Septoplasty without Packing, Splints or Clip-Our Experience
Introduction: Septoplasty is a very commonly done surgery for deviated nasal septum in any Otorhinolaryngological department. Sometimes it may be combined with other procedures like FESS, synechiae release, AC polypectomy, Adenoidectomy, or turbinoplasty also. As the last step, nasal cavity is often packed with medicated gauze or splinted or rarely clips are also used for stabilization and to promote adhesion between the mucosal flaps of the septum. Most often a nasal pack is the choice for the surgeon as it is a simple procedure compared to splints and clips which are costly and have to be kept in the nose for variable time. This causes problems like, a blocked nose till the pack is removed, dry mouth, watering of eyes, and severe pain during removal of the pack blocked ears, headache, difficulty in swallowing, hypoxia, etc. We have conducted a prospective study 0f 58 patients undergoing Septoplasty for nasal blockage and these patients did not undergo any packing, or splints or clips Study Design: longitudinal observational Methods: 58 patients, who came to our department with a complaint of nasal obstruction during the period of one year from October 2015 to October, 2016. There were 46 male and 12 female patients. Youngest patient was 10 year old and the oldest was 55 years. We sutured the septal mucosa with 4 zero vicryl with a few quilting sutures and then continuous sutures for the approximation of the flaps and to prevent hematoma of the septum .On the day of operation and later also they were followed up for any bleeding or ,hematoma .All these patients were initially assessed with NOSE score to assess the degree of blockage, and then followed up, on the next day after a suction clearance with the same criterion to assess the comfort level, and after 1 week and finally after 1 month . During the follow up the nasal cavities were looked for any synechiae, hematoma or perforation of the septum or residual deviation. Results: In one patient, minor bleeding occurred within a few hours in the recovery room and the nose was packed. In another patient, since there was no perfect hemostasis, packing was done on the table itself. For two patients, since there was a little bleeding, I .V Tranexamic acid 500 mg was given and no packing was done. No complication occurred for the rest of the patients. No patient had any long term complication.Conclusion: Septoplasty by putting multiple continuous trans septal sutures after an initial one or two quilting sutures for stabilizing the corrected septum with absorbable 4 zero polyglactin suturing material, without packs, clips or splints inside the nose is a very effective method of preventing hematoma, or synechiae inside the nose at the same time, avoiding all the problems with a foreign material inside the nose even though temporarily with an obstructed airway. Thus, Septoplasty can be a day care procedure. The only problem is the extra time required for putting the suture which is negligible when considering the advantages.
Introduction
Man is the only animal with a deviated septum [1]. Septoplasty is a frequently done operation for symptomatic deviation of nasal septum, in many of the ENT departments either alone or in combination with other surgeries inside the nose. Erkan Eski, et al. [2] describes it as the 3rd frequent Otolaryngologic surgery. It is also being practiced as a part of Septorhinoplasty by the plastic surgeons. After completion of the surgery nose will be kept shut by a pressure packing inside the nose for variable period of time according to preference of individual surgeon at least for a period of 24 hours. The closed nose is causing multiple problems for the patients and also for the Anesthesiologists, and will be discussed later. While going through the text books it is seen that suturing of the nasal septum is a method by which we can avoid packing, splinting or using clips. Textbook of Scott Brown [3] says “There are different ways to keep the septal skeleton in place during healing. First of all, a dressing is put into the nose to bring the mucosa together. In this way, the septum is squeezed between the blades holding the skeleton in place. Mattress sutures have the same effect. Splinting by so-called nasal splints is effective in stabilizing reconstructions that are more extensive. They have the advantage that they can stay in the nose and allow the patient to breathe through the nose, thus prolonging the time the septum is supported. It should be noted that nasal packs are very uncomfortable for the patient.” Another author Beryline J Ferguson [4] says that “Other surgeons prefer using mattress sutures passed through the mucoperichondrial flaps, and others rely on nasal packing. If packing is used, the gauze should be impregnated with antibiotics. Antibiotics should be Inclusion criterion– All the patients presenting with symptomatic deviation of nasal septum presenting to the senior author who required septoplasty for the cure of their symptoms and among them eight patients required additional procedures like polypectomy, synechiae release, adenoidectomy or turbinoplasty (Table 1). All the patients were of ASA 1 or 2 risks only. (American Society of Anesthesiologists) Exclusion criteria were hypertension, diabetes, cases were bleeding is anticipated like patients on anti platelet drugs or those who are having coagulation disorders. Revision surgery was not a contraindication. We studied 58 patients who came to our department with complaints of nasal obstruction for a period of one year from October 2015 to October 2016.All the patients underwent proper septoplasty by the same surgeon. In three cases, septoplasty was combined with polypectomy. Synechiae release, and endoscopic powered turbinoplasty of inferior turbinate was done in two cases and adenoidectomy was combined in one patient. Nose was not packed in any of the cases.
