Comparison of CD and DSA in Diagnosing PVD
Abstract Introduction: Peripheral arterial disease is the most common condition affecting the arteries of lower extremity. Aims and Objectivesï‚· To compare the CD and DSA in diagnosing PVD.ï‚· An attempt to define whether CD is an alternative or an adjunct to DSAï‚· Can CD replace DSA in diagnosing PVï‚· To evaluate the abnormalities of vascular disease with using color Doppler and digital subtraction angiographyï‚· To compare the findings color Doppler and digital substraction angiography.ï‚· Association of risk factorsï‚· Localization of flow obstruction in peripheral vesselï‚· Identification of type and length of stenosis/ occlusionï‚· Grading of stenosisï‚· Evaluation of post occlusive out flow tractMaterial and Method Study Design: Cross sectional Prospective study. Study Period: September 2015 to Jan 2017. Conclusion: Elderly people are with increased risk of peripheral arterial disease. Males are more commonly affected with smoking as the commonest risk factor. The other common risk factors include diabetes and hyperlipidemia. The commonest site of pathology is femoro-popliteal segment. Based on the above findings we in the inference that Color Doppler is an initial investigation of choice in evaluation of peripheral vascular diseases especially in infragenicularpart, and is an adjunct to DSA, but cannot replace it.
Biswas Som1* and Biswas Srirupa2
GRMC, Gwalior, India, E-mail: sombiswas4@gmail.com
Aims and Objectives
• To compare the CD and DSA in diagnosing PVD.
• An attempt to define whether CD is an alternative or an adjunct to DSA
• Can CD replace DSA in diagnosing PV
• To compare the findings color Doppler and digital substraction angiography.
• Association of risk factors
- Localization of flow obstruction in peripheral vessel
- Identification of type and length of stenosis/ occlusion
- Grading of stenosis
- Evaluation of post occlusive out flow tract Material and Method Study Design: Cross sectional Prospective study.
Study Period: September 2015 to Jan 2017.
and is an adjunct to DSA, but cannot replace it.
Keywords: CD; DSA; PVD
Introduction
Peripheral arterial disease is the most common condition affecting the arteries of lower extremity [1]. Compromise of arterial flow due to stenosis and occlusions can result in limb ischemia, which may manifest as claudication, rest pain, local tissue loss (ulceration), and, potentially, amputation. Patients with PAD may have symptoms but can also be asymptomatic [2]. These patients have an increased risk of mortality, myocardial infarction and stroke. It is an independent risk factor for vascular disease in other regions, resulting in increased rate of cardiovascular events and mortality [3]. It adversely affects the functional status of the limb and is associated with poor quality of life.
Aims and Objectives
- To compare the CD and DSA in diagnosing PVD.
- An attempt to define whether CD is an alternative or an adjunct to DSA
- Can CD replace DSA in diagnosing PV
- To evaluate the abnormalities of vascular disease with using color Doppler and digital
- Sustraction angiography
- To compare the findings color Doppler and digital substraction angiography.
- Association of risk factors
- Localisation of flow obstruction in peripheral vessel
- Idetification of type and length of stenosis/ occlusion
- Grading of stenosis
- Evaluation of post occlusive out flow tract
Material and Method
Study Design
Cross sectional Prospective study.
Period
September 2015 to Jan 2017.
Work Place
Department of Radiodiagnosis G.R. Medical College & Jayarogya Hospital, Gwalior using ALOKA SSD-4000 USG machine with high frequency linear probe & low frequency curvinear probe and Allenger DSA with C-Arm machine.
Study Group
All those patients which were referred for digital substraction angiography, in department of Radio diagnosis, G.R. Medical College Gwalior, Madhya Pradesh.
Sample Size
50 Patients
Inclusion Criteria
Patient with complaints pertaining to peripheral vascular disease, who was due for Digital Subtraction Angiography in Department of Radiodiagnosis, Jayarogya Hospital Group & Gajra-Raja Medical College Gwalior, Madhya-Pradesh.
Exclusion Criteria
a) Pregnant female. b) Children. c) Previously operated cases of peripheral vascular disease. d) Patients with renal and heart failure. e) Patients with previous history of allergic reaction to drugs.
Methodology
Patient with complaints pertaining to peripheral vascular disease, who was due for digital substraction angiography, was taken for Color Doppler examination.
