bound |
| 0.898 | 0.028 | 0 | 0.843 | 0.954 |
Table 7: Area under ROC of Child Pugh score in predicting Oesophageal varices is 0.898. Child-Pugh score would be considered to b
| Child Pugh score | Sensitivity | Specificity | PPV | NPV | Youden Index |
|---|---|---|---|---|---|
| 5 | 1 | 0.049 | 0.833 | 1 | 0.049 |
| 7 | 0.991 | 0.434 | 0.857 | 0.909 | 0.425 |
| 8 | 0.852 | 0.826 | 0.961 | 0.528 | 0.678 |
| 9 | 0.574 | 0.992 | 1 | 0.318 | 0.566 |
| 10 | 0.261 | 1 | 1 | 0.213 | 0.261 |
| 11 | 0.148 | 1 | 1 | 0.19 | 0.148 |
Table 8: Youden index of Child-Pugh score in predicting oesophageal varices.
According to Youden index best cut off value of Child- Pugh score is 8 in predicting oesophageal varices.
Child-Pugh score at a cut off 8was significant in prediction of oesophagel varices with sensitivity of 0.852, specificity of 0.826, positive predictive value (PPV) of 0.961 and negative predictive value of 0.528.
Table 9 shows variceal bleeding status of the study subjects. Nineteen (13.8%) study subjects had variceal bleeding.
| Variceal bleeding | Frequency(n) | Percentage (%) |
|---|---|---|
| Present | 19 | 13.8 |
| Absent | 119 | 86.2 |
Table 9: Distribution of the study subjects according to variceal bleeding (n=138).
Discussion
Mean age of the study subjects was 42.16 ± 12.68 years with a range of 19 to 72 years. Maximum patients were in age group 29 –38 years (26.8%) followed by 49 – 58 years (23.9%), 39 – 48 years (21.7%), 19 – 28 years (16.7%) and above 58 years (10.9%). In one study, maximum patients were from 39-59 years age group (48.7%) followed by 12(32.4%) subjects from 60 years of age & above and 7(18.9%) patients from 18-38 years. Males (75.4%) were predominant than females (24.6%) [9]. Male to female ratio was 3.1:1. Among 37 patients, 27(73%) were male and 10(27%) were female in the study of Sumon, et al. (2013) [9].
Ascites was mild in 54.3% cases and marked in 20.3% cases. Hepatic encephalopathy was mild in 23.9% cases and marked in 6.5% cases. Serum albumin was <2.8g/dl in 27.5% cases, 2.8-3.5g/dl in71.0% cases and >3.5g/dl in1.4% cases. Serum bilirubin was <2.0 mg/dl in 55.1% cases, 2.0- 3.0 mg/dl in 29.7% cases and >3.0mg/dl in 15.2% cases. Prothrombin time prolongation was <4 sec in 64.5% cases, 4.0 - 6.0 sec in 29.0% cases and >6 sec in 6.5% cases.
Child-Pugh classes were observed 3.6% class A, 74.6% class B and 21.7% class C. Child-Pugh classes were observed 3(8.2%) Class A, 17(45.9%) Class B and 17(45.9%) Class C [9].
Twenty-three (16.7%) study subjects had no varices. Grading of oesophageal varices were 29.7% grade I, 37.0% grade II and 16.7% grade III. Grades of esophageal varices were 13(35.1%) F1, 20(54.1%) F2 and 4(10.8%) F3 patients among total patients [9].
Among 23 no varices cases, 4 (17.4%) were Child-Pugh class A and 19 (82.6%) were Child-Pugh class B. Among 41 grade I Oesophageal varices, 37 (90.2%) were Child-Pugh class B, 4 (9.8%) were Child-Pugh class C. Among 51 grade II Oesophageal varices, 36 (70.6%) were Child-Pugh classB and 14 (27.5%) were Child-Pugh class C. Among 23 grade III Oesophageal varices,11(47.8%) were Child-Pugh class B and 12 (52.2%) were Child-Pugh class C. Higher grade of esophageal varices was seen in the more advanced class of Child-Pugh classes. There was significant association between grading of esophageal varices and Child Pugh
classes. This study result was similar with Sumon, et al. and Thapa, et al. where they had similar correlation between Child Pugh’s score where grade B and C were associated with higher grade of varices [9, 10]. A statistically significant positive relation was found that higher grade of esophageal varices was seen in the more advanced class of Child-Pugh classes with a p value 0.001 [9].
