Cell Proliferation in the Gleason Scores, Immunogold Localization of CD133 in the Stem Cells of Human Prostate, and Analysis of Embryonic Stem Cells, Including Organogenesis
We studied the cell proliferation in the Gleason histological scores, characterization of stem cells in human prostate, and analysis of embryonic cells, including organogenesis in the hope of providing new insights in the human prostate. Most studies have evaluated embryonic stem cells separately from the stem cells in adult prostate and its cancer resulting in an incomplete understanding of their relationships. We hypothesize that the stem cell proliferation in the Gleason scores can indicate the progression of the prostate cancer. We further hypothesize that the embryonic stem cells after organogenesis can continue after birth in the young and adult human prostate and its cancer. Our hypothesis is also supported by the fact that the fetal prostate (other organs) usually does not degenerate in the womb after implantation. Animal models did not show widespread apoptosis (cell death) and formation of new stem cells in embryonic stem cells. Paraffin and Epon-embedded prostate sections were studied using the light and phase contrast and electron microscopy. Methylene blue stains basic proteins in androgeninsensitive dark-staining stem cells and not the androgen-sensitive light cells. Both cell types of cells localize CD133. Basal and stem cells are closely associated with the acinar basement membrane of the prostate. Our analysis of the animal models indicated that the embryonic stem cells in the blastocysts continue in the ectoderm, mesoderm, and endoderm during gastrulation and in the fetal organ development during organogenesis. Subsequently, stem cells continue after birth in the young and adult organs (such as prostate, lungs). Each fetal organ develops specific set of stem cells and genes that are unique for that organ (such prostate, lungs) resulting in the development organ-specificity. The unrelated genes are either completely or partially inactivated and/or deleted.
Introduction
Cell Proliferation and the Gleason Scores
Gleason identified five patterns [1, 2, 3, 4, 5] in prostate tumors and by combing two patterns, he established the histological scores, ranging from scores 2 to 10 using the morphological features of the prostate glands using hematoxylin an eosin- stained sections [1, 2]. Gleason did not study cell proliferation using cell proliferation markers. Currently, the Gleason scores 4 to 10 are being used in diagnosis and treatment of the prostate cancer throughout the world. About 192,000 new cases were diagnosed in 2021 the USA and nearly 1 million cases in the world [3]. The higher Gleason score cancers are more aggressive than lower score ones [2]. We studied benign prostate (normal), benign prostatic hyperplasia (BPH) and the Gleason histologic score 4 to 9 cancer cases [4, 5, 6]. In the era of PSA-based diagnosis, the Gleason score 10 are rarely diagnosed in patients. The basal cells usually do not proliferate except in basal cell hyperplasia [7]. Earlier studies related cell proliferation to the Gleason scores [8, 9, 10, 11]. We hypothesize that stem cell proliferation can indicate the progression of the prostate cancer in the Gleason histological scores.
Stem Cells in the Human Prostate
Numbers of stem cells in olid organs are usually limited to about 1 to 2 %, as in human prostate [12, 13]. Stem cells are identified in human prostate by their location, immuno- staining, and electron microscopy [14]. Stem cells are closely associated with the acinar basement membrane. Basal cell is identified by its elongated nucleus containing mostly and cytoplasm contains small mitochondria and ribosomes. In contrast, stem cell has an oval nucleus mostly containing chromatin, cytoplasm has small mitochondria, rough endoplasmic reticulum, and ribosomes [5, 14]. These features were described by us and others as well [4, 5, 6]. Localization of biomarkers (such as alpha2 beta 1 integrin, CD44, CK33 and CK16) distinguishes stem cells from basal cells [15, 16, 17, 18, 19, 20, 21, 22, 23]. CD133 has consistently localized in the stem cells in prostate and its cancer [13, 14]. Embryonic stem cells have been studied and characterized before by several markers (such as GATA6, FOXA2, GATA4, AFP, SMO, GLI1, GLI2, GLI3) [15, 16, 17, 18, 19].
