Goblet Cell Carcinoid of Appendix: Report of Two Cases and Review of Controversial Aspects
Goblet cell Carcinoid is a rare type of appendix tumor that constitutes 14% of malignant appendix neoplasms. Management of these lesions is a challenge; there are many controversial points and, until now, no consensus has been achieved. They are stemmed from pluripotential cells placed on intestinal crypt base, as a result, they are hybrid tumors with mucinous and neuroendocrine differentiation. This peculiar feature becomes them into a heterogeneous group that requires special attention. According to WHO, they are considered a subtype of mixed adenoneuroendocrine carcinoma, under neuroendocrine category. Tang described three hystological types, group A, B and C, based on presence of goblet cells, signet ring cells and carcinoma component, as long as architecture and pattern of distribution. Although, it is generally accepted that their behavior is intermediate between Carcinoid and adenocarcinoma, prognosis is related to Tang's groups and TNM (7th edition). Recently, some studies have pointed that goblet cell Carcinoid is a peritoneal disease, and treatment should include hyperthermic intraoperative peritoneal chemotherapy, for this purpose, patients should be referred to centers of excellence. We report two cases of goblet cell Carcinoid, group A and B, and review controversial aspects.
Background
Malignant tumors of appendix account for less than 1% of all malignant gastrointestinal tumors. They are classified into colonic adenocarcinoma, mucinous adenocarcinoma and neuroendocrine [1]. According to SEER database, mucinous adenocarcinoma is the most common lesions (37%), followed by colonic adenocarcinoma (35-27%), malignant carcinoid (11- 30%), goblet cells carcinoid (14-19%) and signet ring cell carcinoma (4-6%) [2]. Goblet cell carcinoid (GCC) is a rare entity. The incidence of these tumors is 0.005% per
100.000 habitants. They constitute 14% of all malignant appendix tumors and they are identified in 0.3-0.9% of specimens after appendectomy [3, 4, 5]. They most occurr in caucasians with mean age of 52 years old and no differences in gender have been reported. GCC classification has been matter of debate for years, and a great variety of terms have been used to refer to these tumors. In 2010, WHO determined that GCCs are a subtype of mixed adenoneuroendocrine carcinoma (MANEC) and consequently, they are under neuroendocrine category [6]. In general, it is accepted that their behavior is more aggressive than neuroendocrine and show better prognosis than adenocarcinoma [4]. Their origin is also motive of controversy. Different theories have been postulated. Warner suggested that they stem from a pluripotent cell placed on a crypt base with multidirectional differentiation, and as a result, GCCs are hybrid tumors with two components: neuroendocrine and glandular [1]. Surgery is the gold standard treatment; however, it is surrounded by several dilemmas. Whether an appendectomy alone is an adequate treatment is still questioned. Some centers recommend right hemicolectomy for all GCCs; however, others highlight that GCC is a peritoneal disease and right hemicolectomy should be performed only in selected cases. Similarly, HIPEC should be considered in some cases, and always in centers of excellence [1, 4]. We report two cases of goblet cell carcinoids: group A and B, and review management and controversial points.
Case Report
Case 1
A 64-year male with a two-week history of lower right abdominal pain was admitted to General Surgery Department. He also referred fever and asthenia. His medical history included hypertension, chronic obstructive pulmonary disease, smoking and daily intake of 50 grams of alcohol. The patient was apyrexial and hemodynamically stable. During physical examination, a painful tender mass was palpable in the lower right area with no rebound. Routine blood test showed a mild leukocytosis of 12.5•10^9/L with a neutrophilia of 10.5•10^9/L. A CT was performed and revealed an appendicular mass with fat stranding and periappendicular fluid collection (4x2 cm in size) (Figure 1). The patient underwent laparoscopic appendectomy. A perforated appendix with periappendicular abscess was found. Appendectomy and drain were carried out. The postoperative period was uneventful and the patient was discharged 5 days later.

