Evaluation of Carbon Dioxide Angiography in Management of Critical Lower Limb Ischemia with Infrapopliteal Arterial Disease
The aim of the study is to elaborate on the understanding of the application of the CO2 angiography in obtaining quality imaging of infrapopliteal diseased arteries by digital subtraction CO2 angiography, and angioplasty using the automated Angiodroid CO2 injector® (primary outcome). This is a retrospective observational non-randomized study that included 23 patients of critical LL ischemia having infrapopliteal disease alone or combined with the femoropopliteal disease along with typical renal impairment. Carbon dioxide digital subtraction angiography (CO2 DSA) was used for all the patients and the outcomes were subjected to the comparison by iodinated contrast by an operator. The study included 17 female and 6 male subjects. The age group of the patient was between 48 years and 78 years. The mean age was 61.8 ± 11.1 years. The quality of the images obtained from the CO2 DSA method adopted was categorized as: good images (9) 39%, Accepted (8) 34%, and bad (6) 26% images. No complication from CO2 injection occured for the patients, while leg pain was recorded in 4 patients during the CO2 injection (17.3%). The trial outcome elaborated and supported the safety of using CO2 angiography in the diagnosis and management of critical LL ischemia with infrapopliteal disease.
Introduction
Peripheral arterial disease (PAD) or Peripheral vascular disease is predominant in the global population presently. Recent analysis suggests that more than 200 million people are having PAD [1]. Specific diagnosis of PAD especially the infrapopliteal disease remains the key for management [2]. Endovascular therapy with iodinated contrast is considered the main stay but sometimes it is not suitable for renal impairment patients [3]. Carbon dioxide angiography is considered then as an alternative contrast for endovascular diagnosis and management of critical limb ischemia especially those who are diabetics and have renal impairment [4, 5]. The incidence of contrast induce nephropathy in peripheral arterial disease patient is 3% [6]. Prevention of this problem included decreasing the amount of contrast used, also CO2 as a contrast can be used as it is neither nephrotoxic nor allergic [7, 8]. The use of carbon dioxide is useful however the quality of image is doubtful [9].
Methods
Patient Selection
This is a retrospective observational non-randomized study that included 23 patients having Critical Limb Ischemia (CLI). All the selected patients were having renal impairment either accompanied with infrapopliteal disease alone or in combination with the femoropopliteal disease.
The recruitment of the patients was done at the Outpatient Clinic of the Vascular Surgery Unit in Kasr alainy University Hospital. The patient recruitment was conducted for two years (June 2017-May 2019). We confirm the approval of the Medical Committee of Vascular Surgery Department that this work is ethically accepted and all patients have signed and approved to be in the study.
Inclusion and Exclusion Criteria
The inclusion criteria of the patients included Critical LL ischemia with only infrapopliteal disease or infrapopliteal disease along with femoropopliteal disease clinically established. The presence of Diabetic nephropathy was another important inclusion criteria decided for this study. Similarly, patients having certain characteristics were excluded from the study such as patients who were having end-stage renal disease and the patients having a normal renal function and were not diabetic.
Pre-procedure data recording
All the selected patients were investigated strictly considering the inclusion and exclusion criteria mentioned and records on the clinical and medical history, outcome of the clinical examination and routine laboratory investigations were collected systematically. Additionally, information on their duplex scan of both the lower limbs from the Aorto- iliac position to both the pedals was carefully investigated and recorded.
Procedure Preparation
All patients were done in the Angiosuite. In this process, Carbon Dioxide Angiography (CDA) was used to fulfill the purpose.
Angiosuite Set Up
The angiography was done by Philips AlluraXper® FD 20/722028164 system that is compatible with the automated Angiodroid CO2 injector® that had important required features such as digital subtraction angiography (DSA), CO2 software, frame rate at least 4-6 fps, road mapping, CO2 stacking, contrast enhancement, pixel shift, and inversion scale. Iodinated contrast (IC) was used with variable amounts to confirm and compare the CO2 DSA.