The Pluripotential Embryonic Cells and Stem Cells and Organogenesis
Stem cells were identified by a variety of markers (alpha2 beta 1 integrin, CD44) in the early 21st century [13, 14, 20, 21, 22, 23, 24]. Earlier, we studied morphological features of pluripotential embryonic cells in the inner cell mass, blastocysts, and early embryo, including placentation of the sea otter (Enhydra lutris), the western spotted skunk (Spilogale putorius latifromis), and the whitemailed deer (Odocoileus viraginous), including fetuses and fetal membranes [25, 26, 27]. These studies found that the embryonic cells were very similar in eutherian mammals [25, 26, 27]. CD133 is often used for identifying stem cells in the benign prostate and its cancer [14]. Many studies have evaluated embryonic stem cells and adult organ stem cells separately resulting in the idea that stem cells in embryos are different from the stem cells in the adult organs and their cancers We hypothesize that the embryonic stem cells found in fetal prostate can continue after birth in the young and adult prostate since there is no evidence that the fetal prostate degenerates before birth and new prostate develops after birth and in the young and adult.
Materials and Methods
The former Veteran Affairs Medical Center (VAMC) urology surgeon Dr. Clyde E. Blackard and his associates selected untreated and diethylstilbestrol (DES)-treated patients and biopsy reaps suspected of cancer as reported before [4]. The former and current VAMC urology surgeons, Drs Pratap K. Reddy and Eduardo T. Fernandes and their associates, selected prostatectomy patients for radical prostatectomy at the Minneapolis VAMC. All prostate specimens were submitted to the Pathology Service at the Minneapolis VAMC and extra specimens were provided for the research. These patients were not treated with any hormone therapy or chemotherapy prior to biopsy and prostate my. Paraffin sections used in this study were reported before and are not repeated here [4]. Biopsy specimens not used in diagnosis of PC collected between 1972 and 1975 and proctectomy specimens were collected between 1983 and 1993 at the Minneapolis VAMC. For this study, we collected untreated biopsy (# 14) and prostatectomy (# 55) samples which were processed for antibody localizations followed by examination using light, phase contrast and electron microscopy. All samples were collected after obtaining the approval of the institutional review board (IRB) guidelines in place at the VA and the University of Minnesota. Briefly, prostate pieces were fixed in a combination of paraformaldehyde and glutaraldehyde [4, 14]. After washing, pieces were post-fixed in 1% to 2% buffered osmium- tetroxide washed and dehydrated in graded ethanol, and then embedded in Epon 812 as previously described [4, 14]. For localization of MIB1 antibody IgG (ABCAM, Cambridge U.K.) prostatectomy specimens were fixed in 10% buffered formalin and embedded in paraffin as reported before [4, 14]. CD133 was localized by immunohistochemistry using immunogold localization techniques as reported [13, 19]. Former staff pathologists Drs. Donald F. Gleason and Nancy A. Staley graded Epon-embedded sections. Paraffin sections were graded by Drs. Donald F. Gleason and Stephen L. Ewing using Gleason grading system. Patients had prostate cancer with pathological grades III and IV tumors are comparable to Gleason histological scores 6 to 10 [28]. Clinical stages were B, C and D [28].
Monoclonal antibody of CD133 was kindly provided by Drs. John Ohlfest and. S. K. Swaminaathan (University of Minnesota, Minneapolis, MN). This antibody was characterized by them and found suitable for localization in neuroblastoma [29] and human prostate [14]. We localized this antibody on formalin-fixed, paraffin embedded sections of prostate using immunohistochemical methods reported before [4, 14, 30, 31]. Epon-embedded thick sections (1 to 2 micron) were prepared using LKB III Ultratome and/or Reichert-Jung microtome and used for localization of CD133 antibody in localization human prostate [14]. Sections were stained with methylene blue for morphological analysis [4, 14]. Methylene blue stains basic proteins and cells were identified dark-staining basal/stem cells [14, 30, 31]. For immunogold localization, methylene blue-stained sections were etched for 10 minutes with 10% H2O2, washed with distilled water for 10 minutes (four changes) subjected to antigen retrieval for 10 minutes with citrate buffer (pH 6.0; Invitrogen Corp., Fredrick, MD, USA), and washed with phosphate-buffered saline (PBS). After blocking of non- specific localization by a mixture of 1 to 2% bovine serum albumin and 1 to 2% normal goat or sheep C). Localization of CD133 IgG was achieved by using rabbit or mouse secondary antibody IgGs or protein A conjugated with 15 to 25 nm Aurion gold particles (Aurion Immuno Gold Reagents, Wageningen, The Netherlands). The reaction product was enhanced using an Aurion R-Gent silver enhancement kit (Electron Microscopy Sciences, Hatfield, PA, USA). For example, methylene staining and CD133 localization by immunogold and silver enhancement did not differ in light and dark cells. Details of immunogold and histochemical techniques including controls were published before [30, 31]. In this study, we used positive control of decalcified bone marrow infiltrating with leukemia cells. In another control, normal serum of animals was used in preparation of antibody and/or did not use CD133 antibody. Negative control sections did not show CD133 immunostaining [14, 31]. We studied sections by light and phase contrast and electron microscopy. For localization of MIB1 antibodies deparaffinized sections in xylene were processed through graded alcohol to water and after localization of MIB1 we processed through the graded alcohol and mounted with paramount Images were acquired directly from the slides to a Zeiss microscope-equipped with a Nikon digital camera and to a computer. Images were adjusted for uniformity of brightness or darkness by Photoshop, as needed. The laboratory study was completed before the author retired (December 31, 2019).