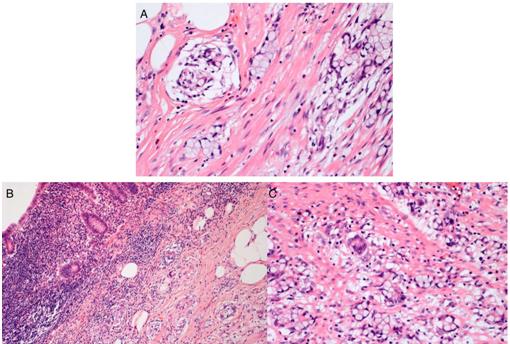
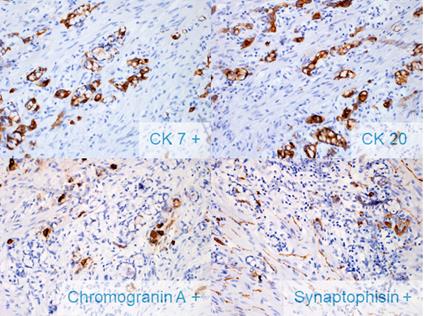
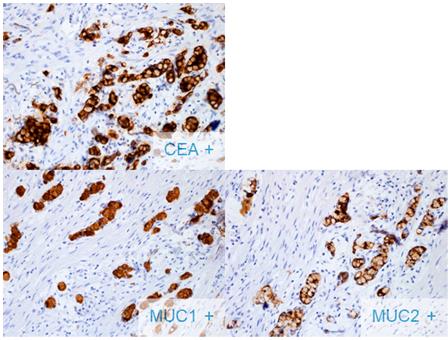
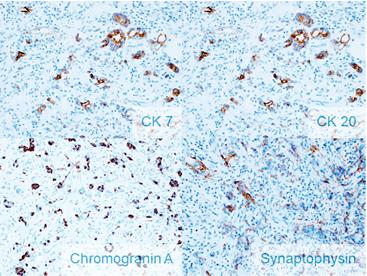
Figure 1: CT shows appendix mass surrounded by fat- stranding, periappendiceal abscess and appendicolith. Some reactive lymph nodes are identified. The appendix showed a length of 4.5 cm and 1 cm in diameter. Frozen biopsy revealed a goblet cell carcinoid with goblet cells arranged in cohesive clusters, no desmoplasia and minimal cytological atypia. Perineural and perivascular infiltration were also found (Figure 2). Immunohistochemistry was performed and demonstrated immunoreactivity for cytokeratin 20, cytokeratin 7 and CEA; andfocal positivityfor endocrine markers (chromogranin A or synaptophysin) (Figure 3). In addition, goblet cells displayed preserved immunoreactivity for MUC1 and MUC2, which is not the common pattern for typical goblet cell carcinoid. Also, P53 was positive in 5-10% of tumoral cells (Figure 4). In conclusion, the patient was diagnosed of GCC group A, T3N0Mx. After surgery, colonoscopy and thoracoabdominal CT were performed. Neither of them revealed distant metastases. Tumoral markers (CEA, CA- 125 and CA-19.9) were within normal ranges. Eventually, the patient underwent right hemicolectomy. Histological study demonstrated neither tumoral cells nor affected lymph nodes. Adjuvant FOLFOX regimen was considered. Currently, the patient is under chemotherapy and doing well.
Case 2
A 56 year male presented to General Surgery Department with a three-day history of lower right abdominal pain, vomits and low-grade fever. His medical history was unremarkable. Physical examination revealed pain on palpating at lower right quadrant, McBurney's and Rousing's signs were positive. On blood test, leukocytosis (14•10^9/L) with 90% neutrophilia was present. With the diagnosis of acute appendicitis, the patient underwent urgent surgery. A perforated appendix on the tip was found and laparoscopic appendectomy performed. The patient was discharged 48 hours later.