Duplex Ultrasound Criteria for Arterial Evaluation
B – Mode: Assess ability
Anatomy (course, variants) Vessel contour (aneurysm, stenosis) Wall thickness (calcification, plaque) Pulsations (axial, longitudinal) Per vascular structures (haematoma, abscess, compressing structures)
Doppler
Demonstration of flow Flow direction Flow pattern (laminar, turbulent) Flow character (monophonic, biphasic, triphasic) Flow velocity
Technical Aspects of Arterial Duplex Imaging
The examination is explained and a history (risk factors, signs and symptoms) is obtained from the patient. The presence/absence of peripheral pulses and bruits should be documented. Arterial duplex imaging is performed with the patient lying in the supine position on an examination table. Peripheral arterial imaging begins at the level of the aortic bifurcation. Visualization of the proximal arteries is improved if patients do not take anything by mouth the morning of the examination. It is best to use a low frequency transducer (2.0-3.5 MHz) for the proximal segment of the examination. The aortic bifurcation is best seen with the patient turned to the left side and with the transducer placed just in front of the right iliac crest in a longitudinal plane. The distal aorta can usually visualize with the origin of both common iliac arteries. Doppler signals should be obtained from all three vessels at this location. Turn the patient into a lateral decubitus position (side being evaluated up) to evaluate the internal and external iliac arteries with the transducer placed between the iliac crest and the umbilicus. Doppler waveforms should obtain from the internal and external iliac arteries, noting direction of blood flow and velocity. If difficulty is encountered in locating the iliac arteries from this approach, the arteries may be located by identifying the femoral arteries at the groin level and following the arteries proximally. The patient returns to the supine position and a higher frequency linear array transducer (5-10MHz) should be used for evaluation of the arteries of the lower extremity. The common femoral artery is located at the level of the groin. The artery lies lateral to the common femoral vein. Imaging should be performed in the longitudinal plane, and a Doppler Signal should be obtained from this artery. The vessel should be followed distally on the leg to the origin of the superficial femoral and profundafemoris (deep femoral) arteries. Doppler signals should be obtained from the origin of both the superficial femoral artery and the Deep femoral artery. The superficial femoral artery is followed distally as it courses down the medial aspect of the thigh. Doppler signals should be obtained along its pathway and at areas of questionable narrowing. The distal portion of the superficial femoral artery may be easier to evaluate from the distal posterior thigh. This artery is followed distally in the limb and becomes the popliteal artery. The popliteal artery should be followed through the popliteal fossa. The popliteal artery lies deep to the vein, and Doppler spectral waveform should be obtained from this vessel. Following the distal popliteal artery in a longitudinal plane, the origin of the anterior tibial artery can usually be visualized diving deep on the monitor. The anterior tibial artery can only be followed for a short distance from this approach. The remainder of the vessel can be located distally by placing the transducer on the lateral calf and it can be followed to the level of the ankle. The tibial-peroneal trunk extends into the calf from the popliteal artery. The posterior tibial and peroneal arteries are usually visualized by placing the transducer on the medial calf. The peroneal artery lies deep and runs parallel to the posterior tibial artery. These vessels are located above the malleolus and followed proximally. At the end of the arterial duplex examination, the ultrasound gel should be removed from the patient with a clean towel, and any excess gel should be removed from the transducer. The transducer should be cleaned using a disinfectant.
Digital Substraction Angiography
Patient those planned was investigated done all routine work up including HIV & HBsAg. Then after taking informed and written consent, and after lignocaine sensitivity test, patient was taken on DSA examination table .Under all aseptic precautions and under monitoring of anesthesiologist femoral artery puncture was done with patient in supine position. After reaching up to concerned vessel through Trans- femoral route dye was injected through catheter into concerned vessel. Followed by fluoroscopic and digital substraction image was taken. Findings were noted and were compared with color Doppler finding. The collected data was analyzed with the aid of calculator and presented in the form of tables, graphs, figures and diagrams wherever necessary. The findings are discussed and compared with findings of other similar studies.
- Observation and Results
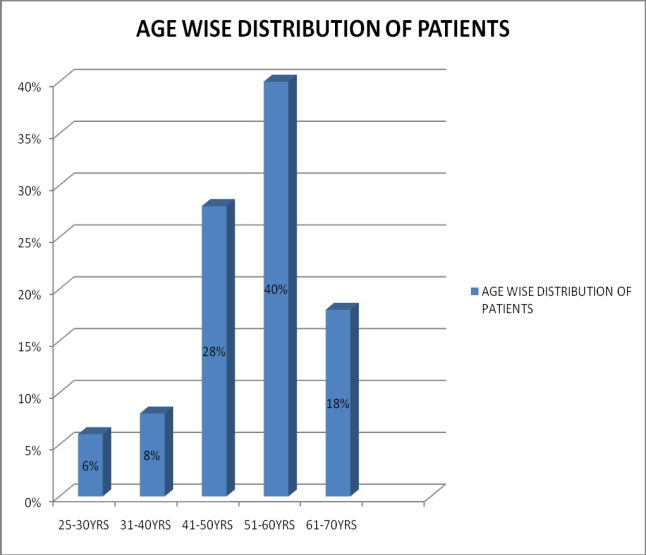
- Age (Years)
- Male
- Female
- No. of patients
- Percentage
- 25-30
- 3
- 0
- 3
- 6%
- 31-40
- 4
- 0
- 4
- 8%
- 41-50
- 12
- 2
- 14
- 28%
- 51-60
- 17
- 3
- 20
- 40%
- 61-70
- 8
- 1
- 9
- 18%
Table 1: Age Wise Distribution of Patients.
