A Review Paper on Lipoprotein(a) and its Biochemical Relevance as a Risk Factor in the Assessment of Cardiovascular Disease
The accumulation of lipids in the forms of increased total cholesterol (High Density Lipoprotein), Triglycerides, Low Density Lipoprotein) in the blood stream is significant of several health conditions such as coronary congestive heart disease, atherosclerosis, heart failure and several other forms of cardiovascular diseases. Although several blood tests such as lipid profiling of individuals with diabetes type II as well as stroke has been the gold standard for the detection of increased total cholesterol in the arteries but this review paper revealed significant levels of the concentration of lipoprotein(a) (p<0.05) when measured in the assessments of individuals with diabetes. The ultimate reason for this research work is that measurements of lipoprotein(a) has proved to be more sensitive, accurate and specific in the detection of cholesterol especially with the measurement of low -density (LDL) lipoprotein as indicated in this research compared to the conventional methods of lipid profiling.
Introduction
Lipoprotein(a) and Cardiovascular Diseases
Cardiovascular disease has been reported to be the leading cause of death worldwide [1]. However, levels of lipids and lipoprotein particles are known to cause a major underlying pathological contribution to the inflammatory processes that bring about the problems of atherosclerosis, coronary artery disease, stenosis, heart attacks, which are some examples of a cardiovascular disease. The proper regulation of the primary function of the cellular components of the body and its metabolism is done by diverse groups of lipids such as the fats, oils and hormones. Although lipids are organic and are soluble in these substances but insoluble in water. Lipoproteins such as ‘High Density Lipoproteins’ are known as the ‘good’ cholesterol because they can easily pass through the arteries and easily absorbed in the body unlike the ‘Low Density Lipoproteins’ also known as ‘bad’ cholesterol causes coronary heart problems. Lipoprotein(a) according to the reports of Jose, et al. [2]. Lipoprotein(a) is a risk factor for numerous cardiovascular diseases, when individuals are tested in the laboratory for high levels of lipoprotein(a), there is a likelihood of having coronary heart problems or heart attack, a stroke especially when also there is an elevated level of cholesterol or hypercholesterolemia [3].
Lipoprotein(a) is not a routinely ordered test. A National Cholesterol Education Program (NCEP) guideline, the Adult Treatment Panel-III acknowledged the possible usefulness of Lipoprotein (a) but it did not recommend widespread screening (National Cholesterol Education Program, 2001). The National Academy of Clinical Biochemistry (NACB) guidelines for emerging biomarkers of cardiovascular disease and stroke also recommend testing individuals with a strong family history of premature atherosclerotic heart disease and/or high lipid levels (hyperlipidemia) or those with intermediate cardiovascular risk, but do not recommend general screening.
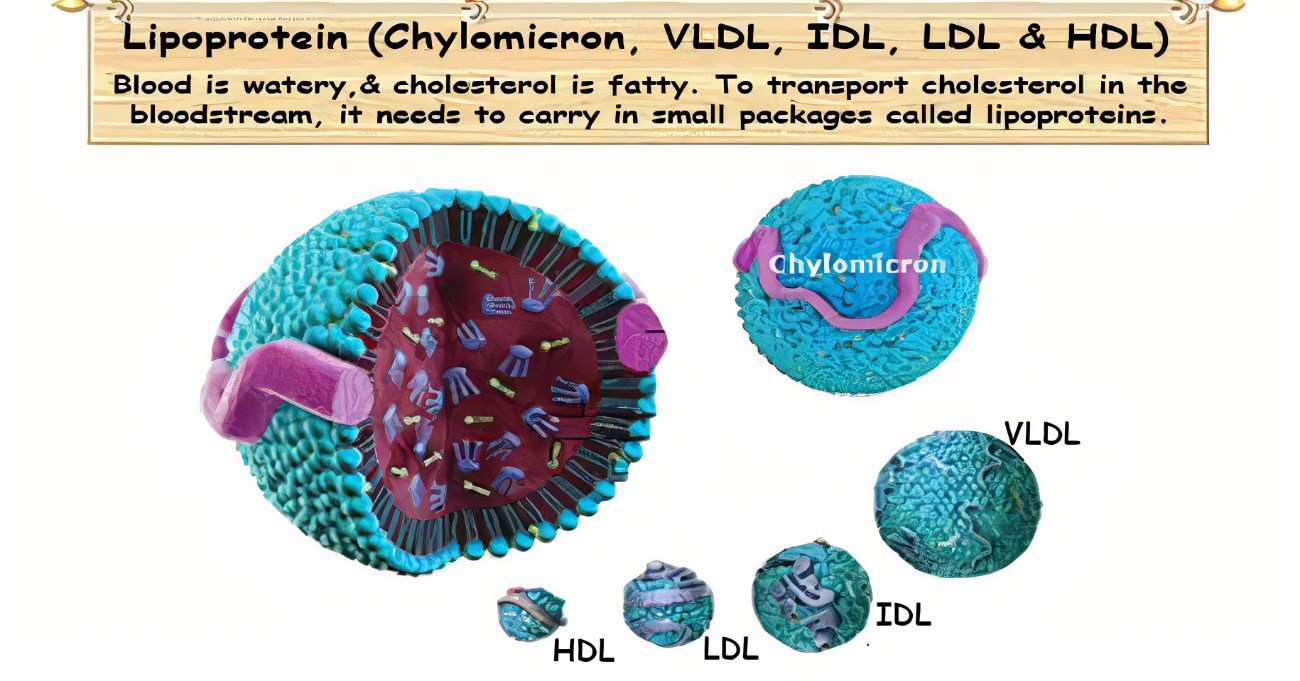
Rather, levels of Lipoprotein(a) are determined chiefly by the rate of de-novo hepatic synthesis (~5.0mg/Kg per day). Catabolic pathways may include dissociation of apo(a) from apo B100. Formation of differing molecular weight fragment and clearance largely by the kidney and spleen (Rank, 2001) within apo(a) is a unique region highly structurally homologous to plasminogen but devoid of protease activity. By competitively antagonizing plasminogen binding, Lipoprotein(a) may have played an ancestral role in hemostasis and wound healing at sites of arterial injury, attenuating fibrinolysis, promoting thrombosis/ coagulation and delivering cholesterol. Potential atherogenic effects may include arterial deposition of oxidized phospholipids by apo B. Structure of Lipoproteins