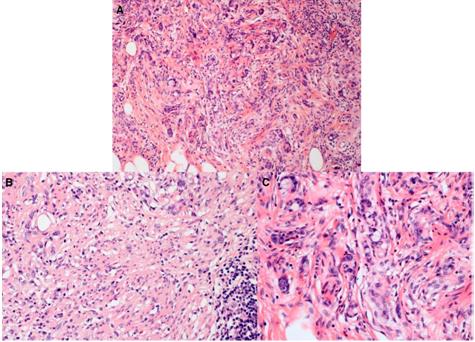
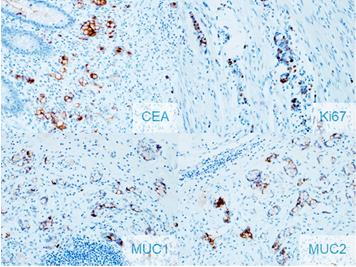
Frozen biopsy revealed a goblet cell carcinoid group B with goblet cells or signet cells arranged in a disorganized pattern, and foci of typical GCC (group A), with atypia and desmoplasia (Figure 5). When immunohistochemistry was made, it revealed stain for cytokeratin 20 and cytokeratin 7, beside focal reactivity for endocrine markers (chromogranin A and synaptophysin) (Figure 6). The proliferation index, Ki-67, was 30%, with MUC 1 and MUC2 preserved and positive reactivity for CEA (Figure 7). Moreover, the base of the appendix was infiltrated by tumoral cells. Neither perineural nor perivascular invasion were found. Finally, with the diagnosis of CGG group B, T3N0Mx, colonoscopy and thoracoabdominal CT were performed, as long as tumoral markers. No distant metastases were found and the patient underwent laparoscopic right hemicolectomy. The postoperative period was uneventful and was discharged 6 days later. The histological study of specimen did not show tumoral cells, and lymph nodes were not affected.
Discussion
Goblet cell carcinoid is considered a rare entity with an incidence rate of 0.01– 0.05 /100.000/ year, affecting both genders equally. According to SEER (Surveillance, Epidemiology and End Results) database, they are more common in Caucasians in their sixth decade [5]. GCCs show neuroendocrine and adenocarcinoma features. Therefore, their classification has been matter of debate for years. They are characterized by goblet-shaped cells, containing mucin, that cluster in the lamina propia of submucosa. Most of them are larger than 2 cm [7]. In the past, the terms mucinous carcinoid tumor, mixed crypt cell carcinoma, adenocarcinoid-goblet cell type and microglandular goblet cell type were used for describing these tumors [1, 8]. In 1969, Gagne was the first to describe three cases of tumor of appendix that displayed characteristics of carcinoid and adenocarcinoma. Later, in 1974, Subuswamy described 12 cases and coined the term goblet cell carcinoid. Eventually, Warkel reported a series of 39 cases and suggested that GCC tumors had a behavior between carcinoid and adenocarcinoma [9]. In 2008, Tang et al. published a series of 63 GCCs of appendix, and divided these tumors into three groups according to histological findings: Group A or typical GCC: goblet- shaped epithelial cells cluster and invade submucosa, and, on occasions, muscularis propria and subserosa; however, mucosa is unaffected. Cells show a cohesive architecture. They display minimal atypia and mitoses are scarcely identified. Sometimes, extracellular mucin can be identified. Group B or adenocarcinoma ex GCC or signet ring cell type: goblet or signet cells grow in an irregular and discohesive pattern. Atypia, desmoplasia and destruction of the wall of the appendix are typical features of this group. Group C or adenocarcinoma ex GCC, poorly differentiated adenocarcinoma type: they are the most infrequent tumor occurring only in 11% of all GCCs. These tumors show typical GCC and in addition, a foci, of at least 1 mm2, of poorly differentiated adenocarcinoma (glandular, confluent sheets of signet ring cells or undifferentiated carcinoma) [10]. The adenocarcinomatous component has impact on prognosis. Burke et al. suggested that when it constitutes more than 50% of the tumor, the prognosis is poor. Conversely, the probability of metastasis is low when adenocarcinomatous component is less than 25%. Similarly, Melissa studied 142 cases and concluded that adenocarcinomatous component is associated with clinical features, stage and survival [8]. According to these studies, GCCs represent a group of tumors with heterogeneous behavior related to their histological features. Although, they are usually considered to have a better prognosis than adenocarcinomas, when adenocarcinomatous component is higher than 50% they should be treated as adenocarcinoma [8]. In 2010, the World Health Organization (WHO) classified these tumors as neuroendocrine based on grade and differentiation. Grade is defined by mitotic activity and Ki67 index, and subdivided into G1-low grade (< 2 mitosis/ 10 HPF and ≤ 2% Ki index), G2-intermediate grade (2-20 mitosis/10 HPF, 3%-20% Ki index) and G3- high grade (> 20 mitosis/10 HPF, > 20% Ki index). However, the role of Ki- 67 on prognosis is uncertain, and most cases show a low Ki-67 index [1, 7]. In addition, these tumors are called well differentiated when cells resemble normal neuroendocrine cells (G1, G2), otherwise they are poorly differentiated (carcinomas, G3). GCC are a rare subtype of mixed adenoneuroendocrine carcinoma (MANEC) and, according to this, at least 30% of GCC tumor must show glandular component and other 30% neuroendocrine component. However, this cut-off may be lower in advanced stages where poorly differentiation prevails (group C) [1, 11]. On the other hand, TNM classification (7th edition) must be also taken into account when classifying these tumors, based on size, nodes and metastases [12]. Pathogenesis of GCC remains uncertain. The sequence of adenocarcinomatous-carcinoma, accepted for adenocarcinomas of colon and appendix, does not seem to play a role at these tumors. The absence of dysplasia or preinvasive lesions at GCC supports this theory [13]. GCC could arise from pluripotential cells located in the intestinal crypt. It was in 1974, when Cheng described the crypt based columnar cells as intestinal stem cells [1, 14]. These stem cells differentiate as enterocyte, goblet cell, neurone doctrine and Paneth cells. Although the knowledge of goblet cells is limited, recently some studies have suggested that goblet cells would have a relevant role in interacting with immune system presenting oral antigens [15]. The goblet cells at GCC are larger than normal goblet cells. Different signalling pathways participate in the proliferation cycle of these cells (Wnt, Notch, Ephephrin and Math 1) [1]. Consequently, mutations at these crucial pathways cause an uninhibited proliferation and loss of regulated inhibition. Allelic losses of chromosomes 11q, 16q and 18q have been reported. Contrarily, mutations of KRAS or BRAF have not been found. Some authors suggest that p53 mutation is decisive for the development of GCC, however, others have failed to demonstrate this. Naoto reported a reduced expression of E-Catherine and preserved expression of B-catenins [16]. In conclusion, alterations of the proliferation of pluripotential intestinal cells would cause an uncontrolled growth of goblet and neuroendocrine cells that would explain the hybrid nature of GCC [1, 10, 13]. Immunohistochemistry of GCC is peculiar and does not follow ordinary patterns of carcinoid. Most GCCs show an inconsistent reactivity for neuroendocrine markers. On this way, chromogranin A and synaptophysin are focally positive. Other markers as CEA, CDX-2, CAM5.2 and CK20, CK 7 and CK19 are more evident in immunohistochemistry [4]. Tang reported negativity for MUC1 and preserved staining for MUC2 at groups A and B. Conversely, group C displayed expression of MUC1 and loss of MUC2 [10]. Pathogenesis of GCC supports that they are an entity completely different from carcinoid and adenocarcinoma, and therefore they require especial evaluation and understanding. Expression of somatostatin receptors is erratic and scattered; therefore 111-Indium pentetreotide scintigraphy (Octreoscan) and Gallium 68 octreotide positron emission tomography have a limited use. The vast majority of patients present symptoms of acute appendicitis, especially when located in the mid third of the appendix. However, approximately a third of patients maybe be asymptomatic and GCC diagnosed as an incidental finding on surgery performed by other reasons [1, 5]. Krukenberg tumor in the ovaries has also been reported, occurring in up to 80% of women at stage IV [1, 7, 10]. Perforation presents in 16% of all appendectomy, and this is a concern when facing GCCs: does perforation imply a higher possibility of metastases? The literature demonstrates that perforation of appendix carcinoid lacks prognostic impact. On the contrary, perforation could be a major concern in GCC. However, the association with peritoneal carcinomatosis remains uncertain. Approximately 80% GCCs are presented as perforated appendicitis [6, 7]. Furthermore, peritoneal spread is frequent at diagnosis, occurring in 72% of all patients. Conversely, only approximately 50% present lymph node metastases. In conclusion, GCC must be considered a peritoneal disease [17]. Distant metastases at liver, bone and lung have also been reported [13]. Carcinoid syndrome and 5HIAA levels are usually in normal range. Management is also controversial: appendectomy alone versus right hemicolectomy has been evaluated in many studies. Some meta-analysis have proved benefits of appendectomy alone when tumor is T2 or less, with no cecal involvement and low-grade [18, 19]. On the other hand, centers of excellence have reported benefits of cytoreductive surgery and Hyperthermic Intraoperative Peritoneal Chemotherapy (HIPEC) in selected patients. Recently, Lamarca has published a series of 97 patients treated in a reference center (Manchester, UK) and concluded GCC treatment should be focused on peritoneal cavity (cytoreductive surgery and HIPEC) rather than on local treatment (right hemicolectomy). Appendectomy alone should be considered for tumors of group A, T1 or T2, with no radiological evidence of metastases or lymph node spread. For the rest of cases, cytoreductive surgery and HIPEC should be considered in reference centers, and the need of performing a right hemicolectomy at this time individualised. Also, female patients should undertake bilateral oophorectomy. Adjuvant chemotherapy (FOLFOX) should follow cytoreductive surgery and HIPEC [7]. On the other hand, North American Neuroendocrine Tumor Society and ENETS recommend a prophylactic right hemicolectomy for all GCCS in order to reduce risk of metastases [5, 20]. However, according to SEER database, only 42% of patients undertook right hemicolectomy [5]. The two patients treated in our center, undertook right hemicolectomy and adjuvant chemotherapy. Although our center provide HIPEC for other tumors, they were not considered candidates for this procedure because of lack of consensus and ausence of factors of risk. Surveillance is also a controversial point. Most authors recommend tumoral markers and image technique (CT) every 3-6 months. Conclusion To summarise, GCC is a rare subtype of MANEC, and belongs to neuroendocrine tumour category. Albeit, its classification has been matter of debate for decades, we strongly recommend to use Tang's classification (group A,B and C) and also TNM 7th edition. Pathogenesis is based on uncontrolled growth of pluripotent cells located at crypt base as consequence of mutations affecting pathway signals. As a result, a hybrid tumour is originated. Therefore, tumoral cells display neuroendocrine and adenocarcinoma features, and this concept distinguishes them from carcinoids. They are more aggressive than ordinary carcinoids. The role of p53 mutation and Ki-67 index are uncertain and numerous papers have been published with different theories. GCCs show a peritoneal spread similar to mucinous neoplasms, and consequently, patients should be referred to specialized centers to consider cytoreductive surgery and HIPEC. Although right hemicolectomy has been recommended for all GCCs, recently, Lamarca failed to evidence benefit for all GCCs. Currently, more studies are required to achieve consensus in management, based on TNM and Tanger classification.
Consent of Patient
Written informed consent was obtained from the patient.
References
-
Shenoy S (2016) Goblet cell carcinoids of the appendix: Tumor biology, mutations andmanagement strategies. World J Gastrointest Surg 8(10): 660-669.
-
Brathwaite S, Yearsley MM, Saab TB, Wei L, Schmidt CR, et al. (2016) Appendiceal Mixed Adeno- Neuroendocrine Carcinoma: A Population- Based Study of the Surveillance, Epidemiology, and End Results Registry. Front Oncol 6: 148.
-
Rossi R E, Luong TV, Caplin ME, Thirlwell C, Meyer T et al. (2015) Goblet cell appendiceal tumors-- management dilemmas and long-term outcomes. Surg Oncol 24(1): 47-53.
-
Clift AK, Frilling A, Frilling (2017) Neuroendocrine, goblet cell and mixed adeno-neuroendocrine tumours of the appendix: updates, clinical applications and the future. Expert Rev Gastroenterol Hepatol 11(3): 237-247.