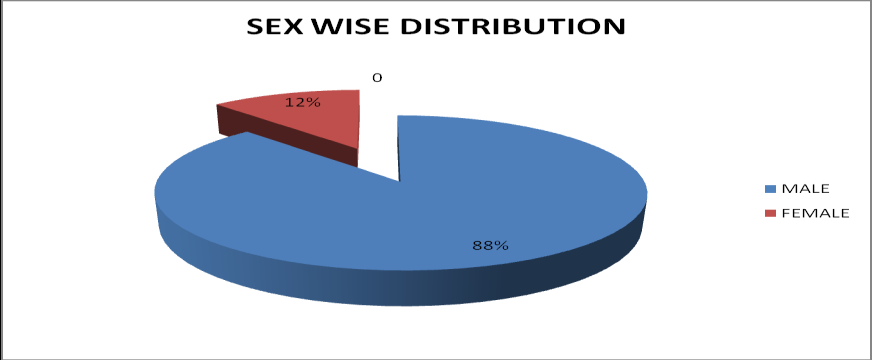
| Sex | No. of patients | Percentage | ||||||
|---|---|---|---|---|---|---|---|---|
| Male | 44 | 88% | ||||||
| Female | 6 | 12% | ||||||
| Total | 50 | 100% |
Table 3: Sex wise distribution of patients
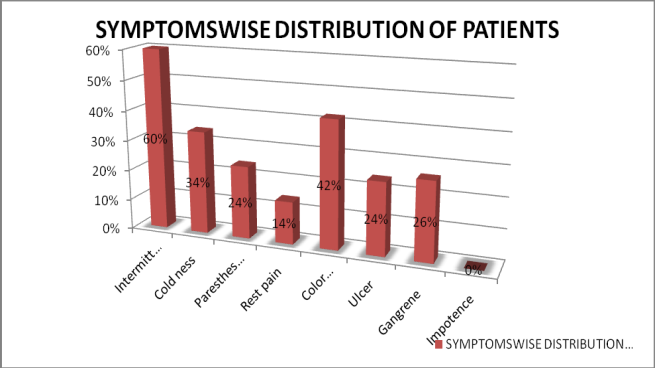
| Symptoms | No. Of patients | Percentage | ||||||
|---|---|---|---|---|---|---|---|---|
| Intermittent claudication | 30 | 60% | ||||||
| Cold ness | 17 | 34% | ||||||
| Paresthesias | 12 | 24% |
| Rest pain | 7 | 14% |
|---|---|---|
| Color changes | 21 | 42% |
| Ulcer | 12 | 24% |
| Gangrene | 13 | 26% |
| Impotence | 0 | 0 |
Table 2: Symptoms wise distribution of patients
| Risk factor | No. of Patient | s | Percentage | |||||
|---|---|---|---|---|---|---|---|---|
| Hypertension | 25 | 50% | ||||||
| Smoking | 40 | 80% | ||||||
| Alcohol | 13 | 26% | ||||||
| Diabetes mellitus | 23 | 46% | ||||||
| IHD | 5 | 10% | ||||||
| Hyperlipidemia | 25 | 50% |
Table 4: Risk factored wise distribution of patients
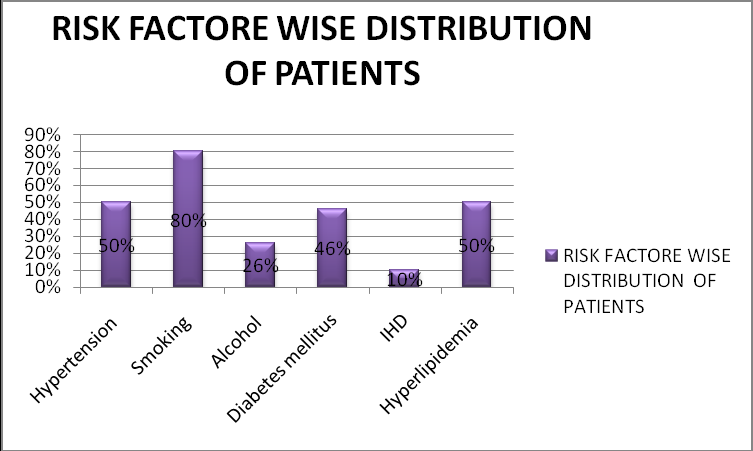
In the history taken during the study for risk factor evaluation, it showed that smoking, hyperlipidemia, hypertension and diabetes were the major risk factors.