administered systemically intraoperatively and postoperatively.” In yet another text book Jeevan B Ramakrishnan says “mucosal incision is then closed with absorbable suture. At this point, the septum can be quilted with absorbable suture / or splints can be placed " [5] It is written in the text book by Nabil Elsahy Basic Septoplasty and Turbinate Reduction;; Plastic and Reconstructive surgery of the Nose [6] “hemostasis is achieved by quilting sutures and light Telfa packing with antibiotics is inserted’’ Pack less septoplasty by sepal suturing can avoid these problems at the same time can serve all the functions a pack does in septal surgeries. Hence Septal surgeries will no more be a nightmare with pack less septoplasty.
Materials and Methods
adenoidectomy 40 male 2male 2male 1male 1male 10 female 1 female 1 female

| No pack | Tranexamic acid | No pack, with C-PAP | Mild bleeding,pack removed after 30 mts | Bleeding in the recovery room -pack kept for 6 hours |
| 55 | 2 | 1 | 1 | 1 |
Table 1: Problems encountered and the way by which they are tackled.
| Patients aged between10-16 | Between16-43 | Between43-55 | male | Female |
| 7 | 45 | 6 | 46 | 12 |
| one operated cleft palate | 45 | 6 | 46 | 12 |
Table 2: Age and sex distribution.
| Problem | 0 | 1 | 2 | 3 | 4 | Final score |
|---|---|---|---|---|---|---|
| Not a problem-0 | Very mild problem-1 | Moderate problem-2 | Fairly bad problem-3 | Severe problem-4 | ||
| Nasal congestion or stuffiness | ||||||
| Nasal blockage or obstruction | ||||||
| Trouble breathing through my nose | ||||||
| Trouble sleeping | ||||||
| Unable to get enough air through | ||||||
| my nose during exercise or exertion |
Table 3: NOSE scale, the criterion of assessment of preoperative and postoperative conditions as described by Stewart.
Procedure
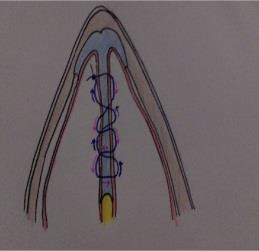
Septoplasty is performed using standard technique under G. A. An initial infiltration with 2 percentxylocaine containing 1/1000 adrenaline was given 5 to 10 minutes before the surgery and the nose was packed with surface anesthetic agent 4 percent xylocaine diluted with adrenalin. The Anesthesiologist keeps the mean arterial pressure around 65 m .m of mercury. Then the usual septoplasty procedure is carried out and care is taken to avoid any septal tear. Finally the incision made in the anterior end of septum is sutured with absorbable sutures of 4 zero Vicryl. Initially a quilting suture is put on the septum starting from the roomy side going to the narrow side and then coming back to the wider side so that it can pull the deviated septum to the midline. Then continuous sutures are placed on the septum to hold the flaps together and to prevent hematoma formation. A 4 0 vicryl on a curved cutting needle is used. A knot is made at the end of the suture. Starting from the anterior end till posterior end the needle is passed through the septum from one nasal cavity to other. Thus, sutures are put, back and forth from one side of the nose to the other, in a zig- zag manner, ensuring that all the areas of separated mucous membranes are closed together. Postoperatively, head end of the patient is kept elevated, and saline nasal irrigation, topical nasal decongestant nasal drops are put, antibiotics, antihistamines and analgesics are given. If found necessary, a5 to 10 minutes packing can be given before the patient comes out of the Anesthesia and then the pack is pulled out. A smooth recovery from the Anesthesia is very much essential otherwise bleeding can occur. If mild oozing is noticed at this time, Inj. Tranexamic acid can be given and usually the bleeding stopped.
