BALGI'S Flap: A Safe and Reliable Option in Small and Medium Defect of the Oral Cavity
The Balgi’s flap takes its name from the first parts of the surnames of the two authors describing this flap (Balercia and Girotto). This flap comes from the necessity of mucosal reconstruction after resection of small-medium size oral cancers (T1-T2) at the level of the oral cavity since it uses the whole mucosal cheek area as a source for reconstruction. Particularly it addresses the better reconstruction of the lateral edge of the tongue and lateral floor of the mouth, alveolar process and also the mandibular trigone.
Surgical Technique
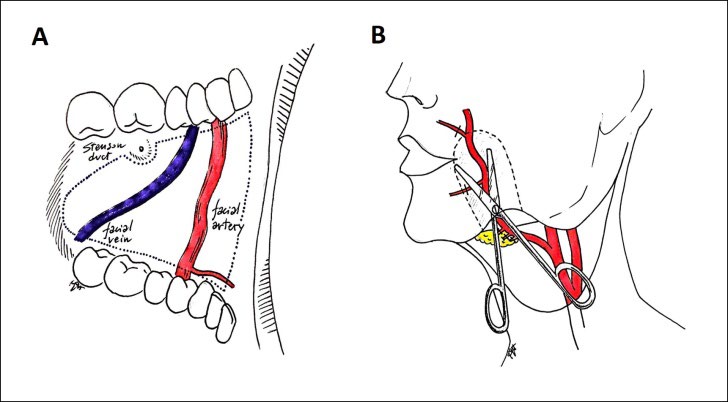
This flap is composed by a layer of mucosa, submucosa and muscle in monobloc with the underlying facial artery. The extension of the mucosal area is represented by the whole mucosal cheek with exception of the papilla of the Stenson’s duct at the level of the upper molar region (II molar generally). The anterior limit arrives 1-1,5 cm from the oral commissure.
Clinical Note
Posteriorly the height of the mucosal paddle, which anteriorly extends from the upper vestibular fornix to the lower fornix, decreases progressively in a triangular shape in front of the anterior mandibular ramus and external oblique line. Thus the Balgi’s flap has an almost triangular shape anchored inferiorly by the underlying facial artery (Figure 1). It is different by the FAMM (Facial artery mio mucosal flap) flap described by Pribaz, et al. because all of the mucosa in circumferentially incised and no mucosal pedicle is present [1].
We generally begin the dissection by retracting the lips and cheek and incising the vertical retro commissural edge at approximately 1-1,5 cm behind the oral commissure and red lip. It is advisable to priory detect the position of the facial artery which run in an almost vertical pattern by Doppler or palpation. First we deepen the dissection identifying the buccinators muscle and progressively proceeding posteriorly in the fat tissue until the detection of the facial artery. During this part of the procedure it is easy to meet the labial arteries travelling horizontally. After ligation to the labial artery it is possible to address the upper oblique edge in the same way. Preceding inferiorly the facial vein comes on sight in a almost vertical direction. After the incision of the lower mucosal edge, we ligate the facial artery in its upper pole. The facial vein was never preserved in any of our cases. In all of the cases we never observed discoloration of the mucosal flap or clinical signs of ipoperfusion or venous congestion.
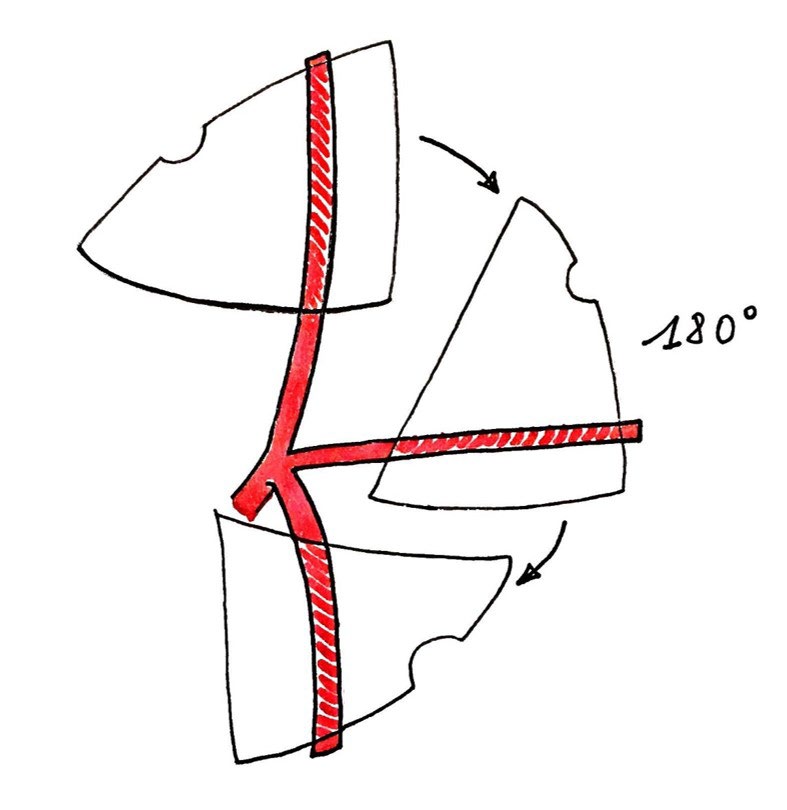
The dissected flap is now ready to rotate in any direction or twisted on its axis or passed inferiorly below the mandible to perform the required reconstruction (Figure 2).