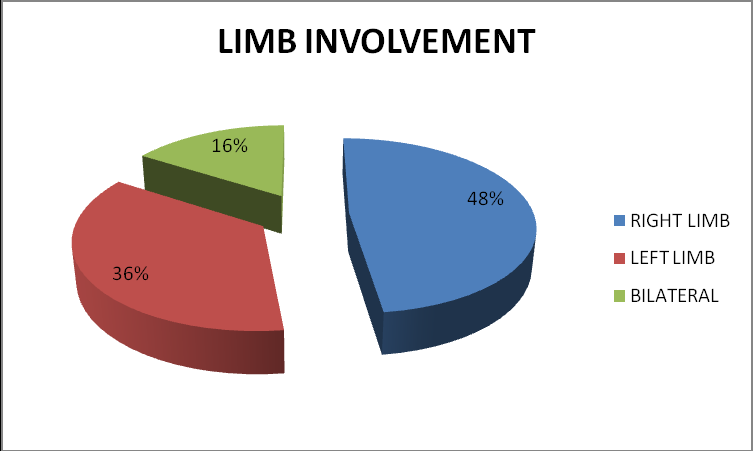
| Limb involvement | No. of Patients | Percentage | ||
|---|---|---|---|---|
| Right limb | 24 | 48% | ||
| Left limb | 18 | 36% | ||
| Bilateral | 8 | 16% | ||
| Total | 50 | 100% |
Table 7: Limb Involvement
| Level | Right limb | Left limb | ||
|---|---|---|---|---|
| CIA | 2 | 1 | ||
| EIA | 1 | 2 | ||
| CFA | 8 | 3 | ||
| SFA | 16 | 12 | ||
| DFA | 4 | 3 | ||
| POP. A | 11 | 9 | ||
| PTA | 6 | 7 | ||
| ATA | 5 | 6 | ||
| PERONEAL | 1 | 2 | ||
| DPA | 3 | 3 |
Table 9: Site of Lesion on Doppler in Lower Limb.
| Percentage of stenosis | No. of patients | ||||
|---|---|---|---|---|---|
| Percentage | |||||
| on CD | |||||
| 1-19% | 5 | 10% | |||
| 20-49% | 10 | 20% |
| 50-99% | 16 | 32% |
|---|---|---|
| Total occlusion | 19 | 38% |
| Total | 50 | 100% |
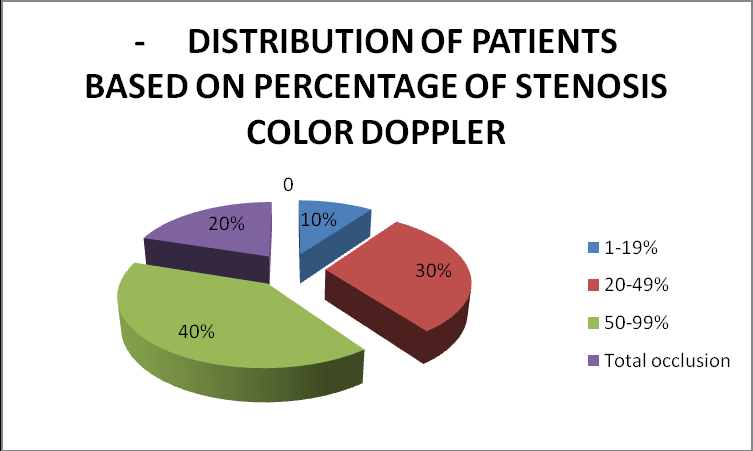
Table 6: Distribution of Patients Based On Percentage of Stenosis on Color Doppler.
On categorizing patients based on percentage stenosis, 10% of them showed 1-19% steno tic lesion, 20% of them showed 20-49% stenosis, 32% showed 50-99% stenosis and 38% of them showed total occlusion.
| Percentage of stenosi | s | N | o. of patient | s | Percentage | |||
| 1-19% | 5 | 10% | ||||||
| 20-49% | 15 | 30% | ||||||
| 50-99% | 20 | 40% | ||||||
| Total occlusion | 10 | 20% | ||||||
| Total | 50 | 100% |
Table 8: Distribution of Patients Based On Percentage of Stenosis on Dsa
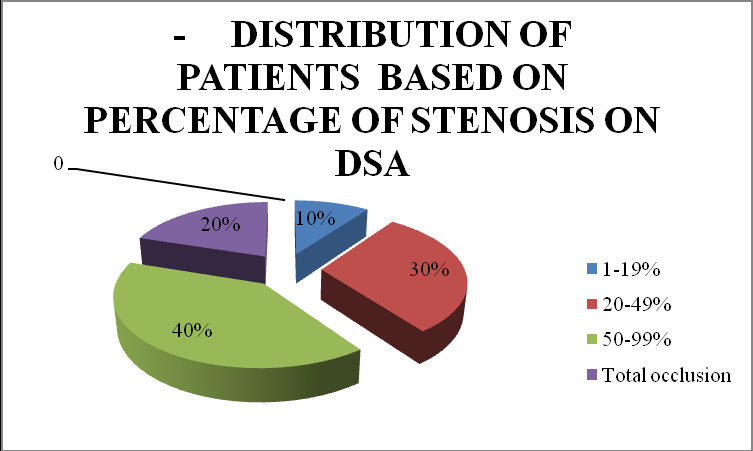
Among patient studied 60% of them showed significant (50% or more), and 40% showed non-significant (<50%) stenosis.
