Inguinal Hernia Containing Ovary/Uterus: Presentation and Management of 4 Cases
Background: Inguinal hernia is common surgical condition in pediatric age group with an estimated incidence of 1% to 5% in term new born. Inguinal hernia is more common in boys than girls. The content of inguinal hernia in both male and female patients is usually small bowel, presence of uterus or ovary is extremely rare incidental finding. Material and Methods: We retrospectively review the files of the 4 patients managed with inguinal hernias containing uterus and /or ovary in the last 2 years. Their presentation, treatment and outcome of the treatment were reviewed and document. Results: All the patients were managed as day cases surgeries and followed up for at least 6month. None of the patient developed recurrence, one of them had surgical site infection which was treated with dressing and antibiotics. Conclusion: Inguinal hernia containing ovary is a rare occurrence in female children but the outcome of its management seems to be good.
Introduction
Hernia is defined as a protrusion of a portion of an organ or tissue through an abnormal opening or defect in the cavity containing it [1]. In children it is usually an indirect hernia hence the defect is the internal inguinal ring. Inguinal hernia is pediatric age group is mostly congenital, though may not be apparent at birth [1, 2]. The incidence of inguinal hernia in children is estimated to be 1% to 5% with male preponderance, male female ratio of 3- 10:1 [3]. Female inguinal hernia usually contained small intestine but some time may contain ovary, uterus or both [3, 4].
Case Report
Case 1
unit with complain of recurrent left groin swelling for 1 year which is more while coughing or crying but disappear on lying down. No history of abdominal pain, abdominal distension or constipation. Had occasional cough but no chest pain or difficulty in breathing. On examination there was a reducible swelling in the left inguinal region which was non tender, firm in consistency. Respiratory rate(RR) was 14 cycle per minute, pulse rate (PR) of 122beat per minute. Other systems were essentially intact. Abdominal ultrasound (USS) reveals normal study, packed cell volume (PCV) was 38% and urinalysis was essentially negative.
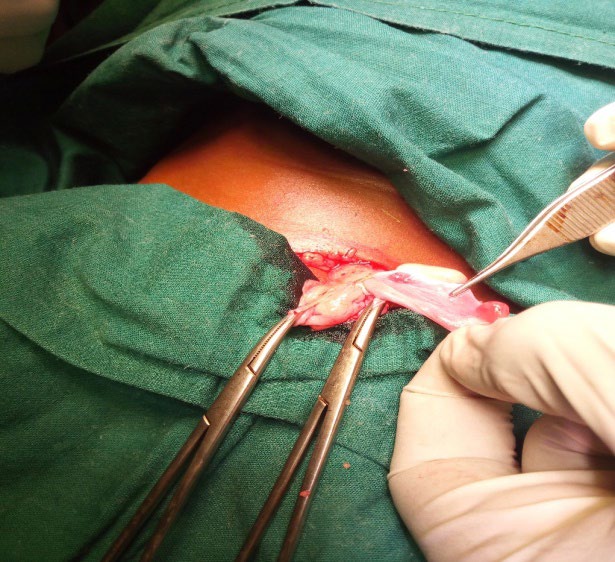
Patient had herniotomy as a day case under general anesthesia, intra operatively the hernia sac contained ovary which was pushed in to the pelvic cavity and herniotomy was effected (Figure 1). Patient did well post operatively, was seen a week after the operation and was followed up in the clinic for up to 6month before they lost to follow up.
Case 2
An 8month old girl who presented to our pediatric surgical unit with complain of recurrent left groin swelling for 3 months which is more while crying but disappear on lying down. No history of abdominal pain, abdominal distension or constipation. No cough, chest pain or difficulty in breathing. On examination there was a reducible swelling in the left inguinal region which was non tender, firm in consistency. Respiratory rate(RR) was 16 cycle per minute, pulse rate (PR) of 132beat per minute. Other systems were essentially intact. Abdominal ultrasound (USS) reveals normal study, packed cell volume (PCV) was 34% and urinalysis was essentially negative. Patient had herniotomy as a day case under general anesthesia, intra operatively the hernia sac contained ovary which was pushed in to the pelvic cavity and herniotomy was effected (Figure 2).

Case 3
A 4year old girl who presented to our pediatric surgical unit with complain of recurrent right groin swelling for 8 months which is more on straining but disappear on lying down. Had occasional history of abdominal pain, but no abdominal distension or constipation. No cough, chest pain or difficulty in breathing. On examination there was a reducible swelling in the right inguinal region which was non tender, firm in consistency. Respiratory rate (RR) was 16 cycle per minute, pulse rate (PR) of 132beat per minute. Other systems were essentially intact. Abdominal ultrasound (USS) reveals a globular structure suspected to be the ovary within the inguinal sac, packed cell volume (PCV) was 32% and urinalysis was essentially negative.
Patient had herniotomy as a day case under general anesthesia, intra operatively the hernia sac contained both uterus and ovary which were pushed in to the pelvic cavity and herniotomy was effected (Figure 3). Patient did well post operatively, was seen a week after the operation noticed to has surgical site infection which was managed with daily wound dressing and is still on followed up in the surgical out-patients’ clinic.