The patient is then monitored for any bleeding in post- operative room for one hour and if there is no problem, can shifted to post-operative ward. Then close monitoring is necessary to check for any bleeding, hematoma formation and then can be discharged the next day after a suction clearance with an advice not to strain and keep the head end elevated for a few days more. In two patients, for whom endoscopic powered inferior turbinoplasty was done , Surgicel which is absorbable oxidized regenerated cellulose (manufactured by Ethicon, LLC, SanLorenzo, Puertorico, USA) was kept along the entire raw area and the nasal cavity kept open. These patients were then followed up for a period of 3 months to see if he/she develops any problems related to this technique. Post operatively they were evaluated at 1 week, 1 month and 3 months respectively with NOSE scale and the improvement is recorded. The average time taken for doing Septoplasty was 20 minutes and the mean time for suturing was 23 minutes even though in the initial series it was more than the mean The mean arterial pressure of the patient was around 60-65m.m.
Results
All the patients were followed up in the above mentioned manner. It was seen that the symptoms improved very much after a suction clearance on the first post-operative day and the Nose Score improved. Better results were obtained after one week. There were no symptoms after one month. There were no incidents of synechiae, hematoma or perforation in any of these patients. Most of them were discharged on the next day itself after suction clearance. Post operatively, NOSE scores came down on the first post-operative day itself and continued to improve when the score was calculated after one week, one month and finally after three months. There was no hematoma, synechiae, perforation or residual deviation.
Discussion
Septoplasty is a surgical procedure to correct a deviated nasal septum. Common indications of septoplasty are 1) nasal airway obstruction 2) septal spur headache 3) nasal septal deformity in the presence of other intranasal surgery 4) for harvest of septal cartilage for reconstructive purposes(nasal reconstruction) 5) as part of pituitary surgeries6. A sharp spur causing bleeding Six phases 3 in standard septoplasties are (1) gaining access to the septum; (2) correction of pathology (3) removing pathology (4) shaping removed cartilage and bone (5) reconstruction of the septum (6) stabilizing the septum. Last phase of stabilizing the septum following septal surgeries was conventionally achieved by nasal packs (anterior nasal packing). Medicated packs like Ribbon gauze, fingerstall packs, polyvinyl acetate sponge (Merocel), cellulose sponges, and carboxymethyl- cellulose, balloon tamponade has been described by Rowan V, et al. [8]. Other methods of stabilizing the septum include, Splints [9] Clips [10], various materials including cotton tape, gauze, paraffin gauze, Tefla, Merocel, sponges, and silicone nasal splints have been recommended for this purpose [11]. I septoplasties, the mucoperichondrial and mucoperiosteal flap layer on both sides of the midline cartilaginous septum is elevated, and the deviated portion of the cartilage or bone is removed. Then, the flaps are placed back together in the midline. Packs are placed on either side of the septum, to splint the septum in new position, compress the mucous membrane layers together, thus promoting adhesion between the same thereby preventing blood clots in between them. Cartilage gets its blood supply and nutrition from its perichondrium so left over cartilage has to be in contact with the perichondrium for its survival. A septal hematoma or abscess that separates the two mucous membrane layers can hamper nutrient flow to the remaining cartilage thus the cartilage die off, leading to drooping of nasal tip. The first study in rabbit noses was published in 2004 by Erkhan G, et al. [12] and the septal suture is an efficient and useful method for bringing the septal flap over the septal cartilage. Disadvantages commonly encountered during anterior nasal packing are compromised nasal breathing, dryness of mouth, nasal pain, nasal valve narrowing, occasional ear block sensation, vestibulitis, crusting, synechiae, headache, watering from eyes, irritation of throat, difficulty in swallowing, hypoxia, hypoxemia-in patients with Obstructive sleep apnoea syndrome. Toxic shock syndrome is a rare complication [8]. Tight packing may even lead to septal perforation, adversely affects mucosal ciliary activity and can jeopardize the vascularity causing septal perforation. Awan MS, et al. [13] noted that nasal pack removal is very painful [13]. In our study, we have done trans-septal suturing. Which avoids all these disadvantages? Moreover it is comfortable for the patient and reduces hospital stay. Study conducted by Cukurova, et al. [14] in 697patientsfound that the routine use of nasal packing is not justified, and also showed a positive impact on patient comfort after surgery for septoplasty using the suturing technique. Suturing technique also had less pain and complications. Study conducted by Daniel Pérez P, et al. [15] named Transeptal suturing – a cost- efficient alternative for nasal packing in septal surgery. They say that Transeptal suture is an effective and safe alternative to classic nasal packing in septal surgery. Moreover, it improves the efficiency of the intervention by saving costs. Sashikanth JA, et al. [16] says that avoidance of nasal packing or splints does not increase the incidence of postoperative bleeding complications while the associated morbidity and pain can be avoided. Sarfaz MB [17] in a meta-analysis named “Is nasal packing nessary after septoplasty” says that most of the RCTs did not favor the use of nasal packing and did not show any significant benefit In a study named “Comparison of totally occlusive nasal pack, internal nasal splint, and trans septal suture technique after septoplasty in terms of immediate respiratory distress (RD) related to anesthesia and surgical complications” Melih C, et al. [18] concludes that patients who underwent septoplasty with bilateral totally occlusive nasal packing experienced higher immediate RD events than patients in whom trans septal suture technique and internal nasal splint were applied. Ina study named “The Effects on Cardiac Functions and Arterial Blood Gases of Totally Occluding Nasal Packs and Nasal Packs with Airway”, Ehab Z, et al. [19] says that the cardiac results were caused not by the obstruction of the nasal passage, but instead, by the pressure exerted on the nasal mucosa increasing the vagal stimulus by the pack, which may lead to cardiac problems. A close monitoring of patients with nasal packs is mandatory In a study of “Assessment of Complications of Nasal Packing after Septoplasty“ by Ali Maeed S Al-Shehri, et al. [20] concludes that Nasal packing in septoplasty patients is not necessary. It causes significantly more pain and complications, and it should be reserved only for those who have bleeding tendency. In another study by Christos G, et al. [21] says that-Patient satisfaction with day-case septoplasty has been shown to be high. It is possible only with a pack less Septoplasty In another study named ROUTINE NASAL PACKING FOLLWOING NASAL SURGERY— IS IT NECESSARY? “by SI Basha, et al. [22] says that the routine use of nasal packs after nasal surgery is not justified. Packing should be reserved for the patients with significant oozing after surgery in a study by Muhammad H [23], named SEPTOPLASTY WITHOUT NASAL PACKING concludes by saying The frequency of bleeding after septoplasty without nasal packing is low and nasal packing should be reserved only for selected cases Maria TB, et al. [24] in a study titled “Septoplasty with or without postoperative nasal packing? Prospective study” Says that Routine use of anterior nasal packing should be challenged for not presenting proven benefit Rajashri SM, et al. [25]in a study titled “Comparison of Septoplasty With and Without Nasal Packing and Review of Literature” says The use of nasal packing following septoplasty is thought to stabilize the remaining septum and prevent complications such as bleeding, septal hematoma, and formation of synechiae. Quilting sutures can effectively serve all the above purpose plus reduces the hospital stay Simple DNS can be safely treated with septoplasty Nasal packing should be should be reserved only for selected cases. Kiran Naik [26] in his article, “A Novel Way of Trans-Septal Splint Suturing Without Nasal Packing for Septoplasty”. Says that This study also confirmed that intranasal packing would result in increased incidence of adhesions and synechiae than the trans-septal through and through splint suturing technique. Moreover, the septal surgery procedure could be based on these observations the septal suturing technique is a valid alternative to intranasal packing following septal surgery Korkut Arzu Y [27] in his article named, “A randomized prospective trial of trans-septal suturing using a novel device versus nasal packing for septoplasty” says, -suturing that is easy to use in the nasal cavity. We conclude that the use of continuous septal suturing with our device is an easy modification of the standard procedure, with only a small increase in operating time Naghibzadeh B [28] in his article, “Does Post Septoplasty Nasal Packing Reduce Complications? Says Septal suture is one of the procedures that can be used as alternative method to nasal packing. Therefore the nasal packing after septoplasty should be reserved for the patients with increased risk of bleeding Erkan Eşki, et al. [29] in their article, Effects of nasal pack use on surgical success in septoplasty renasal pack use does not affect surgical success and complication rates in septoplasty. Pack-free septoplasty with the trans-septal suture technique is an effective method in the treatment of septal deviation. Caner Şahin, et al. [30] in their paper. “Influence of nasal pack removal on patients’ anxiety after septoplastyconcludes by saying that they recommend administering soluble packs or sewing techniques without nasal packs after septoplasty due to concerns related to quality of life after surgery. If packing can be avoid in the nose, it will be highly beneficial for all those who are caring the patient and all the more for the patient because he/she can breathe easily through an open nose and septoplasty can be done as a day care procedure. Tranexamic acid In ‘Packing in Endoscopic Sinus Surgery: Is It Really Required?” Ron Eliashar [31] concludes that Merocel packing or a hemostatic agent (microfibillar collagen or tranexamic acid) was used only when bleeding continued for more than 5 minutes after completion of surgery Mahzad Ali mian, et al. [32] in the study, “The effect of intravenous tranexamic acid on blood loss and surgical field quality during endoscopic sinus surgery: a placebo-controlled clinical trial” says that Intravenous tranexamic acid effectively reduces bleeding and improves the surgical field during FESS. Tranexamic acid at low dose improved hemostasis significantly, is the opinion of Rowan Valentine while discussing the effect of
20th century biomaterials on intra operative hemostasis [7].