- PSV ratio
- No. of patients percentage
- <2:1
- 15
- 30%
- 2-4:1
- 12
- 24%
- >4
- 4
- 8%
- Total Occlusion
- 19
- 38%
- Total
- 50
- 100%
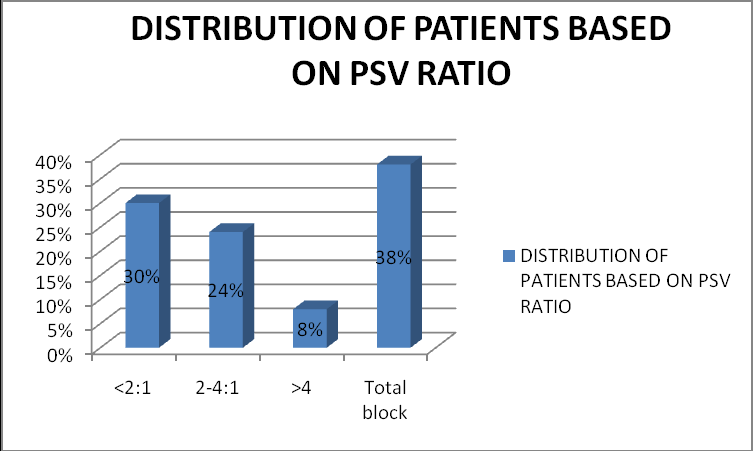
Table 11: Distribution of patients based on PSV ratio
| DSA | S | ignifican | t | Not significan | t | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| T | ota | l | |||||||||
| Color Doppler | (<50%) | (<50%) | |||||||||
| Significant (>50%) | 42 | 6 | 48 | ||||||||
| Not significant (<50%) | 4 | 248 | 252 | ||||||||
| Total | 46 | 254 | 300 |
| DSA | S | ignifican | t | Not significan | t | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | |||||||||||
| COLOR DOPPLER | (>50%) | (<50%) | |||||||||
| Significant (>50%) | 20 | 10 | 30 | ||||||||
| Not significant (<50%) | 4 | 116 | 120 | ||||||||
| Total | 24 | 126 | 150 |
Discussion
Peripheral arterial diseases form one of the most important causes of morbidity and death worldwide [4]. P.A.D. can affect your quality of life, make walking difficult, or worse, increase your risk of heart attack, stroke, leg amputation and even death [5]. Early diagnosis and treatment of P.A.D. can help to: – Prevent disability and restore your mobility – Stop the disease from progressing – Lower your risk for heart attack, heart disease, and stroke. For long angiography has been considered the Gold standard in evaluation of PVD and is done before any surgery is planned. This investigation is done to demonstrate the extent of the lesion, condition of vessels above the lesion, development of collaterals and reformation of distal vessels [6]. It provided excellent anatomical detail. However, it does not give adequate physiological information about the hemodynamic of lower limb [7]. It is associated with risks due to its invasiveness, cost, contrast associated complications and it does not give information about plaque. With the recent introduction of CTA, MRA, the study has become further improvised but because of their high cost and unavailability, colour Doppler Duplex sonography becomes the most easily available modality for evaluation of arteries. Over the past several years, interest in noninvasive testing of PVD has increased rapidly. The use of the Duplex sonography has revolutionized the investigation of blood vessels. Colour Doppler is the most valuable of the noninvasive tests [8]. Colour Doppler imaging is safe, popular, cost effective, repeatable, noninvasive procedure for investigating lower limb arteries. It can provide most of the essential anatomic information and functional information like velocity gradients across the stenosis, degree and extent of occlusive lesion. Doppler studies are helpful in postoperative follow-up of operated limbs where arterial surgery has been carried out. In this study the peripheral vascular disease was evaluated clinically and by Duplex imaging [9].
Age Distribution
In our study 86% of the cases were above the age of 40 years and 14% of the cases were between the ages of 25- 40 years. It is well accepted fact that the lower extremity arterial disease is the disease of middle and older age groups as cited by Cossman, et al. 23, Hughson et al.
Sex Distribution
Among 50 diagnosed cases of peripheral vascular insufficiency, patients who underwent Doppler study 44(88%) were males and 6 (12%) were females. Hughson et al observed that 2% of males and 1% of females had symptoms of peripheral vascular disease.