Pre-Procedure Preparation
In this process, clopidogrel 75 mg (4 tablets = 300 mg) was used as the loading dose, intravenous hydration (0.5-1 ml/kg/hr., normal saline) was applied and continued after the procedure for 12 hours. The individual patient was instructed to lie in the supine position with a 30-degree inclination in a Trendelenburg position as a safety measure. The patients were having proper immobilization for accurate x-ray and were also having compatible external bandage.
Procedure
During the procedure, local anesthesia was used at the puncture site when ipsilateral common femoral artery access was done with 6FG and 10 ml of CO2 was injected to replace the air in the tubes and to prevent the formation of the air bubbles. The volume of CO2 injection (10-100 ml) applied per injection was dependent on the target site and the catheter size. In the present study, the volume injected was 30 ml for infrapopliteal angiography (selective 5 FG catheter 60 cm long), and 20 ml was injected through femoral sheath when the patient was undergoing popliteal angiography. While using a short catheter, the pressure setup was 200 (150-250) mm Hg, and 400 (350-450) mm Hg was set when micro catheters or long introducers were used. Usually, the pressure was set to 30 mmHg above the patient’s systolic blood pressure in case of the use of short catheters. Interval of 1-2 min was allowed between the repeated CDA procedures. For each case, CO2 stacking, contrast enhancement, pixel shift after processing, and inversion scaling were done carefully. To have high-resolution images, CO2 DSA was conducted for the infra-popliteal area. Unlike conventional DSA with IC, immediate evaluation of the images was avoided as many images (6 frames/sec) were integrated [9]. Analyses were done frame by frame along with capturing the better images through using the subtraction button [10]. This setup allowed better visualization of infrapopliteal angiography images as well as caused reduced pain to the patient. During this process, the amount of CO2 injected, the pressure of CO2 used, and the amount of iodine confirmatory contrast obtained was recorded. The quality of the imaging obtained by the CO2 distal subtraction angiography was compared with the iodine contrast digital subtraction angiography by an operator using the subjective method.
Quality analysis of CO2 DSA Angiography
The images obtained from CO2 DSA were compared with the iodinated contrast iopromide by an independent operator using (Ultra vist®) at 12 points where each tibial had 4 zones. Each zone was scored as “1” if found good, or “0” if found not acceptable. Later, the sum was calculated. The 4 zones considered were: I: From just above the malleoli till the foot II: Above malleoli for the distal 1/3 of the leg III: Second (2nd) 1/3 of the leg IV: Proximal first 1/3 of the leg from below neck of the fibula. The obtained quality of the CO2 DSA imaging was further divided into 3 categories (Good, accepted, bad) according to the Philips proprietary post-processing software as defined in the following section.
- Good: Adequate image quality for appropriate diagnosis that can allow proceeding with the intervention [10, 11, 12].
- Accepted: Adequate image quality for diagnosis, but needed confirmatory Iodinated Contrast (IC) to proceed with the intervention [7, 8, 9].
- Bad: Inadequate image quality for proper diagnosis and intervention. (IC) must be used for these imaging (6 and below 6).
Data availability
The authors confirm that the data supporting the findings of this study are available within the article.
Results
Population, comorbidities, CLI
Twenty three (23) patients were considered in this study with CLI infrapopliteal disease & renal impairment. These patients underwent angioplasty using CO2 as a contrast. The study included 17 females and 6 males. The observed age group was 48-78 years. The mean age observed was 61.8 ± 11.1 years.
The risk factors associated with considered patients were: Diabetes mellitus (n=21)91%, Hypertension (n=21) 91%, Ischemic Heart Disease (n=9) 39%, Renal complications (n=19) 82% and Cerebrovascular stroke (n=5) 21%.
