Small Intestinal Tubulovillous Adenoma: A Rare Case Report
Introduction: Small bowel adenoma is very rare disease and most common location in duodenum. Ileal adenoma is very rare disease. Case presentation: We report the case of 42 years old male. Presenting with an upper recurrent abdominal pain, nausea, vomiting. Pain was sudden onset presenting 4 days ago. Blood examination: WBC was 8.6*103g/dl, PLT=149*103/ul, CRP was 38.60mg/l Trans abdominal ultrasound: Bowel loops dilated up to 3 cm PA erect Abdominal Radiography: Many air- fluid level in abdomen Exploratory laparotomy: Small bowel obstruction due to ileal tumor. Operation was right hemicolectomy. Anastomosis was side to side.
Introduction
The small bowel accounts for 75% of the length and 90% of the mucosal surface area of the gastrointestinal tract, fewer than 3% of gastrointestinal malignancies arise in this organ [1, 2]. Small bowel adenoma is very rare disease and most common location in duodenum [3, 4, 5, 6]. Ileal adenoma is very rare disease [1, 2, 3, 4]. As in the colon, small bowel adenomas are histologically classified as tubular, tubulovillous, or villous [5, 7]. Most common in the periampullary region, they can develop throughout the small bowel mucosa [1, 2, 3]. Increased size correlates with malignant potential, and excision is advised when diagnosis is established, often as an incidental finding [4, 5, 6, 7, 8, 9]. Adenomas larger than 2 cm in diameter should be considered worrisome for malignancy. Large, periampullary duodenal adenomas may present with obstructive jaundice [4, 5, 6]. In these cases ultrasound will reveal evidence of biliary obstruction, prompting upper endoscopy with endoscopic retrograde biliary and pancreatic duct evaluation (endoscopic retrograde cholangiopancreatography), which will reveal the presence of the ampullary lesion [1, 2, 3]. Without these physical signs to direct the workup, duodenal adenomas are detected during evaluation of gastrointestinal blood loss or other abdominal complaints, with either contrast upper gastrointestinal series or EGD, which are equally sensitive in most series [3, 6]. Adenomas usually appear as intraluminal filling defects and may be pedunculated [4, 6]. CT scan may differentiate adenoma from carcinoma, as carcinomas are often associated with bowel wall thickening [2, 4]. Endoscopic ultrasound is becoming essential in the evaluation of duodenal adenomas to evaluate depth and to determine if mucosal excision or surgical resection is more appropriate [6]. Transduodenal local excision for small lesions is appropriate, while lesions larger than 3 cm in size have a high rate of associated malignancy and are most appropriately treated with either pancreas- sparing duodenectomy, or pancreaticoduodenectomy for larger lesions or periampullary tumors in suitable operative candidates [2, 8].
Although accounting for 30–50% of primary neoplasms of the small bowel, benign tumors are poorly characterized [1, 3, 6]. Half the patients with benign tumors are symptom free, and most will be diagnosed at the time of presentation with a surgical emergency such as obstruction, gastrointestinal hemorrhage, or perforation [4, 6, 8]. Gastrointestinal bleeding is the most common presenting complication, presumably a consequence of spontaneous necrosis when the benign lesion outgrows the available blood supply [2, 6]. Once these lesions are diagnosed, surgical segmental intestinal resection is appropriate [3, 5]. While local excision via endoscopic mucosal resection or operative enterotomy with submucosal excision is feasible, it is generally not possible to grossly differentiate between benign and malignant lesions [2, 3, 4]. Hence, transmural resection is preferred for indeterminate lesions [2, 3, 4]. Open and laparoscopic approaches have been described [2, 3]. Most of these tumors are clinically silent [3, 4, 5, 6]. Autopsy series have identifi ed incidental small bowel tumors in 0.2–0.3% of hospital deaths-a rate 15 times the operative incidence of small bowel resections for tumors [7, 9]. Small bowel tumors are more prevalent in older than in younger patients, and a recent analysis identified that over 65% of patients with small bowel adenocarcinoma were age 60 or older [7]. The proportion of small bowel tumors that are benign varies from 14 to 52% in different series, a disparity explained by the failure to detect the typically asymptomatic benign lesions [4, 6]. There are no satisfactory explanations for the observed variation in prevalence of small bowel tumors around the world [5]. Men are more likely to develop small bowel neoplasms than women, with a male preponderance reported for both benign and malignant tumors [1, 2, 3, 4].