Overview of Biochemistry and Potential Pathophysiological Effects
Lipoprotein (a) includes a single molecule of apolipoprotein (apo) B100 covalently linked in a 1:1 molar ratio to apo (a). This unique glycoprotein-containing (hydrophilic) moiety is secreted by the liver. The 2 molecules are most likely complexed in the hepatocyte cellular membrane and are connected biochemically by a disulfide bridge through cysteine residues within apo(a)(Cys 45057) and apo B100 (Cys 4326) [4]. According to Tsimikas, et al. [5], when lipoprotein from a single molecule of an oxidized phospholipid such as apolipoprotein, this produces an inflammatory response that is measured with the principle and use of an antigen-antibody reaction that reflects the presence and the extent of obstructive coronary disease commonly known as a stenosis that is measured greater than fifty (50) percent of the luminal diameter.
Although Lipoprotein(a) contains an LDL-receptor binding region, the hepatic LDL receptor likely plays a negligible role in Lipoprotein(a) catabolism.
Source: Thirievelan, 2010.
Materials
In an experimental cross-sectional study carried out by Thirievelan [6]. One hundred and Sixty-five (n=165) subjects of both male and female were recruited in this study, out of which one hundred (Females=56 and Males=44) were diabetes type 2 patients and the remaining sixty-five non- diabetic patients (Females=37 and Males=28) were the control group. The study areas were the Braithwaite Memorial Hospital, BMH and the University of Port Harcourt Teaching Hospital, UPTH respectively. The diabetic individual’s blood samples were tested for levels of Lipoprotein (a). Glycemic index of each test control was measured, those that showed a glycated hemoglobin concentration greater than or equal to 6.5 was recruited for the study.
Methodology
- The diabetic individuals were placed on fasting overnight.
- Blood samples were tested for levels of Lipoprotein(a).
- The Lipoprotein(a) concentration was be measured quantitatively as described by the manual provided in the kit by Cloud- Clone Corporation laboratories, Houston Texas, United States of America purchased for the experimental procedure in the laboratory.
Principle
The Enzyme Linked Immunosorbent Assay employed a sandwiched enzyme immunoassay technique that measured human lipoprotein (a) [LP(a)] in less than 4 hours. A polyclonal antibody specific for human Lipoprotein(a) had been pre-coated onto a 96 well microplate with removable strips. Lipoprotein(a) in the standards and samples was sandwiched by the immobilized antibody and also with the biotinylated polyclonal antibody specific for Lipoprotein(a), which is recognized by a streptavidin-peroxidase conjugate. All unbounded material was washed away and a peroxidase enzyme substrate was added. The colour development was stopped and the intensity of the colour was measured spectrophotometrically at 450nm.
Methodology
- The reagents were brought to room temperature before use.
- The assay was performed at room temperature (20- 250C).
- The micro plate strips were removed from the plate frame to which 50µl of human Lipoprotein(a) standard and sample were added per well.
- The wells were covered with a sealing tape and incubated for 2 hours.