Conclusion
Keeping packs inside the nasal cavity in a conscious person is something very much unacceptable. But due to the lack of other methods everybody is ready to undergo this torture hoping for a better future with a clear nose. But this can be avoided if you are ready to take some more time. This method has been described in the text books and journals. This can be a help to the patients, and the Anesthesiologists who are looking after the patient with an obstructed airway while in recovery ,and a tremendous help when some patient is having Obstructive Sleep Apnoea Syndrome Septoplasty by putting multiple continuous trans septal sutures after an initial one or two quilting sutures for stabilizing the corrected septum with absorbable 4 zero polyglactin suturing material, without packs, clips or splints inside the nose is a very effective method of preventing hematoma, or synechiae inside the nose at the same time, avoiding all the problems with a foreign material inside the nose even though temporarily with an obstructed airway. Thus, Septoplasty can be a day care procedure. The only problem is the extra time required for putting the suture which is negligible when considering the advantages.
- This study was not funded from external agencies
- No animals were used for the study
- Informed consent was taken from all patients
- There are no conflicts of interest
References
-
Saharia PS (1988) Cartilaginous Septal Defects and Their Correction. Indian Journal of Otolaryngology 40(1): 12-15.
-
Erkan Eşki, Ismail Yilmaz (2015) Pack-free septoplasty: functional outcomes and complications. Ear Nose BogazIhtis Derg 25(5): 275- 278.
-
Adriaan F, Van Olphen (2008) The Septum; Michael Gleeson, et al. Scott-Brown’s Otorhinolaryngology Head and Neck Surgery; Seventh Edition; London, UK; Hodder Arnold; 1580: 185
-
Ferguson BJ (2008) Surgical correction of nasal obstruction, Ricardo L. Carren, et al. Operative Otolaryngology Head and Neck Surgery, Philadelphia, United States; Saunders Elsevier 1133.
-
Jeevan B Ramakrishnan (2016) Septoplasty and Turbinate Surgery in Melissa A Scholes & Vijay R. Ramakrishnan (eds), ENT SECRETS, Fourth Edition, Elsevier India, page 185.
-
Nabil Elsahy (200) Basic Septoplasty and Turbinate Reduction. Plastic and Reconstructive surgery of the Nose; First Edition; Philadelphia, United States, Saunders: 48: 48.
-
Stewart, Michael G, David L Witsell, Timothy L Smith, Bevan Yueh, et al. (2004) Development and validation of the Nasal Obstruction Symptom Evaluation (NOSE) scale 1." Otolaryngology—Head and Neck Surgery 130(2)2: 157-163.
-
Rowan Valentine (2009)et al in Advances in Biomaterials and Nasal Packing in Raj Sindwani (eds) Otolaryngological Clinics of North America, 42(5). **9.** Shan Tang, Asahuhosh kicker (2012) Should intranasal splints be used after nasal septal surgery**?** The Laryngoscope 122(8): 1647-1648. **10.** Veluswamy Anand, Sachin Handa, Santosh Shivaswamy (2012) Nasal septal clips: an alternative to nasal packing after septal surgery?. Indian Journal of Otolaryngology and Head & Neck Surgery 64(4): 346-350.
-
Abdullah Karatas, Filiz Pehlivanoglub, Mehti Salviza, Nuray Kuvatb, Isil Taylan Cebi, et al. (2016) The effects of the time of intranasal splinting on bacterial colonization, postoperative complications, and patient discomfort after septoplasty operations, Brazilian Journal of Otorhinolaryngol 82: 654-661.
-
Genç, Erkhan, Tan Ergin N, Banu Bilezikçi (2014) Comparison of suture and nasal packing in rabbit noses. The Laryngoscope 114(4): 639-645.
-
Awan, Mohammad Sohail, Moghira I (2008) Nasal packing after septoplasty: a randomized comparison of packing versus no packing in 88 patients. Ear, Nose & Throat Journal 87(11: 624-627.