Area under the curve (AUC) of Child Pugh score in predicting Oesophageal varices is 0.898. Child-Pugh score would be considered to be “good” at predicting Oesophageal varices. Child-Pugh score at a cutoff 8 was significant in prediction of oesophageal varices with sensitivity of 0.852, specificity of 0.826, positive predictive value (PPV) of 0.961 and negative predictive value of 0.528. Child-pugh score was significant in prediction of oesophageal varices with advanced score [11]. Nineteen (13.8%) study subjects had variceal bleeding.
However, the relationship between Child Pugh score and oesophageal varices is not consistent. Some studies fail to show a relationship between oesophageal varices and Child Pugh score [12, 13, 14, 15].
Conclusion
Bleeding from esophageal varices is the most clinically relevant complication of liver cirrhosis and still carries a high mortality which increases as Child-Pugh score rises. Non-invasive Child-Pugh score can predict the presence of EV inpatients with cirrhosis. Hence, its application may decrease the burden of endoscopy and provide a tool for selecting patients for whom endoscopy may be beneficial.
Limitations
The limitations of the study are it was a single center study with relatively small sample size. Aetiological factors could not be assessed in the study.
References
-
D’Amico G, De Franchis R, Cooperative Study Group (2003) Upper digestive bleeding in cirrhosis. Post‐ therapeutic outcome and prognostic indicators. Hepatology 38(3): 599-612.
-
Garcia‐Tsao G, Sanyal AJ, Grace ND, Carey W, Practice Guidelines Committee of the American Association for the Study of Liver Diseases, et al. (2007) Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology 46(3): 922-938.
-
Carbonell N, Pauwels A, Serfaty L, Fourdan O, Lévy VG, et al. (2004) Improved survival after variceal bleeding in patients with cirrhosis over the past two decades. Hepatology 40(3): 652-659.
-
Kim HY, Kim CW, Choi JY, Lee CD, Lee SH, et al. (2016) Complications requiring hospital admission and causes of in-hospital death overtime in alcoholic and nonalcoholic cirrhosis patients. Gut and liver 10(1): 95- 100.
-
Pugh RN, Murray‐Lyon IM, Dawson JL, Pietroni MC, Williams R (1973) Transection of the oesophagus for bleeding oesophageal varices. British Journal of Surgery 60(8): 646-649.
-
Peng Y, Qi X, Guo X (2016) Child–Pugh versus MELD score for the assessment of prognosis in liver cirrhosis: a systematic review and meta-analysis of observational studies. Medicine 95(8): e2877.
-
Kumar A, Sharma P, Sarin SK (2012) Adding variceal status to Child– Turcotte–Pugh score improves its performance in predicting early mortality in cirrhosis: the Child–Turcotte–Pugh–Kumar score. European journal of gastroenterology & Hepatology 24(11): 1348- 1349.
-
Lee JY, Lee JH, Kim SJ, Choi DR, Kim KH, et al. (2002) Comparison of predictive factors related to the mortality and rebleeding caused by variceal bleeding: Child-Pugh score, MELD score, and Rockall score. The Korean journal of Hepatology 8(4): 458-464.
-
Esophageal varices (2013) World Gastroenterology Organization Global Guidelines, World Gastroenterology Organization.
-
Sumon SM, Sutradhar SR, Chowdhury M, Khan NA, Uddin MZ, et al. (2013) Relation of Different grades of esophageal varices with Child-Pugh classes in cirrhosis of liver. Mymensingh medical journal 22(1): 37-41.
-
Thapa PB, Maharjan DK, Tamang TY, Shrestha SK (2015) Clinical correlation between Child Pugh’s score and oesophageal varices in upper gastrointestinal endoscopy in cirrhotic patient. Journal of Kathmandu Medical College 4(4): 135-139.
-
Ashraf DG, El-Sayed I (2018) Esophageal varices predictive score in liver cirrhosis. The Egyptian Journal of Internal Medicine 30(2): 72-77.
-
Chalasani N, Kahi C, Francois F, Pinto A, Marathe A, et al. (2002) Model for end‐stage liver disease (MELD) for predicting mortality in patients with acute variceal bleeding. Hepatology 35(5): 1282-1284.
-
Benedeto-Stojanov D, Nagorni A, Bjelaković G, Stojanov D, Mladenović B, et al. (2009) The model for the end- stage liver disease and Child-Pugh score in predicting prognosis in patients with liver cirrhosis and esophageal variceal bleeding. Vojnosanit Pregl 66(9): 724-728.
-
Flores-Rendón ÁR, González-González JA, García- Compean D, Maldonado- Garza HJ, Garza-Galindo AA (2008) Model for end stage of liver disease (MELD) is better than the Child-Pugh score for predicting in-hospital mortality related to esophageal variceal bleeding. Annals of Hepatology 7(3): 230-234.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient