Double Whammy: Severe Necrotizing Soft Tissue Infection in the Setting of Extra Peritoneal Bladder Injury from Prolonged Urinary Bladder Catheterization
Urinary bladder injury due to prolonged indwelling Foley catheter placement is reportedly rare but potentially lethal complication. Review of literature showed most of the urinary bladder injuries reported was intraperitoneal. This is the first reported case of extra peritoneal bladder injury causing severe necrotizing soft tissue infection of the lower abdomen and groin area. The patient was initially managed by surgical debridement of infected soft tissue, IV antibiotics and indwelling Foley catheter. The extra peritoneal bladder injury eventually required surgical repair of the perforated site and open wound managed with negative pressure dressing. The patient was discharged from the unit after a course of antibiotics which helped clear the infection.
Introduction
Perforation of the urinary bladder due to long term indwelling catheter is a rarely reported but potentially lethal complication with mortality rate as high as 50% [1]. The Centers for Disease Control estimates that roughly 12-25% of long-term hospitalized patients will have a Foley catheter. Growing geriatric population can lead to increase in chronic urinary catheterization making them at risk for possible urinary bladder perforation [2]. Majority of urinary bladder perforation from this etiology is intraperitoneal and managed operatively. Extraperitoneal bladder injury is typically managed conservatively with indwelling foley catheter, empiric antibiotics, and analgesics and follow-up cystogram in 7 to 10 days prior to Foley removal. This is the first case report on an extraperitoneal bladder injury complicated by severe necrotizing soft tissue infection.
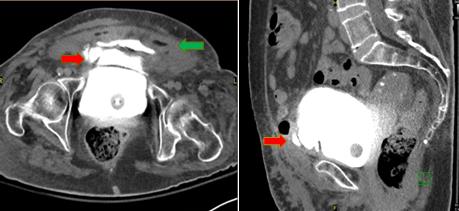
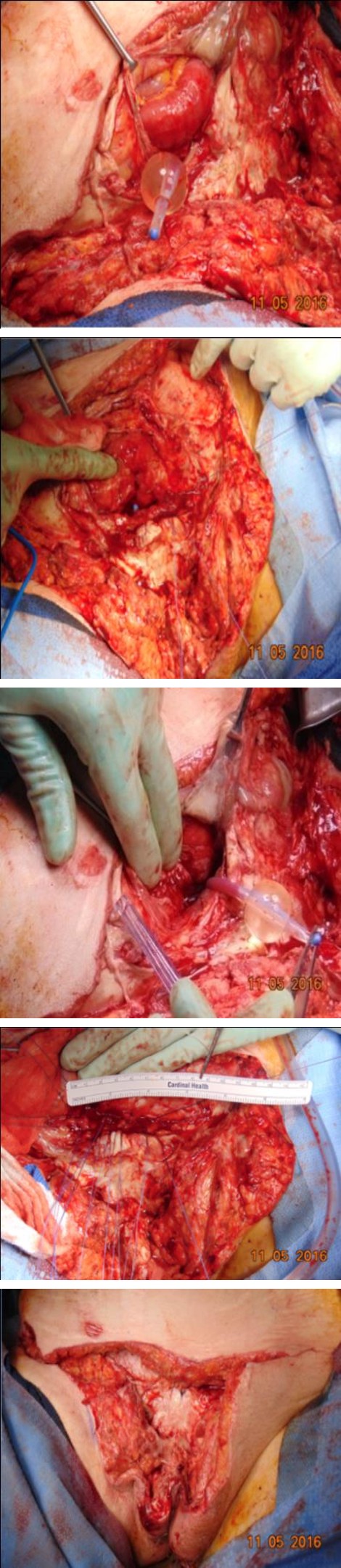
This is a case of an 83-year-old lady with past medical history of CVA, diabetes mellitus, hypertension and hypothyroidism who developed cystitis with longstanding indwelling catheter. Foley catheter was replaced at a nursing home and she eventually developed severe abdominal pain. She was transferred and admitted to the Internal Medicine Service and subsequently referred to the Urology Service. She was treated with indwelling foley catheter and broad spectrum antibiotics. After 4 days, the patient developed cellulitis and was referred to the Acute Care Surgery service. A CT cystogram was requested which showed extraperitoneal bladder injury with extensive soft tissue edema concerning for necrotizing soft tissue infection (Figure 1). Decision was made to go to the OR for wound exploration. She was noted to have severe necrotizing soft tissue infection of the lower abdominal wall extending to the mons pubis (Figure 2). The Patient was admitted to the Surgical Intensive Care Unit post-operatively. Re-exploration of the wound three days after the first operation revealed infection of the fascia requiring excisional debridement which exposed the 7 cm extraperitoneal bladder perforation. This was repaired in layered fashion using Vicryl sutures (Figure 3). Five days after, the patient underwent re-debridement and eventual VAC dressing. Wound culture grew Bacteroides, Pseudomonas and Enterococcus faecium. The patient was kept on broad spectrum antibiotics per sensitivity for 10 days. She was discharged to a rehabilitation facility 13 days after the original operation. The wound was successfully managed using negative pressure dressing and completely healed after 8 weeks (Figure 4). The foley catheter was removed after a negative cystogram.
Discussion
Foley catheter insertion is a common medical procedure and can cause some complications including no other associated injury requiring surgical intervention. Extraperitoneal injury is treated with foley catheter and follow up cystogram. Review of literature showed that presence of other medical conditions such as diabetes mellitus, advanced age, immunocompromised state, uterine fibroids, infection, appendicitis, urinary bladder neoplasm, and pelvic radiation predisposed patients with chronic indwelling foley catheter to urinary bladder perforation [5, 6, 7]. Spontaneous rupture of the urinary bladder had been reported but other risk factors can contribute to the rupture including blunt trauma to the lower abdomen, cancer of the pelvic organ, irradiation, bladder tumor, large uretero-vesical stone, urethral or suprapubic catheterization, postpartum, atonic bladder, previous laparotomy, iatrogenic from saline irrigation, and binge alcohol intake[4]. The exact mechanism on why perforation occurs in chronic foley catheter placement is uncertain. In vivo experiment by G. Miles showed that negative pressure exerted on untrained column of urine in the drainage tubing sucks the bladder mucosa in the proximal orifices of the catheter causing formation of hemorrhagic pseudo-polyp within 10 minutes of catheter insertion [8, 9]. We believe that our patient, having been predisposed to necrotizing soft tissue infection by her diabetic state, may have developed necrosis of the bladder that leads to the perforation. Delay in appropriate management of necrotizing soft tissue infection and bladder perforation carries a high rate of morbidity and mortality. For this reason, patients with bladder High index of suspicion for perforated bladder injury should be considered on elderly patients with chronic catheterization presenting with abdominal pain. Necrotizing soft tissue infection can occur concomitantly with bladder injury and aggressive and early debridement should be done. More recent cases have shown that intraperitoneal bladder injures can be repaired using the laparoscopic method. However, both of these cases were performed in stable patients without any bladder neck injury [11, 12]. Therefore, we would not recommend using laparoscopic repair in complicated bladder rupture cases. In general, patients who are suspected to have a bladder rupture should be admitted to the surgery service to ensure complications are identified and handled in a timely fashion.
perforation even those managed non-operatively, should be admitted to the surgical team to prevent delay in surgical management should it be deemed necessary. Bladder perforation can be prevented by avoidance of catheterization and timely discontinuation of foley catheter if possible. Alternative methods like intermittent catherization and supra-pubic catherization should also be considered [10]. However, in patients with coexisting diabetes supra-pubic catheterization may not be appropriate since there is a risk for developing severe soft tissue infection.
Conclusion

References
-
Paul AB, Simms L, Paul AE, Mahesan AA, Ramzanali A (2016) A Rare Cause of Death in a Woman: Iatrogenic Bladder Rupture in a Patient with an indwelling Foley Catheter. Urol Case Rep 6: 30-32.
-
Ogawa S, Date T, Muraki O (2013) Intraperitoneal urinary bladder perforation observed in a patient with an indwelling urethral catheter. Case Rep Urol 765704.
-
Magee GD, Marshall SG, Wilson BG, Spence RA (1991) Perforation of the urinary bladder due to prolonged use of an indwelling catheter. Ulster Med J 60(2): 237-239.
-
Saleem MA, Mahmoud AM, Gopinath BR (2009) Spontaneous urinary bladder rupture: a rare differential for lower abdominal pain in a female patient. Singapore Med J 50(12): 410-411.
-
Huffman JL, Schraut W, Bagley DH (1983) Atraumatic perforation of bladder. Necessary differential in evaluation of acute condition of abdomen. Urology 22(1): 30-35.
-
Fujikawa K, Yamamichi F, Nonomura M, Soeda A, Takeuchi H (1999) Spontaneous rupture of the urinary bladder is not a rare complication of radiotherapy for cervical cancer: report of six cases. Gynecol Oncol 73(3): 439-442.
-
Stojadinovic MM, Mitrovic S, Milovanovic DR (2012) Micropapillary carcinoma of the bladder presented with spontaneous intraperitoneal bladder rupture. Can Urol Assoc J 6(2): 42-45.
-
Milles G (1965) Catheter-Induced Hemorrhagic Pseudo polyps of the Urinary Bladder. JAMA 193(11): 968-969.
-
Feneley RC, Hopley IB, Wells PN (2015) Urinary catheters: history, current status, adverse events and research agenda. J Med Eng Technol 39(8): 459-470.
-
Margolin DJ, Gonzalez RP (2004) Retrospective analysis of traumatic bladder injury: does suprapubic catheterization alter outcome of healing? Am Surg 70(12): 1057-1060.
-
Karadag CA, Tander B, Erginel B, Dilek Demirel, Unal Bicakci, et al. (2016) Laparoscopic repair in children with traumatic bladder perforation. J Minim Access Surg 12(3): 292-294.
-
Marchand TD, Cuadra RH, Ricchiuti DJ (2012) Laparoscopic repair of a traumatic bladder rupture. JSLS 16(1): 155-158.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review