Results
Cell proliferation indicates progression of human prostate cancer in score 5 and 7 Gleason scores (Table 1 and Graph). Localization of CD133 antibody in decalcified bone marrow of leukemia patients embedded in paraffin sections showed numerous stem cells (Figure 1a). The positive control section was used for comparison with localization of CD133 in benign (normal) prostate, benign prostatic hyperplasia, and prostate cancer (Figures 1b-1e). Phase contrast microscopy showed more stem cells than light microscopy (Figure 1e). This indicates that the number of stem cells vary in prostate and requires evaluation of heterogeneity in stem cells by several techniques. Figure 1f shows dark and light stem cells. Further analysis indicated that human prostatic acinus contains five types of cells, namely, basal, stem niche, columnar and cuboidal cells (Figures 1b-1f,2a,2c). Basal and stem cells are closely associated with the basement membrane and the niche cells have supportive role for the stem cells. Columnar and cuboidal cells are terminally differentiated secretory yells in the human prostate. (Figures 2b,2c). Figure 2a shows localization of CD133 in prostate gland by immunogold, but not in the stroma and glandular lumen. Electron microscopy showed that the basal cell has elongated nucleus whereas the stem cell has an oval nucleus and cytoplasm containing small mitochondria, rough endoplasmic reticulum, and ribosomes (Figures 2b,2c). Our analysis of prostatic acinus indicated that only stem cells usually proliferate in human prostate.
The table shows the total number of cases with PSA. 36 cases with < 9 PSA (these patients are more responsive to treatments than those 9 patients who had >9 PSA. PSA is an independent predictor of treatment response [33]. Proliferation in Gleason scores was nearly 3 times higher than the BPH. Further analysis indicated that the cell proliferation was less than average in 34 cases and more than average in 21 cancer cases. Gleason score is an independent predictor of prostate cancer progression [1, 2].
| Count | BPH | PSA < 9 | BPH | CA | CA Less than Avg | CA Greater than Avg | |
|---|---|---|---|---|---|---|---|
| 55 | 55 | 46 | 36 | 46 | 55 | 34 | 21 |
| Cases | Avg Age | PSA > 9 | Avg | Avg CA | 34 | 21 | |
| 55 | 66.79 | 46 | 9 | 0.08 | 0.23 | 34 | 21 |
Table 1: Proctectomy Cases.
Bar shows magnification of each figure. Composite images were not uniform and were modified for uniformity in the Photoshop. Negative control sections did not show CD133 immunostaining because sections were not incubated with the primary antibodies. Additional controls have been published before [14, 30, 31].