It can be performed in association with the neck dissection and must be planned priory in the way to preserve the facial artery along its course (it is also possible to prepare part of the artery from below creating a tunnel above the facial artery, on the most external part, which correspond to a tunnel below the facial artery when we address the flap from the oral cavity [2, 3, 4].
This simple maneuver strongly decreases the dissecting surgical time and it is possible to introduce a flat surgical instrument into this pocket in the way to identify it when we dissect from the inside of the mouth. Performing the dissection of Robbins’ level II it is mandatory to preserve the facial artery all along its course and ligate the small arterial vessels entering the submandibular gland.
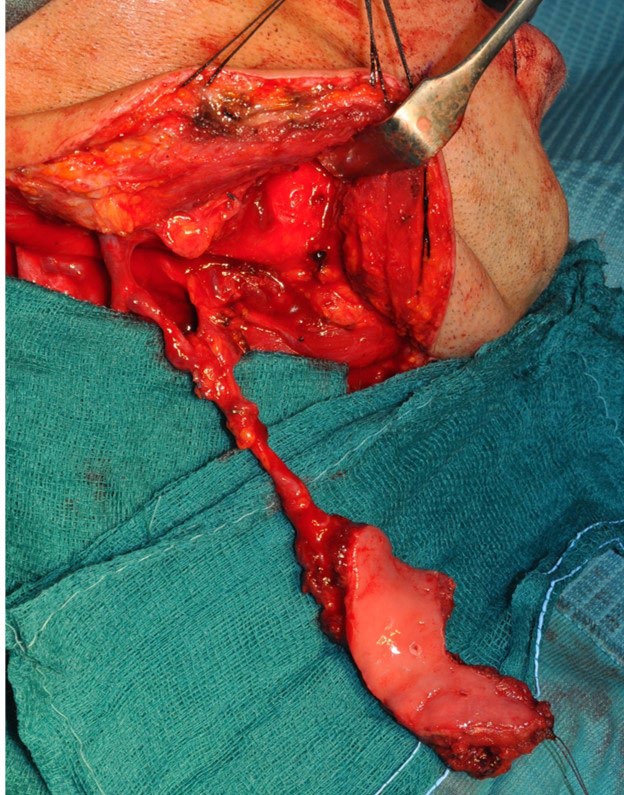
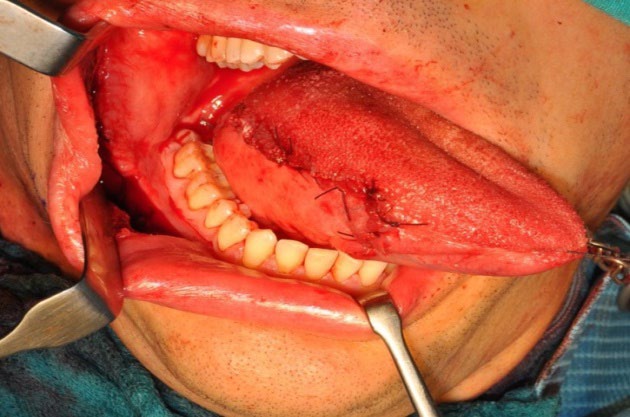
Once the neck dissection is performed with preservation of the facial artery, the tumor resection is done. Reconstruction is conducted with the Balgi’s flap as planned. After the positioning of the flap in the proper position, the posterior part of the cheek woud can be closed with the exteriorization of the Bichat fat pad. Mucosization of the defect proceed in the usual manner. Aggressive physiotherapy is mandatory in the post-operative period in the way to maintain adequate mouth opening (Figures 3-5).