-
Pape UF, Perren A, Niederle B, Gross D, Gress T, et al. ( 2012) ENETS Consensus Guidelines for the management of patients with neuroendocrine neoplasms from the jejuno-ileum and the appendix including goblet cell carcinomas. Neuroendocrinology 95(2): 135-156.
-
Madani A, van der Bilt JD, Consten EC, Vriens MR, Borel Rinkes IH, et al. (2015) Perforation in appendiceal well-differentiated carcinoid and goblet cell tumors: impact on prognosis? A systematic review. Ann Surg Oncol 22(3): 959-965.
-
Lamarca A, Nonaka D, Lopez Escola C, Hubner RA, O Dwyer S, et al. (2016) Appendiceal Goblet Cell Carcinoids: Management Considerations from a Reference Peritoneal Tumour Service Centre and ENETS Centre of Excellence. Neuroendocrinology 103(5): 500-517.
-
Taggart MW, Abraham SC, Overman MJ, Mansfield PF, Rashid A, et al. (2015) Goblet cell carcinoid tumor, mixed goblet cell carcinoid- adenocarcinoma, and adenocarcinoma of the appendix: comparison of clinicopathologic features and prognosis. Arch Pathol Lab Med 139(6): 782- 790.
-
Roy P, Chetty R (2010) Goblet cell carcinoid tumors of the appendix: An overview. World J Gastrointest Oncol. 2(6): 251-258.
-
Tang LH, Shia J, Soslow RA, Dhall D, Wong WD, et al. (2008) Pathologic classification and clinical behavior of the spectrum of goblet cell carcinoid tumors of the appendix. Am J Surg Pathol 32(10): 1429-1443.
-
Bosman FT, Carneiro F, Hruban RH, Theise ND ( 2010) WHO classification of tumours of the digestive system. World Health Organization.
-
Cancer AJCO (2010) AJCC Cancer Staging Manual, 7th (Edn.), DRB Stephen B. Edge, Carolyn C. Compton, April G. Fritz, Frederick L. Greene, Andy Trotti III. 2010 (Eds.).
-
Pahlavan PS, Kanthan R (2005) Goblet cell carcinoid of the appendix. World J Surg Oncol 3: 36.
-
Cheng H, Leblond C (1974) Origin, differentiation and renewal of the four main epithelial cell types in the mouse small intestine V. Unitarian theory of the origin of the four epithelial cell types. American Journal of Anatomy 141(4): 537-561.
-
Pelaseyed T, Bergstrom JH, Gustafsson JK, Ermund A, Birchenough GM, et al. (2014) The mucus and mucins of the goblet cells and enterocytes provide the first defense line of the gastrointestinal tract and interact with the immune system. Immunol Rev 260(1): 8-20.
-
Kuroda N, Mizushima S, Guo L, Jin Y, Tao L, et al. (2001) Goblet cell carcinoid of the appendix: Investigation of the expression of beta-catenin and E-cadherin. Pathol Int 51(4): 283-287.
-
Radomski M, Pai RK, Shuai Y, Ramalingam L, Jones H, et al. (2016) Curative Surgical Resection as a Component of Multimodality Therapy for Peritoneal Metastases from Goblet Cell Carcinoids. Ann Surg Oncol 23(13): 4338-4343.
-
Varisco B, McAlvin B, Dias J, Franga D (2004) Adenocarcinoid of the appendix: is right hemicolectomy necessary? A meta-analysis of retrospective chart reviews. Am Surg 70(7): 593- 599.
-
Pham TH, Wolff B, Abraham SC, Drelichman E (2006) Surgical and chemotherapy treatment outcomes of goblet cell carcinoid: a tertiary cancer center experience. Ann Surg Oncol 13(3): 370-376.
-
Boudreaux JP, Klimstra DS, Hassan MM, Woltering EA, Jensen RT, et al. (2010) The NANETS consensus guideline for the diagnosis and management of neuroendocrine tumors: well-differentiated neuroendocrine tumors of the Jejunum, Ileum, Appendix, and Cecum. Pancreas 39(6): 753-766.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review