Case report
A 42-year-old male presented to the emergency department with complaints of severe abdominal pain, vomiting, and abdominal distension for four days. He reported not passing stools for three days. On examination, he was conscious, oriented, and his vitals were stable. On digital rectal examination, the rectum was empty. Blood examination: WBC was 8.6*103g/dl, PLT=149*103/ul, CRP was 38.60mg/l (Table 1).
| Reference | V/18 | V/20 | V/21 | |
|---|---|---|---|---|
| WBC | 4-10*103 | 5.7 | 7.3 | 8.6 |
| PLT | 150-500*103 | 149 | 126 | 160 |
| Biochemistry | ||||
| CRP | 0-5 mg/l | 38.6 | 162.97 | 97.5 |
| BUN | 0.5-8.3 mmol/l | 8.6 | 7.7 | |
| T.bilirubin | 0-5.7 umol/l | 13.5 | ||
| D.bilirubin | 0-21 umol/l | 30.8 |
Table 1: Changes of blood analysis.
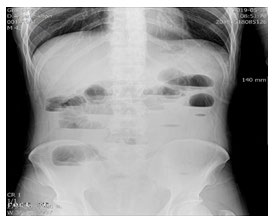
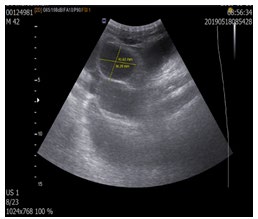
An ultrasound of the abdomen was done which showed dilated hyper-peristaltic small bowel loops of maximum caliber 3.0 cm and wall thickness (Figure 1). There was no free-fluid in the peritoneal cavity. Plain x-ray of the abdomen: Multiple air-fluid level in the small bowel loops (Figure 2).
We are the patient was decided for an emergency exploratory laparotomy. Intraoperatively, there were no bowel adhesions. A 3×1.5 cm well-defined firm intraluminal mass was palpable in the ileum about 15 cm proximal to the ileocaecal junction. The bowel loops proximal to the mass were dilated and the loops distal to it were collapsed. The mass was motionless and softer, was found impacted at the transition area in the bowel. This mass was may be bowel cancer; therefore we decided right hemicolectomy operation. Operation: Exploratory laparotomy, right colectomy, anastomosis side to side (Figure 3A-F). During surgery figure:

Figure 3A: Small bowel adenoma with displasia. a(Ileum), b(cecum), c(adenoma).
Figure 3B: Small bowel adenoma with displasia (The adenoma is indicated by a white arrow).
Figure 3C: Small bowel adenoma with dysplasia.
Figure 3D: Small bowel adenoma with dysplasia.
Figure 3E: Small bowel adenoma with dysplasia.
Figure 3F: Ileocolic anastomosis side to side.
Histologic analysis: Pathologic diagnosis
- Small bowel: Tubulo-villous adenoma with low grade dysplasia. Perifocal ulcerative ileitis, hemodynamic disorders.
- Cecum: Congestion
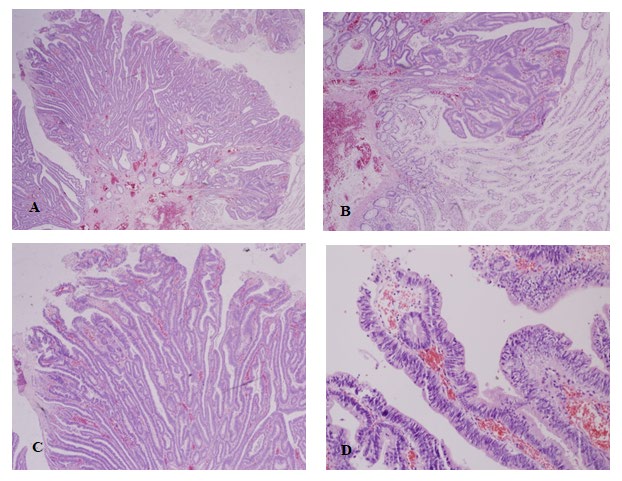
Figure 4A-D: Tubulo-villous adenoma with low grade dysplasia.