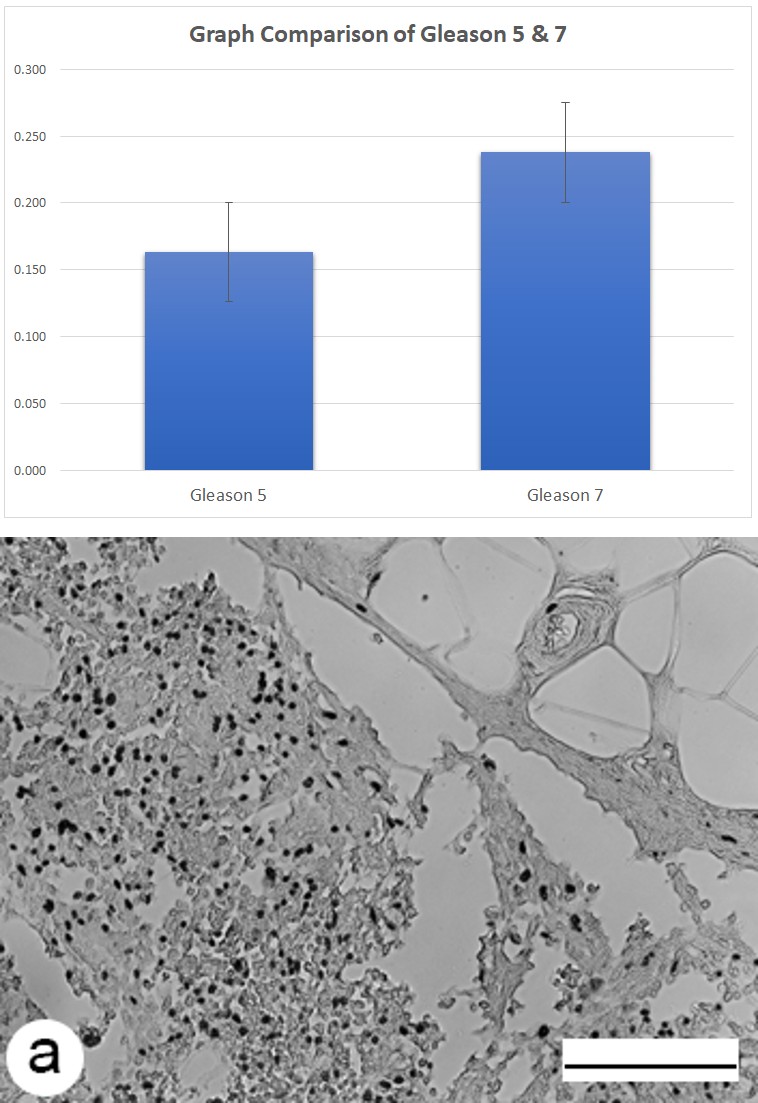
Graph 1: Gleason 5 graph does not include 1 case of Gleason 4 and 3 cases of score 6 tumors. Gleason 7 graph does not include 1 case of Gleason 8 and 3 cases of 9 tumors.
Figure 1a: Paraffin sections of decalcified bone marrow of leukemia patients were used as positive control. Numerous stem cells are shown in this figure after localization of CD133.
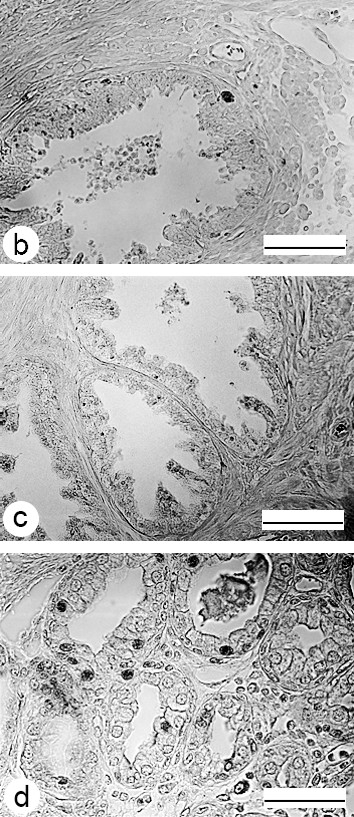
Figure 1b: Benign prostate illustrates distribution of CD133 immuno-stained stem cells in prostate gland. Only few stem cells localize CD133.
Figure 1c: Benign prostatic hyperplasia (BPH) illustrates distribution of CD133 in few immuno-stained stem cells.
Figure 1d: Prostate cancer shows distribution of CD133 immuno-stained stem cells. Gleason histologic score 6. Prostate cancer #391.
