The Interest of the Modified Lateral Supramalleolar Flap in the Management for Defect of Ankle
Covering the defect of ankle substances as well as the defect of distal leg substances has long been a challenge for plastic surgeons. Through the experience of two clinical cases, we show the ease of survey, the clinical result and the effectiveness of the use of an externally supra-malleolar flap modified according to the Valenti technique for the coverage of the defects of substances.
Introduction
Covering the large loss of substance in the distal third of the leg and ankle remains difficult. Depending on their location, extent and terrain, we have a number of solutions using regional or remote flaps. A number of these flaps have been abandoned because of their uncertain fiability, surgical difficulty or important sequelae. Among these flaps is the external Supramalleolar flap, vascularized by an ascending branch of the fibular artery, which was first described by Masquelet, et al. in 1988 [1] and is unpopular because of its difficulty. Valenti has modified it, making it simpler and more reliable [2]. We illustrate its interest through this clinical case.
Surgical Technique
In dorsal decubitus position, under rachi anesthesia, after marking the external malleolus and the tibial crest. The future flap as well as the estimation of the location of the ramus perforans (about 5 cm from the tip of the lateral malleolus) is drawn beforehand on the lateral aspect of the leg. The skin palette is positioned more proximally, to increase the arc of rotation, with a size slightly larger than the area to be covered. The pivot point is shifted 2 cm more proximally. The procedure is started with an elongated S-shaped incision. A very superficial detachment is performed to expose the subcutaneous tissue. An incision of the medial edge of the flap opposite the tibial crest at the top, then the tibialis anterior muscle at the bottom for greater safety, followed by an incision of the upper and lateral edges of the flap, carrying the fascia and joining the plane of detachment is performed. The detachment of the deep face carrying the fascia (the procedure is safe since the arterial pedicle travels above the fascia) stops above the origin of the ramus which is neither located nor sectioned. The flap is then rotated around its axis (a subcutaneous tunnel can be used to return the flap to the recipient site), attached to the recipient area with grafting from the donor area.
Clinical Case 1
A 64-year-old patient, diabetic for 12 years, amputated his right big toe and left forefoot 10 years ago following frostbite lesions (monopodal support on the affected side only). Who presents an epidermoid carcinoma, 7.5 cm long axis, on the inner side of the ankle and the right forefoot (Figure 1), locally advanced (bone lysis), without lymph node invasion or distant metastases. Given the history of amputation of the contralateral limb, the decision is for a wide excision with reconstruction followed by complementary radiotherapy. Thus the patient underwent a carcinological excision removing the soft parts of the inner face of the ankle, the first metatarsal and the inner part of the medial cuneiform and the navicular bone (Figure 2), and immediate coverage by a lateral supra-malleolar flap by Valenti’s technique (Figure 3) with secondary grafting of the donor area. The evolution was good: no vascular or infectious complications (Figure 4) with a satisfactory functional result over a 10-month collection: mobility of the ankle preserved, walking with assistance possible.