Discussion
Small bowel adenoma was first described by Perry in 1893 and was named as duodenal papilloma [1, 2]. The adenoma is usually located in the colon [3, 4]. However, during endoscopic examination, 0.4% occur in the duodenum [1, 3, 4]. Adenomas make up about one-third of benign tumors and occur in all parts of the small bowel [4, 7]. They make up <10% of all duodenal polyps, although they are most commonly located in the second part of the duodenum, particularly in the vicinity of the ampulla of Vater, which is the site of 80% of all small bowel adenomas [7, 8, 9]. Of these, two-thirds are periampullary, possibly reflecting exposure to bile [2, 6]. Surgical series of resected ampullary adenoma report in situ or frank adenocarcinoma in 34–40% of patients [7]. Local recurrence is common for periampullary adenomas treated with excision only: 40% at 10 years, 25% of which were malignant, in a recent retrospective series from the Mayo clinic. For those treated with excision only, annual surveillance with endoscopy is appropriate.
While some adenomas are entirely duodenal, others may involve both the ampulla and the major biliary and pancreatic ducts, to the point where it may be impossible to determine the true site of origin of the tumor [8, 9]. Intestinal benign tumor include polyps such as found in familial adenomatous polyposis (multiple small bowel polyps), Peutz-Jeghers syndrome and Gardner’s syndrome [6, 7, 8]. These tumors are named according to the tumor stage as well as its morphology, villous adenoma, papillary adenoma, villous papilloma, tubulovillous adenoma, and villoglandular polyp [1, 2, 3]. Tubulovillous adenomas may include small, sessile, or polypoid lesions [6]. Though they are mostly asymptomatic, sometimes they may present with the signs and symptoms of jaundice (obstructive jaundice), abdominal pain, melena, hematochezia, fever, malaise or weight loss [2, 3, 4]. Tubulovillous adenomas show a combination of tubular and villous architecture (villous component greater than 25%) and are usually intramural with intraepithelial tumor cells [2, 5].
Tubular adeomas have a tubular architecture with the surface epithelium showing low-grade displasia that extends downward in the base [6, 7, 9]. These can show focal areas of high-grade dysplasia with architectural complexity and marked cytologic atypia [1, 6, 7, 9]. Focal high-grade dysplasia does not have a metastatic potential [6, 7, 9]. The tubulovillous adenomas Figure 4) show a combination of tubular and villous architecture (villous component greater than 25%) [3, 4, 5, 6]. Villous adenoma displays a predominant villous architecture (greater than 75%) and has a greater propensity for malignant transformation [1, 2, 3]. All of these can have focal areas of pseudo invasion that should not be interpreted as intramucosal carcinoma [1, 2, 3]. The conventional adenomas show KRAS mutations [5, 8].
Conclusion
The case we presented was a rare 1.5-cm adenoma with ulcerative lesions located in the small intestine. This case was diagnosed during the operation. Histological examination revealed villo-tubular adenoma. The patient was completely cured and discharged from the hospital.
References
-
Sakorafas GH, Friess H, Dervenis CG (2000) Villous tumors of the duodenum: biologic characters and clinical implications. Scand J Gastroenterol 35(4): 337-344.
-
Church JM, McGannon E, Hull Boiner S, Sivak MV, Van Stolk R, et al. (1992) Gastroduodenal polyps in patients with familial adenomatous polyposis. Dis Colon Rectum 35(12): 1170-1173.
-
Hartenfels Ina M, Dukat A, Burg J, Hansen M, Jung M (2002) Adenomas of Vater’s ampulla and of the duodenum. Presentation of diagnosis and therapy by endoscopic interventional and surgical methods. Surgeon 73(3): 235-240.
-
Pourmand K, Itzkowitz SH (2016) Small bowel neoplasms and polyps. Curr Gastroenterol Rep 18(5): 23-25.
-
Komorowski RA, Cohen EB (1981) Villous tumors of the duodenum: a clinicopathologic study. Cancer 47(6): 1377-1386.
-
Johri V, Arshi SJ (2013) Tubulo-villous adenoma of first part of duodenum-an unusual presentation. Int J Curr Res 5: 123-126.
-
Crawford J (1999) The gastrointestinal tract. In: Cotran RS, et al. (Eds.), Robbins pathologic basis of disease 6th (Edn.), Philadelphia, Pa: Saunders pp: 775-844.
-
Niwa A, Kuwano S, Tomita H, Keita Kimura , Yukiya Orihara, et al. (2017) The different pathogeneses of sporadic adenoma and adenocarcinoma in non- ampullary lesions of the proximal and distal duodenum. Oncotarget 8(25): 41078-41090.
-
Chappuis CW, Divincenti FC, Cohn Jr I (1989) Villous tumors of the duodenum. Ann Surg 209(5): 593-599.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review