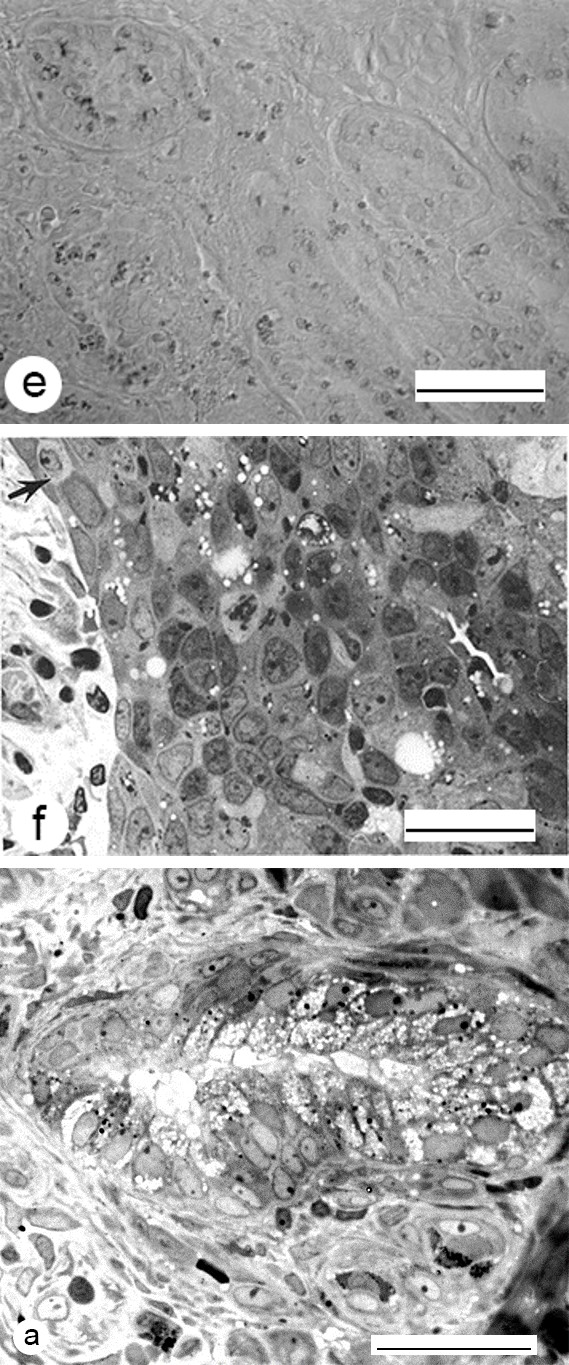
Figure 1e: Prostate cancer shows distribution of numerous CD133 immuno-stained stem cells in a phase contrast microscopy image. Compare with figure 1d. Gleason histologic score 7.
Figure 1f: Epon-embedded and methylene blue stained sections of prostate illustrate dark and light basal/stem cells in a Gleason histologic score 7 tumor.
Figure 2a: Localization CD333 in numerous prostate cancer cells by immunogold techniques shows gold particles in stem cells of a cancerous prostate. Gleason histologic score 7.
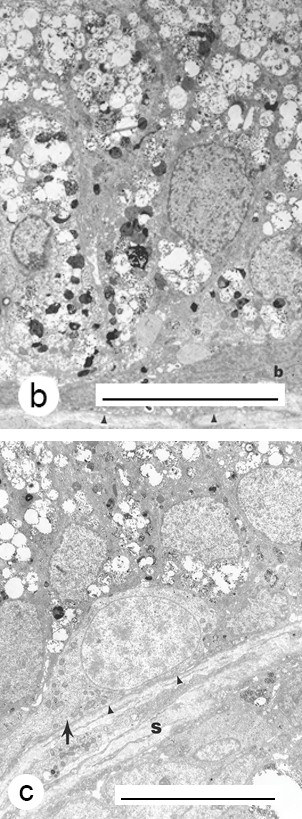
Figure 2b: Micrograph illustrates a basal cell with a spindle-shaped nucleus (b) and the basement membrane (arrows). Basal cell shows nuclear membranes, mitochondria, few ribosomes. This figure also illustrates dedifferentiated columnar/cuboidal cells and secretory granules. Case # 110.
Figure 2c: Stem cells are undifferentiated (poorly differentiated) and show chromatin distribution in the nucleus, mitochondria, and some ribosomes. Oblique section also shows some partially differentiated columnar/cuboidal cells with secretory granules). Arrow heads and an arrow illustrate basement membrane and stroma is shown by ‘s. Case# 110.
The age off prostatectomy cases ranged from 53.36 to 76.30 years, average age 66.79 years. Both BPH and CA secretions localized of MIB 1 antibody IgG antibody (in Table 1, Graph figure 1). Localization of MIB1 was lower in BPH than prostate cancer. Further analysis showed that 21 prostatectomy cases had higher cell proliferation than 34 cancer cases. Table also shows that 36 prostatectomy cases had PSA levels (<9) indicating that the patients ought to be monitored before treatment is started and patients showing PSA levels > 9 ought to receive the increased treatment [32]. The number of cases with Gleason histologic scores 4 and 6 and scores 8 and 9 were few and were not included in the graph.
Discussion
Prostate pieces are usually fixed in formalin and embedded in paraffin, sectioned, and stained in hematoxylin and eosin for examination by a pathologist. The fixation limits localization of antibodies, such as KI-67 or MIB 1. Formalin fixation gave inconsistent localization of Ki-67 in paraffin sections, but MIB1 consistently labeled proliferating cells. Our preliminary study indicates that the net cell proliferation (proliferation minus cell death) ought to be determined before any chemotherapy). The number of proctectomy cases are few in our study and it requires a clinical trial for the definitive conclusion.