Case 4
A 3year old girl who presented to our pediatric surgical unit with complains of recurrent right groin swelling for 1 year which is more while coughing or crying but disappear on lying down. No history of abdominal pain, abdominal distension or constipation. Had occasional cough but no chest pain or difficulty in breathing. On examination there was a reducible swelling in the right inguinal region which was non tender, firm in consistency, left inguinal region appears normal. Respiratory rate (RR) was 14 cycle per minute, pulse rate (PR) of 124beat per minute. Other systems were essentially intact. Abdominal ultrasound (USS) reveals normal study, packed cell volume (PCV) was 36% and urinalysis was essentially negative. Patient had herniotomy as a day case under general anesthesia, intra operatively the hernia sac contained ovary which was pushed in to the pelvic cavity and herniotomy was effected (Figure 1). Patient did well post operatively, was seen a week after the operation and was followed up in the clinic for up to 6month before they lost to follow up.
Discussion
Uterus-containing inguinal hernia is a rare condition in which the uterus and ovary are found in the inguinal hernial sac in female. The uterus may be free within the sac, adherent to the wall by adhesions or a true sliding component. However, in true sliding-type, one of the walls of the hernia sac is formed by the uterus itself [2] Inguinal hernias that contain the uterus and both ovaries are thought to be extremely rare [1, 2, 3]. Most of the patients with inguinal hernias present in infancy, however some may not be noticed till childhood or even adulthood. Diagnosis of an inguinal hernia is mainly clinical by history and physical examination. Inguinal hernias appear usually as intermittent lumps/ swelling in the groin and mostly painless [1, 2, 4, 5]. Ultrasonography is a very effective tool to detect content of an inguinal hernia, but in some cases it is difficult to detect presence of a reproductive organs in infants [6, 7, 8]. Out of our 4 patients abdominal USS was able to detect suspected ovary in only one case.
The treatment for inguinal hernia is surgical which is plan as soon as the diagnosis is made usually as elective unless in the presence of complication like obstruction, strangulation, or incarceration [9, 10]. The ovary as the content of the hernia was discovered incidentally in 3 of our patients and all of our patients had herniotomy with in 3month of diagnosis based on the number of patients and available theatre space as against early operation as suggested by some authors to avoid vascular compromised [11, 12]. The operation involves high ligation of the sac except when the uterus or ovary formed part of hernial wall as sliding hernia where Bevan’s technique may be required [13]. The outcome of the treatment was satisfactory in all of our patients as reported in other studies [14]. Post- operative complications are rare as only 1 patient developed surgical site infection in the first week of the operation and subsided with in 2weeks of operation. This is similar to reports in other studies in the world.
Conclusion
Inguinal hernia containing ovary is a rare occurrence in female children but the outcome of its management seems to be good.
References
-
Abantanga FA, Lakhoo K. Inguinal and femoral hernias and hydrocele in children. Pediatric surgery for Africa a comprehensive text.
-
Cascini V, Lisi G, Renzo DD, Pappalepore N, Chiesa PL (2013) Irreducible indirect inguinal hernia containing uterus and bilateral adnexa in a premature female infant: report of an exceptional case and review of the literature. J Pediatr Surg 48(1): 17-19.
-
Graves GY, Mcllovoy DB, Green B (1951) Hernia of uterus, ovaries and tubes in a six week old infant. J Dis Child 81(2): 250-252.
-
Nuss D (1976) the management of hernias, hydroceles and undescendedtestes. S Med J 50(14): 548–549.
-
Ozbey H, Ratschek M, Schimpl G, Hollwarth ME (1999) Ovary in hernial sac: prolapsed or a descended gonad? J Pediatr Sur 34(6): 977-980.
-
Koak Y, Chaloner EJ (2002) Hernia ovary inguinale with ovulating luteal cyst: a case report. Grand Rounds 2: 32- 34.
-
Chen KC, Chu CC, Chou TY, Wu CJ (1998) Ultrasonography for inguinal hernias in boys. J Pediatr Surg 33(12): 1784- 1787.
-
Khanna PC, Ponsky T, Zagol B, Lukish JR, Markle BM (2007) Sonographic appearance of canal of Nuck hydrocele. Pediatr Radiol 37: 603-606.
-
Marinkovic SM, Kantardzic S, Bukarcia S, Grebeldinger M (1998) Pajic When to operate nonreducible ovary? Med Pregl 51(11-12): 537-540.
-
Boley SJ, Cahn D, Lauer T, Weinberg G, Klein HS (1991) The irreducible ovary: a true emergency. J Pediatr Surg 26(9): 1035-1038.
-
Beaunoyer M, Chapdelaine J, Bouchard S, Ouimet A (2004) Asynchronous bilateral ovarian torsion. J Pediatr Surg 39(5): 746-749.
-
Lau ST, Lee YH, Gaty MG (2007) Current management of hernias and hydroceles. Sem Pediatr Surg 16(1): 50-57.
-
Bradshaw KD, Carr BR (1986) Carr Ovarian and tubal inguinal hernia Obstet Gynecol 68(3): 50-52.
-
Usang UE, Sowande OA, Adejuyibe O, Bakare TIB, Ademuyiwa OA (2008) Day case inguinal hernia surgery in Nigerian children: prospective study. Afr J Paediatr Surg 5 (2): 76-78.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review