Intraneural Lipoma of the Median Nerve at the Forearm Causing Median Neuropathy: A Case Report
Intraneural lipomas are fat tumors of peripheral nerve and their branches. They are presented either as asymptomatic regional swelling or as lesions causing compressive neuropathy, especially when developed in locations with limited potential of expansion, e.g. the carpal tunnel. The median nerve is the most affected nerve and the wrist and the hand the most common sites related to median neuropathy. We present a case of a 72 years old woman with an intraneural lipoma of median nerve at the forearm with symptoms of median neuropathy, which is a rather unusual site of nerve compression.
Introduction
Intraneural lipomas are benign soft tissue masses within the epineurium of a peripheral nerve. Well separated from the ambient structures, microscopically, they are composed of adipose tissue without any neural elements. They are located, most frequently, in the upper extremity, especially in the median nerve [1]. Notably, intraneural lipomas of the median nerve have been described in all the distance from the elbow to the hand, yet they are more common at the wrist and hand, provoking compressive symptoms such as carpal tunnel syndrome [2, 3]. Due to its unusual location, we present a case of intraneural lipoma of median nerve at the forearm, causing symptoms of median neuropathy.
Case Presentation
A 72 years old woman presented at our outpatient clinic complaining for night pain and paresthesias of her right hand and numbness in radial three digits. She had already visited a physician, who had suggested an electromyography (EMG), attributing the symptoms to carpal tunnel syndrome. The results of the EMG were consistent with median neuropathy thus, she was prescribed nonsteroidal anti-inflammatory drugs and she used a night splint for a month. Persistent symptoms lead her to ask for a more effective therapy; consequently, she visited a hand orthopaedic surgeon at our department.
Patient’s distribution and the electromyographic findings indicated median neuropathy. Physical examination was not clearly positive for carpal tunnel syndrome, as Durkan’s and Tinel’s tests were controversial. However, a palpable elastic mass was found out at the palmar aspect of the forearm, which was not noticed by the patient so far. Further investigation with an MRI was suggested and a week later the patient returned with the results, illustrating a tumor with adipose tissues signal adjacent to the median nerve. Therefore, a surgical excision was decided.