Clinical Case 2
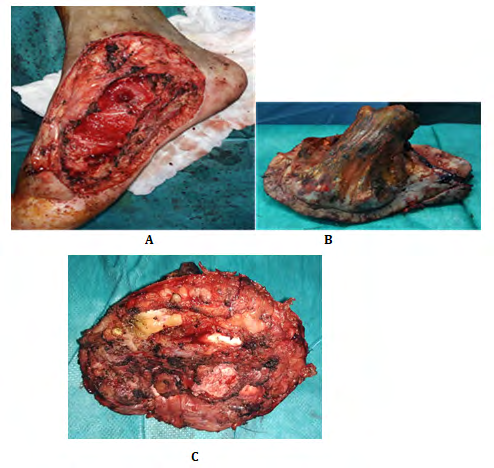
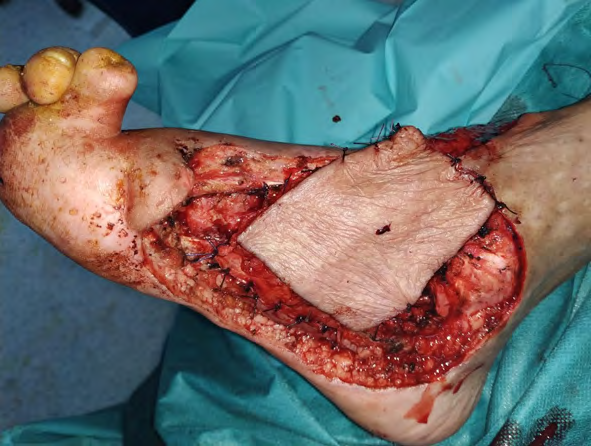
This is a 25-year-old patient, a chronic smoker, victim of a work accident whose mechanism is a crushing of the inner face of the left ankle and heel by a heavy machine, causing him to suffer an open fracture (opening of the tibio-astragal joint), loss of bone substance of the medial malleolus and talus, total destruction of the medial lateral ligament and medial retinaculum) with a decaying wound opposite 10 cm of major axis, exposing the posterior tibial pedicle and medial plantar pedicle (posterior tibial artery severed and repaired) without downstream vascular-nervous disorder. The patient received good emergency surgical trimming under shaving anaesthesia (Figure 5) and immediate coverage with a lateral supra-malleolar flap by the Valenti technique (Figure 6). The skin between the donor and recipient areas was incised and peeled off on the banks to provide a non-compressive passage for the pedicle of the flap. The donor area was grafted secondarily. The evolution was complicated by a nosocomial infection and partial necrosis of the distal half, managed by joint trimming and lavage, antibiotic therapy directed according to the antibiogram, directed wound healing, and thin skin grafting (taken from the inner side of the homolateral thigh) (Figure 7). At 5 months, the functional result is very good: resumption of walking, good mobility of the ankle with symmetrical plantar tenderness on the opposite side. However, the aesthetic result remains average: scarring from the incision and skin grafting, cutaneous depression of the lower half of the loss of substance, sequelae of necrosis, to be managed later by lipofilling (Figure 8).


A B

C


D E Figure 6: A. External supramalleolar flap drawn on the lateral aspect of the leg using the Valenti technique. B and C. removal of the fascio cutaneous flap. D. suture of the donor area to be grafted secondarily. E. Positioning of the flap to cover the joint and exposed pedicle.

A B Figure 7: A and B: partial necrosis of the distal half of the flap managed by directed wound healing and thin skin grafting.