Signs and Symptoms
Intermittent claudicating, rest pain and, color changes are very important signs of lower limb Ischemia. We found 60% of patients in this study having intermittent claudicating. Tetsuo Ostida, et al. 56 found 69 out of 144 ischemic limbs of TAO having this symptom. JL Juergen found it in 100% of atherosclerotic patients. M. Hamilton in 1952 found claudicating was directly proportional to the degree of thrombosis and rest may have little effect on pain. Lindbom A57 found that narrowing of the arterial lumen less than 20% and thrombosis are the two main causes of claudicating rest pain indicates advanced arterial insufficiency to maintain normal requirement of the limb even at rest. Rest pain was found in 14% of our patients. B. Ranjan58 reported 105 rest pain and 62 gangrene/ulceration of total 188 cases. In our study 26% cases had gangrene and 24% cases had ulcers. B. Ranjan noted that the maximum gangrene was associated with distal blocks and popliteal blocks. The incidence of gangrene being 50% in each case, while with femoro- popliteal it was 20%. Out study shows that the maximum block at the level of femoro- popliteal trunk followed by distal run-off arteries. Other symptoms are colour changes (42%), coldness (34%) and Paresthesias (24%). In our study we found clinical evaluation of peripheral pulses as a very important adjunct to colour Doppler study. It helps to suspect the possible site of block and we found good correlation between clinical levels of block and colour Doppler findings in majority of cases.
Risk Factors
In our study 80 % of the patients were smokers with average smoking of 25- 30 cigarettes/bedis per day for a period ranging from 10-30 years. Tobacco smoking affects both arteriosclerosis oblitererans and thromboangitisobliterans (TAO) but TAO is exclusively seen in young smokers. The relationship between smokers and PVD is known since 1911 when Erb59 reported intermittent claudication was 3 times more common among the smokers. 26% of patients in our study had history of alcohol intake for average of 10 years. William F. Ganong noted intake of alcohol promotes increase in blood lipid levels, which promotes atherosclerosis. In our study 50% of patients with hyperlipidemia 50% of patients had hypertension, 46% were diabetes and 10% had IHD.
PSV Ratio
Among patients who had plaque 12 (24%) had PSV ratio of 2-4, 4(8%) had PSV ratio >4, 15(30%) had <2 and 19 (38%) patients had total block. PSV at stenosis and ratio of PSV at stenosis is compared with velocity 1-2cm upstream in a non diseased segment. According to Cossman et al PSV ratio of >2 are indicative of hemodynamically significant stenosis i.e. >50%-75% stenosis and >4 have >75%- 99% of stenosis. Cossman et al have produced accurate results by using PSV ratio for quantifying degree of stenosis. In our study PSV ratio was used which is easy to remember and it can also sub classify 75-99 % of stenosis?
Spectral Waveform Changes
In our study spectral waveform changes were observed and the 2 main features, which are altered are, the overall shape of the waveform and the degree of spectral broadening as a result of flow disturbance. The spectral waveform was monophonic i.e. loss of third and then second phase of the normal triphasic waveform at the areas of hemodynamically significant stenosis and distal to it. The width of the first, systolic complex is increased and overall height is decreased. These changes result in dampening of the waveform which is most marked when there is proximal occlusion. The turbulence generated beyond the stenosis resulted in spectral broadening and spectral fill-in under normal window under the first phase systolic peak. No flow was recorded in cases of occlusion. In cases with distal disease the changes which were seen are the reduced diastolic component, evident from the loss of third component and reduced peak systolic velocity. These findings are comparable to findings of other studies Jager KA et al. 32. Other findings included diffuse irregularity of the vessel wall and resultant irregularcolour fill-in in most of the patients suggesting increased Intima-medial thickness.
Color Doppler versus DSA
Thakur RS, Minhas SS, Dhiman DS, Abbey RK ( Department of General Surgery, IGMC Shimla, HP, *Department of Radiology, RPGMC Tanda, HP, India) showed good statistical agreement between the findings of CFD and arteriography in both the aortoiliac as well as femoro-popliteal region, for identifying hemodynamically significant lesions, with the kappa ranging from. 773 to 1, which represents excellent to perfect agreement [15].