Stem cells play a key role in the development organs in of the fetuses, adult organs and their cancers in humans and animals. They are distributed in the ectoderm, mesoderm, and endoderm during gastrulation and organogenesis in the womb and continue after birth in the young and adult organs (such as prostate, breast, lung, heart). There is no evidence that fetal prostate (or other organs) degenerates in the womb after implantation. The organ-specificity, undoubtedly, arose concurrently with the development of each organ during organogenesis. After organogenesis, stem cells lose their ability to function as embryonic pluripotential cells. The relevant organ-specific genes are retained (such as in the prostate), and the non-organ-specific genes (such as in the lungs) are inactivated and/or deleted. This assures that the genes associated with tongue, foot, and skin do not function in the prostate, breast, lungs, or heart muscles. The organ- specificity allows independent functioning of each organ in the fetus and after birth in the young and adult organs. The coordination of organs is dependent on brain, nerves, and hormones in hormone-dependent organs in the womb and after birth.
Formation of individual organs during organogenesis prevents circulating mutagens from inducing cancer concurrently in the unrelated organs (such as, prostate and Lung, breast, and colon). Dual primary cancers have been reported, but they are relatively rare [37]. The reasons for the origin of the dual cancers are unknown. This could be due to the incomplete inactivation of genes during organogenesis. We suggest that the potential of success of stem cell/ gene therapy is limited in the unrelated organs. The umbilical cord blood, undoubtedly, contains stem cells from many organs and are probably compromised and therefore, unsuitable for use in the stem cell therapy. In contrast, pluripotential stem cells from animals (such as pig, rabbit blastocysts) can be used successfully. Treatment of prostate cancer by stem cells has been advocated by several authors, but with limited success [32, 33, 34, 35, 36, 37, 38, 39]. In conclusion, the embryonic stem cells are the most suitable for the regeneration medicine. There is a great need for a consensus conference on the nomenclature of stem cells.
Conclusion
Some prostate cancer has more stem cells, especially those with Gleason histological scores 7 to 10 than lower score tumors. After organogenesis, stem cells become organ-specific in the fetal organs and after birth in young and adult organs (such as prostate, breast, colon, lung, and heart). Hormone-dependent prostate and breast cancers provide additional opportunities for treatment of hormone- dependent cancers. Individuals can also live longer with improved quality of life by modifying food habits and changes their lifestyle. Metastasis-induced disease is not a death sentence.
Conflicts of Interest
The author has no conflict of interest. No grant fund was used to complete this manuscript
Disclaimer
The opinion expressed in this article is that of the author and not of the U.S. Government, Department of Veterans Affairs, the Research Service of Minneapolis Veterans Affairs Medical Center or the University of Minnesota. The Research Service of Minneapolis Veterans Affairs Medical Center provided laboratory and other research facilities. The VA did not pay any salary, yet the facility was withdrawn from AAS by the Associate Chief of Staff for Research for not having a research grant funds. This led to his retirement on December 31, 2019. The Author is grateful to Drs. Donald F. Gleason, Nancy A. Staley and /Stephen L. Ewing for grading the prostate cancer sections, former staff pathologists at the Minneapolis VA Medical Center. We are also grateful to Dr. Clyde E. Blackard and his associates for biopsy and prostatectomy specimens, to Drs. John Ohlfest and S.K. Swaminathan (University of Minnesota, Minneapolis, MN) for providing the CD133 antibody. We are grateful to Mr. Francis F. Pomroy, Jr. immunohistochemical and for immunogold localization study. The author thanks Dr. Inder Anand for reviewing this manuscript and for helpful comments; Mr. Theodore Birkholz as a technology consultant; and Mr. Don Frederiksen for photoshop preparation of the figures and tale.
Acknowledgement
The Research Service of Minneapolis Veterans Affairs Medical Center provided laboratory and other research facilities. The VA did not pay any salary, yet the facility was withdrawn from AAS by the Associate Chief of Staff for Research for not having a research grant funds. This led to his retirement on December 31, 2019. The Author is grateful to Drs. Donald F. Gleason, Nancy A, Staley, and Stephen L. Ewing for grading the prostate cancer sections, former staff pathologists at the Minneapolis VA Medical Center. We are also grateful to Dr. Clyde E. Blackard and his associates for biopsy and prostatectomy specimens, to Drs. John Ohlfest and S.K. Swaminathan (University of Minnesota, Minneapolis, MN) for providing the CD133 antibody. We are grateful to Mr. Francis, F. Pomroy, Jr. immunohistochemical and for immunogold localization study. The author thanks Dr. Inder Anand for reviewing this manuscript and for helpful comments; Mr. Theodore Birkholz as a technology consultant; and Mr. Don
Frederiksen for photoshop preparation of the figures table and graph.