A B Figure 8: A and B Results at 5 months postoperatively.
Discussion
Covering the loss of substance from the ankle poses particularly acute problems, especially when there is an associated osteoarticular lesion, which is the most common case [3, 4]. This difficulty has led to major innovations in reconstructive surgery. One of the useful methods, the one used in our patients, is the lateral supramalleolar flap. Indeed, the lateral supramalleolar flap described by Masquelet, et al. is a wide fasciocutaneous flap (15x9 cm in adults) in true vascular islet, whose skin paddle is fed by the terminal branches coming from the perforating branch of the fibular artery (ramus perforans). It has been shown that this perforating branch is constant, always emerges 5 cm above the lateral malleolus in the tibio-fibular sinus, and gives two or three ascending skin branches (8 cm long). These branches perforate the fascia and form a vascular system in the lateral aspect of the leg. Its distal pivot point, around the axis of the ramus perforans, allows great local possibilities of coverage [1], but it remains difficult to dissect, requiring opening of the interosseous membrane and clearance of the ramus with risks of injury to the latter. Valenti modified his harvesting technique by positioning the skin paddle proximally, to increase the arc of rotation, stopping the dissection 2 cm more proximal to the origin of the artery, which is neither located nor sectioned for greater safety [5] (offset of the pivot point by 2 cm more proximal), and raising it like a fascio- cutaneous flap with a distal pedicle. This makes harvesting much easier and just as reliable. Several other types of flaps were used [6, 7] to cover the loss of substance from the distal half of the leg and ankle:- The peroneal flap [8], the anterior tibial flap [9] and the posterior tibial flap [10] are reliable flaps. However, the need to sacrifice an important vascular axis of the leg is a potentially serious disadvantage especially in patients with a particular terrain, such as diabetic patients or in the context of associated vascular trauma.
The posterior fascio-cutaneous flaps : are vascularized by perforating pedicles located on either side of the Achilles tendon allowing the lifting of a fascio-cutaneous flap that can extend upwards to the base of the popliteal fossa [4] and the sural neuro-cutaneous flap with distal pedicle (whose aponeurotic pedicle dissection is centered on the medial sural cutaneous nerve), a variant of the latter, are easy and reliable flaps but with a limited arc of rotation. In our second patient, the arc of rotation of the posterior fasciocutaneous flaps did not allow coverage of the PDS, the size of the PDS was too large for a sural neuro-cutaneous flap.
Free cutaneous flaps: placed for the first time on the distal third Daniel 1973, O’brien 1973, making it possible to treat almost all cases. However, the difficulty of the technique, the need for secondary procedures and the risks of vascular failure constitute considerable obstacles to their use [5].
Thus, the lateral supramalleolar flap according to Valenti’s technique remains a good alternative for the coverage of these substance losses. Nevertheless, this flap is not without drawbacks [11, 12, 13, 14].
The aesthetic after-effects of the donor area on the anterior aspect of the leg are very visible. In order to reduce them, Lee, et al. [11] proposed the creation of a lateral fasciofatty supramalleolar flap, preserving the skin of the donor area, and lifting a thin, large flap.
Venous congestion: can be a source of partial necrosis, as in all distal pedicle flaps. To reduce this risk, Uysal, et al. [15] leave the external pedicle and do not pass it under a subcutaneous tunnel. Despite this precaution, the distal half of the flap was necrotic in our second case, we believe that there is some venous congestion, aggravated by infection. A painful neuroma of the superficial fibular nerve that can be prevented by burying the nerve in the muscle masses of the leg.
Conclusion
The external supra-malleolar flap, as modified by Valenti, is a simple, reliable and reproducible alternative, not sacrificing a main vascular axis of the leg with an arc of rotation allowing the coverage of the ankle and distal part of the leg substance losses.
References
-
Masquelet A C, Beveridge J, Romana C, Gerber C (1998) The lateral Supramalleolar flap. Plast. Reconstr. Surg 81(1): 74-81.
-
Valenti P, Masquelet AC, Romana C, Nordin JY (1991) Technical refinement of the lateral supramalleolar flap. Br J Plast Surg 44(6: 459-462.
-
Lai CS, Lin SD, Yang CC, Chou CK (1991) Adi- pofascial turn-over flap for reconstruction of the dorsum of the foot. Br J Plast Surg 44: 170-174.
-
Revol M, Binder JP, Danino A, May P, Servant JM (2012) Manuel de chirurgie plastique, reconstructrice et esthétique. 2nd (Edn.), révisée et augmentée. Sauramps medical.
-
Gibstein LA, Abramson DL, Sampson CE, Pribaz JJ (1996) Musculofascial flaps based on the dorsalis pedis vascular pedicle for coverage of the foot and ankle. Ann Plast Surg 37(2): 152-157.
-
Mark FP, Peter JC, Paul AW, Salvatore L (2002) Reverse sural artery flap: Caveats for success. Ann Plast Surg 48(5): 496-504.
-
Jeung SF, Wei FC (1997) Distally based sural island flap for foot and ankle reconstruction. Plast Reconstr Surg 99(3): 744-750.
-
Yoshimura M, Imura S, Shimamura K, Yamauchi S, Nomura S (1984) Peroneal flap for reconstruction in the extremity: Preliminary report. Plast Reconstr Surg 74(3): 402-409.
-
Wee JT (1986) Reconstruction of the lower leg and foot with the reverse-pedicled anterior tibial flap: Preliminary report of a new fasciocutaneous flap. Br J Plast Surg 39(3): 327-337.
-
Hong G, Steffens K, Wang FB (1989) Reconstruction of the lower leg and foot with the reverse pedicled posterior tibial fasciocutaneous flap. Br J Plast Surg 42(5): 512- 516.
-
Lee YH, Rah SK, Choi SJ, Chung MS, Baek GH (2004) Distally based lateral Supramalleolar adipofascial flap for reconstruction of the dorsum of the foot and ankle. Plast Reconstr Surg 114I(6): 1478-1485.
-
Demori E, Foroglou P, Dionyssious D, Antoniou A, Kakas P, et al. (2006) our experience with the lateral supramalleolar island flap for reconstruction of the distal leg and foot: Review of 20 cases. Scand J Plast Recontr Hand Surg 40(2): 106-110.
-
Hakan A, Cenk S, Murat O (2007) Extended lateral supramalleolar flap for very distal foot coverage: A case with arteriovenous malformation. J Foot Ankle Surg 46(4): 310-313.
-
Voche P, Mewrle M, Stussi JD (2005) the lateral supramalleolar flap: Experience with 41 flaps. Ann Plast Surg 54(1): 49-54.
-
Uysal AC, Alagoz MS, Sensoz O (2006) Distal based lateral supramalleolar adipofascial flap. Plast Reconstr Surg 117(2): 685-686.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review