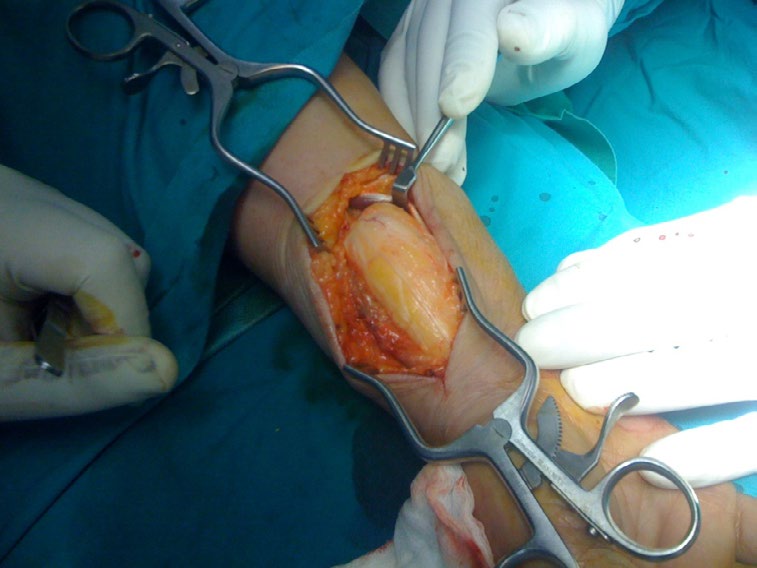

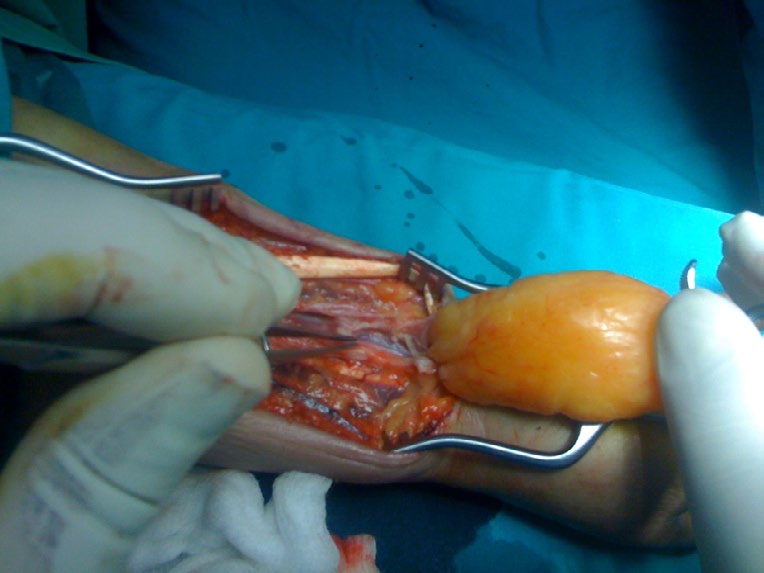
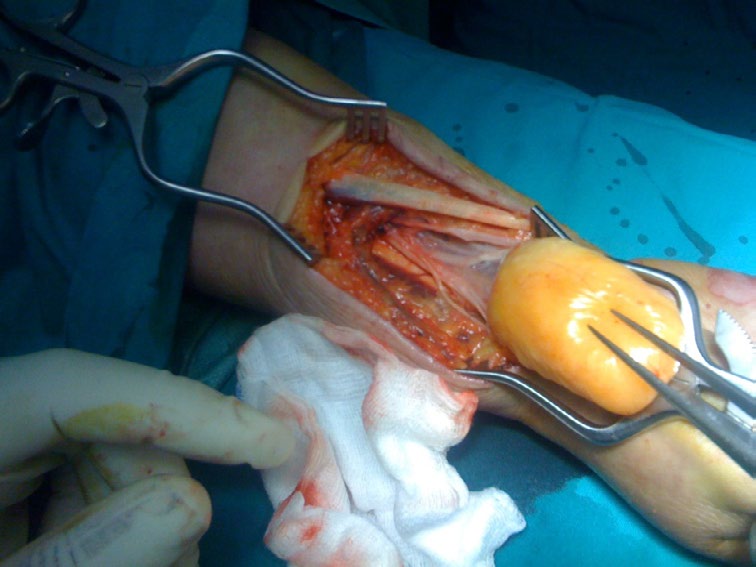
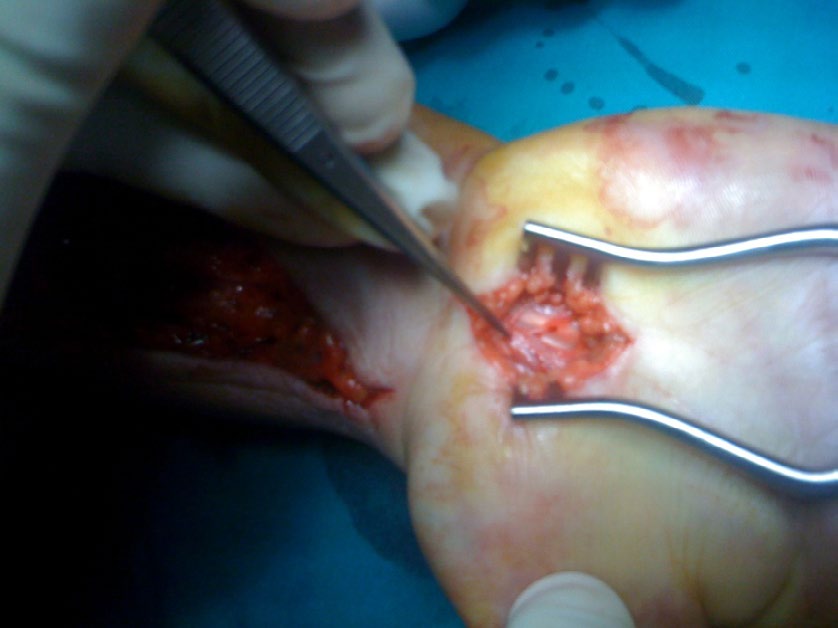
Figures 1-4: Recognition, preparation and excision of the lesion within the epineureum of the median nerve.
Under general anesthesia, Henry’s forearm approach from middle to distal third of the right forearm was performed. After superficial and deep dissection, a mass within the epineurium of the median nerve was detected (Figures 1-4). Carefully, the epineurium was separated from the lesion and the lesion was distinguished from the underneath medial nerve. The mass was exceeded en bloc (Figure 5).
An additional release of the carpal tunnel was performed, to be sure that the neurological symptoms would be relieved, in case of supplementary compression of the median nerve at that site (Figure 6).

The histological analysis of the mass revealed a lipoma without any mixture of other tissue’s elements. In conclusion, the tumor was an intraneural lipoma. One month later patient’s symptoms were improved and three months after the excision she was totally free of symptoms.
Discussion
Benign fatty tumors restricted to peripheral nerves are rare, yet they may cause diagnostic and treatment problems. There are two main categories of lipomas causing peripheral nerve neuropathy, the extrinsic and the intrinsic. The former may squeeze the nerve outside the epineurium and produce symptoms of nerve compression [4]. The latter are under the epineurium and are separated into three types of growth, the intraneural or encapsulated lipoma, the macrodystrophia lipomatosa and the lipofibromatosus hamartoma or diffusely infiltrating fibrofatty tumors. The first type, the intraneural lipoma, arises from the adipose tissue of the epineural sheath and is well encapsulated and distinct from the neural elements [5]. The second type, the macrodystrophia lipomatosa, is a rare congenital disorder which is characterized by the disproportionate overgrowth of fibroadipose tissue at a part or the whole of an extremity, causing principally cosmetic rather than functional problems [6]. The third type, the lipofibromatosus hamartoma, presents the fatty infiltration of a nerve and has the worse prognosis; therefore, early diagnosis and decompression of possible compression sites are necessary to maintain the function of the limb [7].