Sensitivity ranged from 80% to 100%, specificity 93% to 100%, PPV from 77% to 100%, NPV from 90% to 100% and accuracy from 91% to 100%, in different vascular segments. Eiberg JP, et al. in their found agreement between color Doppler and DSA was significantly better in supragenicular (sensitivity-88% (85-91%), specificity, 88% (84%-91%), PPV-93% (90%-95%), NPV-81% (77%- 81%), than for infragenicular sensitivity- 88% (85%- 90%), specificity- 75% (71%-78%), PPV-83% (81%- 86%). NPV- 81% (77%-84%). He also found that even in most experienced centre, 5-20% of patients are impossible to insunate sufficiently on color Doppler due to ulcer, oedema, pain, heavy calcification, and obesity. Aly S, Sommerville K, Adiseshiah M, Raphael M, Coleridge Smith PD, Bishop CCR found that compared with angiography, duplex imaging was able to detect arterial disease with an overall sensitivity of 92 per cent, specificity of 99 per cent, positive predictive value 91 per cent and negative predictive value 100 per cent, and with a P value of 0•87 (95 per cent confidence interval (c.i.) 0•81–0•93). Duplex was able to determine the length of the arterial lesion with a sensitivity of 89 per cent and a specificity of 98 per cent with a κ value of 0•88 (95 per cent c.i. 0•86–0•90). When the surgeon's final management decision concerning each vascular lesion was used as the reference, duplex and arteriography were equivalent, with an accuracy of 84 per cent and 85 per cent respectively in identifying the management used and concluded. Duplex ultra sonography is reliable in detecting arterial lesions in peripheral arteries and could be used routinely in the initial evaluation of patients with lower limb arterial disease. In our study we also found for supragenicular Sensitivity= 91.3%, Specificity = 97%, PPV = 87% , NPV = 98% and for infragenicular ,Sensitivity = 83% , Specificity = 92%, PPV = 66% , NPV = 96%, which are comparable to previous studies. Our results are in good agreement with the earlier studies.
Koelemay et al,
in their review article, concluded that CFD is an excellent tool in the noninvasive work up of patients with PAOD, in aorto-iliac and femoro-popliteal segment. Because of its high diagnostic accuracy, it can replace routine diagnostic arteriography for planning surgical intervention or PTA in a substantial number of patients. For assessment of infra-crural arteries, angiography remains a pre-requisite and our results seem to substantiate this. CFD is able to identify distal runoff well and can also comment decision of whether or not to proceed for angiography, can be taken on the basis of results of CFD and treatment plans can be formulated prior to arteriography, as CFD provides sufficient information as whether to proceed to endovascular intervention or surgery. The road map of the arterial tree inferred from pre- angiographic CFD can be helpful to the angiographer to tailor the angiographic technique for the patient. Moreover, the angiographic approach can be determined beforehand, as the road map of the arterial tree inferred from the pre- angiographic CFD is already at hand. The accuracy and time spent obtaining the arteriograms are also improved, by obviating the need to look for lesions where they do not exist. In addition, examination time is decreased and contrast load diminished if portions of the arterial system can be shown normal on CFD. CFD is also a more accurate way to access the exact length of an occlusion than arteriography, the latter tending to overestimate the length of the lesion. Cautious approach is required in undertaking operative or catheter based procedures in the treatment of PAOD, on the basis of triplex scan results alone, till more experience is gained. However, in the event of triplex scan revealing steno tic lesion, angioplasty can be planned at the time of routine arteriography, combining diagnostic and therapeutic intervention in the same sitting. In patients needing femoro-distal reconstruction, diagnostic arteriography is still recommended in planning operative treatment.
False Positive Occlusions
These are reported to occur due to sluggish low velocity flow, with most of the blood being diverted away from the main vessel by the collaterals, decreasing the amount of blood carried by it, which is not picked up by doppler with the overlying gases in the bowel, movement of abdominal wall due to respiration and heavily calcified vessel wall, leading to beam attenuation, further compounding the problem. It is also reported to be due to diffuse insignificant proximal disease. Moreover, distal third of the superficial femoral artery has been called a blind spot for sonographers.
False Negative Occlusions
This phenomenon of non visualization of patent segments on Doppler is known and reported in literature and has been demonstrated in other studies. This non- opacification of normal segment distal to occlusion is said to be due to its filling with non opacified blood from the collaterals, not carrying the contrast due to timing, or flow or pressure variables. The results are misleading, leading to overestimation of occlusion lengths and at times, revealing no runoff on arteriography and subsequent selective arteriography, or observations at surgery tend to substantiate the findings of the CFD. Vascular surgeons have known this for a long time and will explore non- visualized distal vessels for distal bypass grafting, if Doppler is detectable. This shows that our observed sensitivity can be deceptively lower. Moreover arterial collateral branch can also be inardventely sampled as the patent main arterial segment, as reported literature [10, 11, 12].
False Positive Stenosis
This possibly occurred due to sampling error, as narrowing was not appreciated on the colour scan and spectral waveform in the distal vasculature was tri- phasic, whereas abnormal spectral waveform should continue in the distal vessels [13].
More experience in the future will avoid such errors. Thus, CFD can facilitate the pre-angiographic determination of the nature and extent of arterial disease in the lower limbs. Normal CFD virtually excludes significant lesion, which in turn helps reducing the number of unnecessary diagnostic arteriography in patients with symptoms not justifying the surgical or endovascular procedure. standard of arteriography and provides high-resolution, precise anatomical and physiological information of the peripheral arteries. It is a safe, fast, inexpensive and repeatable non-invasive procedure for investigating PAOD, which can be performed on outdoor basis without hospital admission. With arteriography as the ‘gold standard’, deceptively poor results can be produced, due to non-visualization of segments patent on CFD. A high NPV shows that significant lesions in the vascular tracts can be reliably excluded, which can help reduce the number of diagnostic angiographies, in patients with symptoms not justifying a surgical or endovascular procedure. The study found that, when scan demonstrates normal artery, the angiogram also shows normal segment. Thus, CFD has grown from an ancillary diagnostic aid, to a critical component in the diagnostic workup, raising the possibility of displacing arteriography as the primary diagnostic imaging modality, for patients with chronic arterial occlusive disease of the lower extremity.