Discussion
The ideation of this flap by the authors comes by some observations, some of them completely accidental: a) The first patient of our series received this reconstruction because of a fortuitous event which was the lesion of the facial vein during an attempted execution of a Zhao’s flap [5, 6]. The vein was injured in a position where the repair was impossible and the mucosal paddle has already been 75% elevated. After the lesion of the facial vein we didn’t observed any change in colour and bleeding of the mucosa thus we proceeded with the reconstruction. b) During the following days we didn’t observed any clinical sign of necrosis or perfusion reduction. The Authors observed regular intraoral healing without contraction or distortion of the mucosal paddle. c) The preservation of the facial artery and vein during the neck dissection it is not always easy, mainly because of oncological reasons. The dissection and preservation of the facial vein requires prolonged manipulation of Robbins’ level II, but the preservation of the facial artery and contemporary linfo-areolar cleaning of level II is possible and feasible without increasing the difficulty of the neck dissection. d) In the cheek, the facial vein, much posterior, and the facial artery, much anterior, have a divergent caudal direction. This reason implies that, preserving both vessels, the tridimensional movements of the mucosal flap could be quite difficult and limiting the direction of the orientation more than if the pivot point is only one (i.e. facial artery) [7, 8]. Particularly, in the cases where we preserved both vessels we had many doubts about the venous drainage because of kinking or twisting of the vein itself.
On the basis of this observation in the last five years we started ligating the facial vein without any attempt of preservation and we didn’t observed any clinical problem such as prolonged healing time, marginal necrosis or flap loss. In one case only where we elevated a very wide mucosal flap extending much anteriorly, approximately to the retro commissural region, we observed a post-operative asymmetrical elevation of the corner of the mouth, maybe because of inclusion on the flap of part of the modulus. This case was managed with repeated injection of Botox in the contralateral depressor anguli oris muscle every 5-6 months.
This flap can be consider a simplification of the other local mucosal flaps described by other authors like Pribatz, et al. [1]. It is based on the facial artery only and includes a wide mucosal area which is represented by the whole cheek area (with exception of the Stenson’s or parotid duct).
This arterial flap is a simplified option for oncological reconstruction which allows the surgeon to obtain mucosal lining in small-medium size reconstructions. This flap can be considered the mucosal variation of the “tulip flap” described by Cologlu, et al. [9] which was a skin flap based on the superficial temporal artery. Like the “tulip flap”, the Balgi flap is based on an artery only but it differs on the large amount of tissue, in this case cheek mucosa, which is rotated and perfused by a single artery.
We believe that this flap can increase the daily use of mucosal flaps for oncological intraoral reconstrution because this experience brought us to believe that venous drainage of the mucosal cheek is probably demanded to vasa vasorum better than the facial vein and thus we can performed a simpler flap without inclusion of the vein in the flap.
We also could also think that the methabolic need of the mucosa is very poor. Further studies of microcirculation of this flap are going on to determine which is the true reason of the success of this flap.
References
-
Pribaz J, Stephens W, Crespo L, Gifford G (1992) A new intraoral flap: facial artery musculomucosal (FAMM) flap. Plast Reconstr Surg 90(3): 421-429.
-
Ayad T, Xie L (2015) Facial artery musculomucosal flap in head and neck reconstruction: A systematic review. Head Neck 37(9): 1375-1386.
-
Dolderer JH, Hussey AJ, Morrison WA (2010) Extension of the facial artery musculomucosal flap to reconstruct a defect of the soft palate. J Plast Surg Hand Surg 45(4-5): 208-211.
-
Matros E, Swanson EW, Pribaz JJ (2010) A modification of the facial artery musculomucosal flap for palatal reconstruction in patients with intact dentition. Plast Reconstr Surg 125(2): 645-647.
-
Zhao Z, Zhang Z, Li Y, Li S, Xiao S, et al. (2003) The buccinator musculomucosal island flap for partial tongue reconstruction. J Am Coll Surg 196(5): 753-760.
-
Zhao Z, Li S, Yan Y, Li Y, Yang M, et al. (1999) new buccinator myomucosal island flap: anatomic study and clinical application. Plast Reconstr Surg 104(1): 55-64.
-
Ferrari S, Ferri A, Bianchi B, Varazzani A, Giovacchini F, et al. (2016) Oncologic safety of facial artery myomucosal flaps in oral cavity reconstruction. Head Neck 38.
-
Van Lierop AC, Fagan JJ (2008) Buccinator myomucosal flap: clinical results and review of anatomy, surgical technique and applications. J Laryngol Otol 122(2): 181- 187.
-
Cöloğlu H, Koçer U, Oruç M, Sahin B, Ozdemir R (2007) Axial bilobed superficial temporal artery island flap (tulip flap): reconstruction of combined defects of the lateral canthus including the lower and upper eyelids. Plast Reconstr Surg 119(7): 2080-2087.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review