References
-
Gleason DF (1966) Classification of prostatic carcinomas. Cancer Chemotherapy Rep 50(3): 125-128.
-
Gleason DF (1977) Histologic grading and clinical staging of prostatic carcinoma. In: Tannenbaum M (Ed.), Urologic Pathology: The Prostate. Lea and Fibiger, Philadelphia, pp: 171-213.
-
Penberthy LT, Rivera DR, Lund JL, Bruno MA, Meyer AM, et al. (2022) An overview of real-world data sources for oncology and considerations for research. CA Cancer J Clin 72(3): 287-300.
-
Sinha AA, Blackard CE, Seal US (1977) A critical analysis of tumor morphology and hormone treatments in the untreated and estrogen-treated responsive and refractory human prostatic carcinoma. Cancer 40(6): 2836-2850.
-
Sinha AA, Blackard CE (1973) Ultrastructure of prostatic benign hyperplasia and carcinoma. Urology 2(2): 114- 120.
-
Brandes D (1966) The fine structure and histochemistry of prostate glands in relation to sex hormones. Int. Rev Cytol 20: 207-276.
-
Leav I, Schelling KH, Adams JY, Merk FB, Alroy (2001) Role of canine basal cells in postnatal prostatic development, induction of hyperplasia, and sex hormone-stimulated growth; and the ductal origin of carcinoma. J Prostate 48(3): 210-224.
-
Chen N, Zhou Q (2016) The evolving Gleason grading system. Chin J Cancer Res 28(1): 58-64.
-
Byun SS, Lee M, Hong SK, Lee H (2019) Elevated Ki- 67 (MIB-1) expression as an independent predictor for unfavorable pathologic outcomes and biochemical recurrence after radical prostatectomy in patients with localized prostate cancer: A propensity score matched study. Plos one 14(11): e0224671.
-
Iremashvili V, Pelaez L, Jorda M, Parekh DJ, Punne S (2019) A Comprehensive Analysis of the Association Between Gleason Score at a Positive Surgical Margin and the Risk of Biochemical Recurrence After Radical Prostatectomy. Am J Surg Pathol 43(3): 369-373.
-
Tollefson MK, Karnes J, Kwon ED, Mynderse LA, Cheville JC, et al. (2014) Prostate Cancer Ki-67 (MIB1) Expression, Perineural Invasion, and Gleason Score as Biopsy-Based Predictors of Prostate Cancer Mortality, the Mayo model. Mayo clin Proc 89(3): 308-318.
-
Marzo AMD, Nelson WG, Meeker AK, Coffey DS (1998) Stem cell features of benign and malignant prostate epithelial cells. J Urol 160(6 Pt 2): 2381-2392.
-
Richardson GD, Robson CN, Lang SH, Neal DE, Maitland NJ, et al. (2004) CD133, a novel marker for human prostatic, epithelial stem cells. J Cell Sci 117(Pt 16): 3539-3545.
-
Sinha AA, Wilson MJ (2018) Identification of two types of stem cells in methylene blue-stained sections of untreated and diethylstilbestrol-treated human prostate cancer and their characterization by immunogold localization of CD133. Anticancer Res 38(10): 5725- 5732.
-
Hadjantonakis A, Papaioannou V (2001) The stem cells of early embryos. Differentiation 68(4-5): 159-166.
-
Gordon K (2005) Embryonic stem cell differentiation: emergence of a new era in biology and medicine in mouse embryonic stem cells. Genes Dev 19(10): 1129- 1155.
-
Liu JH, Feng M, Li SY, Nie S, Wang H, et al. (2020) Identification of molecular markers associated with the progression and prognosis of endometrial cancer: a bioinformatic study. Cancer Cell Int 20: 59.
-
Dawud RA, Graffmann N, Ferber S, Wruck W, Adjaye J (2018) Pluripotent stem cells: induction and self- renewal. Philos Trans R Soc Lond B Biol Sci 373(1750): 20170213.
-
Alexandrova S, Kalkan Humphreys P, Riddell A, Scognamiglio R, Trumpp A, et al. (2016) The developmental potential of the inner cell mass of blastocysts that were derived from mouse ES cells using nuclear transfer technology. Development 143: 24-33.