In literature, the intraneural lipoma has been described as a mass of many nerves, both of the upper and of the lower extremity. In the arm, except for the median nerve [8] which is the most common site of development, the ulnar nerve [1], the posterior interosseous nerve [9], the superficial radial nerve [10] and digital nerves [11] have been afflicted. In the leg the sciatic nerve [12], the tibial nerve [13], the common peroneal nerve [1] and the superficial peroneal nerve [14] have been recorded as locations of the lesion.
Intraneural lipoma of the median nerve most frequently appears in the wrist and hand, causing compression of the nerve due to restricted space, requiring excision and carpal tunnel release [15]. The forearm is a rare location of the tumor and median neuropathy owing to a mass at this site is even rarer. The primary reason for excision is the cosmetic and psychological impact of a mass at the arm, even though it is benign; still, only one occasion of nerve compression has been reported in the literature and there was significant improvement in patient’s symptoms after the mass excision [3], as in our case. Proper physical examination and clinical suspicion are important to detect such lesions and provide adequate therapy, particularly when intraneural lipomas are developed in unusual locations.
Conclusion
Intraneural lipomas are benign fatty tumors within the epineureum of peripheral nerves. The median nerve is the most commonly affected nerve and the wrist is the most frequent location of development causing carpal tunnel syndrome symptoms. We present a rare case of an intraneural lipoma of the median nerve at the forearm causing median neuropathy. The site of development is unusual and the most interesting about it is that it was detected due to the symptoms of median nerve pressure. Intraneural lipoma of the median nerve at the forearm may be a cause of median neuropathy and physical examination and clinical suspicion are essential to detect and excise them to reveal patient’s symptoms.
Highlights
- Intraneural lipoma at the forearm of the median nerve is a rare cause of median neuropathy
- Excision of the lesion can treat patient’s symptoms
- Proper physical examination and clinical suspicion are important to detect such lesions
References
-
Marek T, Amrami KK, Mahan MA, Spinner RJ (2018) Intraneural lipomas: institutional and literature review. Acta Neurochir (Wien) 160(11): 2209-2218.
-
Ha JF, Teh BM, Abeysuriya DT, Luo DY (2012) Fibrolipomatous hamartoma of the median nerve in the elbow: a case report. Ochsner J 12(2): 152-154.
-
Okubo T, Saito T, Mitomi H, Takagi T, Torigoe T, et al. (2012) Intraneural lipomatous tumor of the median nerve: Three case reports with a review of literature. Int J Surg Case Rep 3(9): 407-411.
-
Teles AR, Finger G, Schuster MN, Gobbato PL (2016) Peripheral nerve lipoma: Case report of an intraneural lipoma of the median nerve and literature review. Asian J Neurosurg 11(4): 458.
-
Terzis JK, Daniel RK, Williams HB, Spencer PS (1978) Benign fatty tumors of the peripheral nerves. Ann Plast Surg 1(2): 193-216.
-
Prasetyono TO, Hanafi E, Astriana W (2015) A Review of Macrodystrophia Lipomatosa: Revisitation. Arch Plast Surg 42(4): 391-406.
-
Razzaghi A, Anastakis DJ (2005) Lipofibromatous hamartoma: review of early diagnosis and treatment. Can J Surg 48(5): 394-399.
-
Houpt P, Storm van Leeuwen JB, van den Bergen HA (1989) Intraneural lipofibroma of the median nerve. J Hand Surg Am 14(4): 706-709.
-
Patel AP, Aoun SG, Al Tamimi M (2018) Intraneural Posterior Interosseous Nerve Lipoma with Complete Paralysis: Case Report and Review of the Literature. Cureus 10(5): e2689.
-
Balakrishnan C, Bachusz RC, Balakrishnan A, Elliot D, Careaga D (2009) Intraneural lipoma of the radial nerve presenting as Wartenberg syndrome: A case report and review of literature. Can J Plast Surg 17(4): 39-41.
-
Rusko RA, Larsen RD (1981) Intraneural lipoma of the median nerve--case report and literature review. J Hand Surg Am 6(4): 388-391.
-
Chiao HC, Marks KE, Bauer TW, Pflanze W (1987) Intraneural lipoma of the sciatic nerve. Clin Orthop Relat Res (221): 267-271.
-
Krzywosinski TB, Bingham AL, Fallat LM (2017) Intraneural Lipoma of the Tibial Nerve: A Case Report. J Foot Ankle Surg 56(1): 125-128.
-
Sabapathy SR, Langer V, Bhatnagar A (2008) Intraneural lipoma associated with a branch of the superficial peroneal nerve. J Foot Ankle Surg 47(6): 576-578.
-
Gennaro S, Merciadri P, Secci F (2012) Intraneural lipoma of the median nerve mimicking carpal tunnel syndrome. Acta Neurochir (Wien) 154(7): 1299-1301.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review