5. The timer was started, after the last addition; 200µl of wash buffer was used five times to wash maximally. 6. The plate was inverted each time and the content was decanted and hitted 4 to 5 times on an absorbent material to completely remove the liquid. 7. 50µl of streptavidin-peroxidase conjugate was added to each well and incubated for 30 minutes; the micro plate reader was turned on and the program set up in advance. 8. The micro plate was again washed and 50µl of chromogen substrate was added per well and incubated for 10 minutes until the blue colour intensity developed. 9. The plate was gently tapped to ensure thorough mixture of the wells, 50µl of stop solution was added to each well, the colour changed from blue to yellow and the absorbance of the micro plate was read at 450nm using a micro plate reader.
Calculations
ug Concerntraction of Lipoprotein(a)( )= ml Absorbanceof T Standard Absorbance of Standard est × Concentration of By this method the expected reference range for the determination of serum lipoprotein(a) is (374.24-443.46ug/ ml)
Results
P value < 0.0001
20000 C ontrol
D iabetic S ubjects
15000 L P I
10000
5000
0 C o n tro l D iab e tic S u b je cts Figure 1: Graph showing Levels of Lipoprotein against the diabetic subjects and their control counterparts.
Discussion
Lipoprotein(a) is the newest risk factor for the assessment of individuals who are at risk of having cardiovascular diseases as growing interest with this marker is being focused on the association of coronary artery diseases as well as atherosclerosis most especially with individuals suffering from type 2 diabetes mellitus. In this present study, the results from Figure 1 above showed significant increase in lipoprotein(a) levels in the diabetic individuals when compared to that of the control subjects (p<0.05), this is in agreement with the work done by Brown, et al. [7]. Although with these assessments, individuals can also be monitored with lipoprotein which is a more predictive index assessor for cardiovascular disease than the conventional lipid profile indexing used in diagnostic laboratories where individuals diagnosed with high levels of lipoprotein(a) are proffered with treatments to alleviate further damages to the cardiovascular tissues in its entirety.
Conclusion
From the above results, it is pertinent that lipoprotein levels revealed a strong and graded association with the presence and extent of possibilities of coronary disease as well as a predictive marker to enhance treatment modalities especially with type 2 diabetes individuals as compared also with the levels of lipoprotein with the healthy control subjects. However further work may enhance a better predictive model than lipoprotein in future research.
References
-
Vaduganathan M, Mensah G, Turco J, Valentin F, Gregory AR (2022) The Global Burden of Cardiovascular Diseases and Risk. Journal of American College of Cardiology 80(25): 2361-2371.
-
Jose LS, Nathan DW (2022) Lipoprotein(a): Evidence for Role as a Casual Risk Factor in Cardiovascular Disease and Emerging Therapies. J Clin Med 11(20): 6040.
-
Kampstrup PR, Anne T, Rolf R, Nordestgaard G (2009) Genetically Elevated Lipoprotein(a) and Increased Risk of Myocardial Infarction. JAMA 301(22): 2331-2339.
-
Siekmeier R, Marz W, Feussner G, Donnerhak B, Schaaf L, et al. (2010) Apolipoprotein E to B ratio; a marker for Type III Hyperlipoproteinaemia. Eur J Clin Biochem 31(11): 743-747.
-
Tsimikas S, Emmananouil S, Elizabeth RB, Miller BS, Joseph P, et al. (2005) Oxidized phospholipids, Lp(a) lipoprotein, and coronary artery disease. N Engl J Med 353(1): 46-57.
-
Thirievelan (2010) Structure of Lipoproteins.
-
Brown H, Joshua MT (2016) Diagnostic Value of Homocysteine, Cystatin C and Lipid Indices in Assessment of Cardiovascular Risk Status of Patients with Diabetes Type 2. European Journal of Preventive Medicine 4(3): 79-84.
-
National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (2001) Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel of Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 285(19): 2486-2497.
-
Frank HZ, Parse J (2001) A 27-year Follow-Up of Patients with borderline Personality Disorder. Compr Psychiatry 42(6): 482-887.
-
Rank A (2001) Lipoprotein and Coronary Artery Disease. The New England Journal of Medicine 353: 46-57.
- An Efficient and Affordable Method for Isolating Bone Marrow- Derived Mesenchymal Stem Cells from Swiss Albino Mice
- Superposition of Cryo-EM and AlphaFold Predictions of Dengue Antigen-Antibody Complexes
- Jugular-Applied Coherent Low-Level Laser Therapy Enhances Systemic Mitochondrial Metabolic Function and Antioxidant Response
- Role of OMC32 Polypeptide in Acrosin-Mediated Exocytosis during the Bovine Sperm Acrosome Reaction
- Association of Galectin-3 but not Laminin in Tamoxifen-Induced Growth Suppression in Breast Cancer MCF-7 Cells
- Effect of Different Wavelengths of Light on the Rate of Photosynthesis