-
Collins AT, Habib FK, Maitland NJ, Neal DE (2001) Identification and isolation of human prostate epithelial stem cells based on alpha 2 beta-1-integrin expression. J Cell Sci 114(Pt 21): 3865-3872.
-
Lang SH, Frame FM, Collins AT (2009) Prostate cancer stem cells. J Pathol 217(2): 299-306.
-
Kasper S (2008) Exploring the origins of the normal prostate and prostate cancer stem cellS. Stem Cell Rev 4(3): 93-201.
-
Miki J, Furusato B, Li H, Gu Y, Takahashi H, et al. (2007) Identification of putative stem cell markers, CD133 and CXCR4, in hTERT-immortalized primary nonmalignant and nonmalignant tumor derived hum prostate epithelial cell lines and in prostate cancer specimens. Cancer Res 67(7): 3153-3161.
-
Lawson DA, Witte ON (2017) Stem cells in prostate cancer initiation and progression. J Clinical Invest 117(8): 2044-2050.
-
Mossman HW (1987) Vertebrate fetal membranes, 16th Chapter Ovulation place of fertilization: blastocyst morphogenesis. Rutgers University Press, New Jersey; pp: 74-78.
-
Denker HW (2020) Rise of the rabbit model for implantation research: A commemoration of the scientific work of Bent Gouging (1920-2019) Biol Reprod 102(6): 1170-1176.
-
Carter AM, Enders AC, Pijnenborg R (2015) Implantation and placentation of primates. Phil Trans R Soc B 370: 1-17.
-
Ellis WJ, Lange PH (1994) Prostate cancer. Endocrinol Metab Clin North Am 23: 809-824.
-
Swaminaathan SK, Olin MR, Forestor CL, Cru K, Panyan J, et al. (2010) Identification of a novel monoclonal antibody recognizing CD133. J Immunnol Methods 36(1- 2): 110-115.
-
Sinha AA, Pomroy FE, Wilson MJ (2016) Concurrent androgen and estrogen localization ablation and inhibition steroid biosynthetic enzyme treatment of castration resistant prostate cancer. Anticancer Res 36(8): 3847-3854.
-
Sinha AA, Wilson MJ, Gleason DF (1987) Immunoelectron microscopic localization of prostatic- specific antigen in human prostate by the protein A gold complex. Cancer 60(6): 1288-1293.
-
Yamanaka S (2020) Pluripotential-based stem cell therapy-promise and challenges. Cell Stem Cell 27(4): 523-529.
-
Insan MB, Jaitak V (2014) New Approaches to Target Cancer Stem Cells: Current Scenario. Min- Reviews Medicinal Chem 14(1): 20-34.
-
Bhattacharyya S, Khandu JKL (2010) New hope in the horizon: cancer stems cells. Acta Biochim Biophys Sci 42(4): 237-242.
-
Leao R, Domingos C, Figueiredo A, Tabori UH, Branco PC (2017) Cancer stem cells in prostate cancer: Implications for targeted therapy. Urol Int 99(2): 125-136.
-
Harris KS, Kerr BA (2017) Prostate cancer stem cell markers drive progression, therapeutic resistance and bone metastasis. Stem Cell Int 2017: 8629234.
-
Boice Jr JD, Curtis RE, Kleinman RA, Flannery JT, Frauneni Jr FE (1986) Multiple primary cancers in Connecticut, 1935-82. Yale J Biol Med 59(5): 533-545.
-
Joran CT, Guzman ML, Noble M (2006) Cancer stem cells. N Engl J Med 355(12): 1253-1261.
-
Adamowicz J, Pakravan K, Bakhshinejad B, Drewa T, Babashah S (2017) Prostate cancer stem cell from theory to practice. Scand J Urol 51(2): 95-106.
- Superposition of Cryo-EM and AlphaFold Predictions of Dengue Antigen-Antibody Complexes
- Jugular-Applied Coherent Low-Level Laser Therapy Enhances Systemic Mitochondrial Metabolic Function and Antioxidant Response
- Role of OMC32 Polypeptide in Acrosin-Mediated Exocytosis during the Bovine Sperm Acrosome Reaction
- Association of Galectin-3 but not Laminin in Tamoxifen-Induced Growth Suppression in Breast Cancer MCF-7 Cells
- Effect of Different Wavelengths of Light on the Rate of Photosynthesis
- Nutritional, Therapeutic, and Environmental Effect of Oyster Mushrooms: An Editorial