Limitation of Study
First, there is a clear selection of patients with higher degrees of stenosis, as all patients were scheduled for interventional procedures. It remains to be investigated whether these findings are reproducible in unselected patients with peripheral artery disease. Second, angiography was done in the AP view only and thus may have a limited accuracy as well. This partly may account for discrepancies with DUS, and DUS in fact may have been even more accurate in eccentric lesions than monoplane angiography Larger sample could have given better outcome and stenotic and occlusions could have been studied separate.
Conclusion
Elderly people are with increased risk of peripheral arterial disease. Males are more commonly affected with smoking as the commonest risk factor. The other common risk factors include diabetes and hyperlipidemia. The commonest site of pathology is femoro-popliteal segment.
Duplex color Doppler sonography
- Can accurately locate the site and extent of stenosis/occlusion.
- Can be used to classify peripheral arterial disease intohemodynamically non-significant and significant using Peak systolic velocity, Peak systolic velocity ratios and spectral waveforms which will help in management.
- Is safe, cost effective, repeatable, noninvasive procedure for investigating lower limb arteries. Hence it is the primary investigation of choice in all cases of lower extremity arterial disease and helps to decide the need for further evaluation by angiography.
- Allows the evaluation and quantification of arterial disease.
- Also helps in the follow-up of the arterial diseases.
- The agreement between DUS and DSA was generally good, irrespective of the severity of ischaemia. DUS performed better in the supragenicular arteries than in the infrageniculararteries. However, DUS compared favorably with DSA in both tibial vessels, particularly in the distal part, which makes DUS a useful non- invasive alternative to DSA.
- DSA shows better soft tissue vessel contrast.
- DSA assess better degree of stenosis and occlusion
- DSA gives better information about the collateral.
- DSA provides better anatomical details of vessel and hence detailed vascular tree mapping. Based on the above findings we draw the inference that Color Doppler is an initial investigation of choice in evaluation of peripheral vascular diseases specially in infragenicular portion of the vasculature, and is an adjunct to DSA, but cannot replace it.
References
-
Joseph F Polak Diagnostic Ultrasound. Carol MR, et al. 3rd (Edn.), 1: 993.
-
Paul L Allan, Karen Gallagher (2006) Clinical Doppler Ultrasound. 2nd (Edn.), pp: 73-99.
-
Krishnaswamy B, Raja N, Deepak S (2006) A Study of Peripheral Vascular Disease in Elderly and its Association with Coronary Artery Disease. Journal of the Indian Academy of Geriatrics 2: 10-13.
-
Abhay I Ahluwalia , Bedi VS, Indrajit IK, Souza JD (2003) Evaluation And Management Of Peripheral Arterial Disease In Type 2 Diabetes Mellitus Int. J Diab Dev Countries, 23.
-
Michael John Lunt (2000), Clinical Scientist, Clinical Measurement Department, Royal Bournemouth Hospital, Castle Lane East, Bournemouth, BH7 7DW, U Published in World Wide Wounds: September 2000 Version: 1.0.
-
(2004) Cipla Doc HOPE sub study, European Heart Journal 25: 17-24.
-
David Sutton, Roger HS Gregson (2002) Text book of Radiology and imaging 7th (Edn.), David Sutton, published by Churchill Livingstone volume 1.
-
(2001) Annales de Cardiologieetd Angeiologie duplex ultra sonography and lower limb arterial disease. 50(2): 112-118.
-
Raymond K Hung, Peter Zimmerman, Andre Duerinckx, Michelle Melany (1998) Edward Grant non invasive evaluation of peripheral arterial disease.
-
Hussain ST (1997) Blood flow measurements in lower limb arteries using duplex ultrasound. Ann R Coll Surg Engl 79(5): 323-330.
-
Criqui MH, Langer RD, Fronek A, Feigelson HS, Klauber, et al. (1992) Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med 326(6): 381-386.
-
Koshy CG, Chacko BR, Keshava SN (2009) Diagnostic accuracy of color Doppler imaging in the evaluation of peripheral arterial disease as compared to digital subtraction angiography. Vascular Disease Management 6: 2-9.
-
Vucaj-Cirilovic V, Nikolic O, Petrovic K, Govorcin M, Hadnadev D, et al. (2006) Basic characteristics of duplex sonography in the assessment of lower limb arterial circulation. 59(5-6): 287-290.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review