-
Cukurova I, Cetinkaya E A, Mercan G C, Demirhan E, Gumussoy M, et al. (2012) Retrospective analysis of 697 septoplasty surgery cases: packing versus trans- septal suturing method. Acta Otorhinolaryngological italica 32(2): 111-114.
-
Plasencia Daniel PérezJuan, Carlos Falcón, Silvia Borkoski Barreiro, María Sacramento Bocanegra- Pérez b Mario, Vicente Barrero, et al. (2016) Transeptal suturing-a cost-efficient alternative for nasal packing in septal surgery. Brazilian journal of Otorhinolaryngology 82(3): 310-313.
-
Sashikanth J, Vivian M Yu, Peter Catalanom(2011) Endo‐nasal surgeries without nasal packing or splints‐A retrospective review of postoperative bleeding complications in 300 patients. The Laryngoscope 121(S5): s362.
-
Sarfaraz MB, Mandeep Gill, Doron D sommer, Alkis psaltis, Rondy schlosser, et al. (2013) Is nasal packing necessary after septoplasty? A meta‐analysis. International forum of allergy & rhinology 3(5): 418-424.
-
Cayonu Melih, Ayudin Acer, Eyup Horasanli, Aytug Atnunbag, Murat Salihoglu, et al. (2014) Comparison of totally occlusive nasal pack, internal nasal splint, and transseptal suture technique after septoplasty in terms of immediate respiratory distress related to anesthesia and surgical complications. Acta oto- laryngologica 134(4): 390-394.
-
Zeyyan Ehab, Munir Demir Bajin, Kudret Aytemir, Tanir yilmaz (2010) The effects on cardiac functions and arterial blood gases of totally occluding nasal packs and nasal packs with airway. The Laryngoscope 120(11): 2325-2330.
-
Ali maeed S, Al-shehri (2011) Assessment of complications of nasal packing after septoplasty. The Medical Journal of Cairo University 79(2).
-
Georgalas Christos, Rupert Obholzer, Martinez- Devesa P, Sandhu G (2006) Day-case septoplasty and unexpected re-admissions at a dedicated day-case unit: a 4-year audit. The Annals of The Royal College of Surgeons of England 88(2): 202-206.
-
Basha SI, Gupta D, Kaluskar (2005) Routine nasal packing follwoing nasal surgery—Is it necessary?. Indian Journal of Otolaryngology and Head & Neck Surgery 57(1): 69-71. [INLINE_TABLE:6:0]
-
Bernardo Maria Teresa, Sandra AlvesII, Nuno Barros Lima, Diamantino Helena, Artur Condé et al. (2013) Septoplasty with or without postoperative nasal packing? Prospective study. Brazilian journal of Otorhinolaryngology 79(4): 471-474.
-
Rajashri S M, Balasaheb Patil, Anjana Mohite (2013) Comparison of septoplasty with and without nasal packing and review of literature. Indian Journal of Otolaryngology and Head & Neck Surgery 65(2): 406- 408.
-
Naik K (2015) A novel way of trans-septal splint suturing without nasal packing for septoplasty. Indian J Otolaryngol Head Neck Surg 67(1): 48-50.
-
Korkut, Arzu Y (2010) A randomised prospective trial of trans-septal suturing using a novel device versus nasal packing for septoplasty. Rhinology 48(2): 179.
-
Naghibzadeh Bijan, Ali Asghar Peyvandi, Ghazal Naghibzadeh (2011) Does post septoplasty nasal packing reduce complications?. Acta Medica Iranica 49(1): 9-12.
-
Eşki Erkan, Güvenç IA, Hızal E, Yılmaz I (2014) Effects of nasal pack use on surgical success in septoplasty. Kulak Burun BogazIhtis Derg 24(4): 206- 210.
-
Şahin C, Aras H İmer (2014) Influence of nasal pack removal on patients' anxiety after septoplasty. Kulak burun bogaz ihtisas dergisi: KBB= Journal of ear, nose, and throat 25(5): 266-270.
-
Eliashar Ron, Menachem Gross, Jay Wohlgelernter (2006) Packing in endoscopic sinus surgery: is it really required?. Otolaryngology—Head and Neck Surgery 134(2): 276-279.
-
Nuhi, Saeedollah, Ali Goljanian Tabrizi, Leyla Zarkhah, Bahram Rashedi Ashrafi (2015) Impact of Intravenous Tranexamic Acid on Hemorrhage During Endoscopic Sinus Surgery. Iranian journal of otorhinolaryngology 27(82): 349-354.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review