The Rutherford classification of the critical limb ischemia was as following: Class V: n=16 (70%), Class VI: n=7 (30%). The distribution of the lesions recorded was as following: the superficial femoral artery (SFA) with infrapopliteal disease was in 17 (73.9%) patients, and Infrapopliteal disease alone was present in 6 (26.1%) patients.
Imaging Quality Analysis
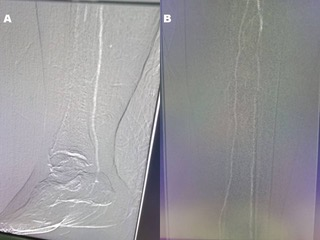
CO2 angiography was used in 21 cases and 2 cases were exempted due to allergy to the iodine. The mean pressure for injection was 170 ± 18 mm Hg, and the mean total volume for each case was 220 ± 48 ml. No complication from CO2 injection occurred in these patients, while leg pain was recorded in 4 cases during CO2 injection (17.3%). During the process, we observed that the diagnostic value of CO2 angiography in the infrapopliteal arteries was least consistent in the distal segments due to the motion artefact caused by leg pain during injection. However, selective catheterization, leg elevation, patient cooperation, analgesia, and local administration of vasodilators, may be helpful (Figures 1-3).


Renal Function Follow-Up
Contrast-Induced Nephropathy (CIN) is considered by >25% increase or > 0.5 mg/dL (44.2 µmol/L) in serum creatinine level within the 3 days of intravascular contrast administration. However, the absence of an alternative cause remains another major criterion. The amount of confirmatory diluted iodinated contrast ranged from 0-35 ml with an average of 15.77 ml. Therefore, the actual amount was 7.88 ml. The purpose and application of IC were presented as confirmatory (n=17), ineffective (n=6), and not used (n=2) for the patients in this study. There were a total of 3 cases of Contrast-Induced nephropathy (CIN), one patient was having dialysis and died after 1 month due to septic shock after BKA. The others recovered to their baseline creatinine level as recorded during the preoperative stage. There were 2 cases of mortality in the whole study (8.6%).
Pain Perception during CO2 Angiography
A total of 4 patients experienced various degrees of transit pain (mild to moderate) (1-6 in scale of 10) during automated CO2 injection for angiography and angioplasty. No additional pain killers were required.
Discussion
Proper diagnosis and accurate invasive procedure determine the success rate of angioplasty, especially, for the patients having severe complications such as CLI. CO2 as contrast has been used for a long time in endovascular therapy [4]. Specifically, in patients who have renal impairment, such procedures become essential, however, often such patients are expected to have Contrast-Induced nephropathy (CIN) or known to have some kind of contrast-induced allergy [8]. Technically, for better imaging and diagnosis requirement, endovascular therapy requires the use of iodinated contrast. However, this increases the incidence of Contrast-Induced nephropathy (CIN), especially in the diabetic patient [11, 12].
The use of CO2 as a contrast medium is still noisy to the physicians, especially, if the target vessels are infrapopliteal arteries which require higher precision and accuracy for diagnosis and treatment. Motion or artifact derived comparatively poor quality of images derived from CDA remains a major challenge in this issue. The experience and expertise of the radiologist play a pivotal role in interpreting the images in such circumstances. In the present study, such a problem was countered by using 6 frames/sec imaging with better subtraction, pixel shifting, and image stacking.
The use of high-quality imaging machine with high resolution of more the 1024 X 1024 pixels analyzed with the sophisticated software in the imaging machine, allowed us to have high-quality CO2 imaging. Further, due to the integration of multiple images and frame-wise analysis, the outcomes of the observations were accurate. A similar report is done by Cho as well [9]. The state-of-the-art machinery used in this analysis also supported tremendously in the reduction of the artifacts and false-positive outcomes. Another important technical problem of air contamination was managed by using the air filter and injecting 10 ml of CO2 in this study. The other issue is the pain triggered during the CDA process due to the gas explosion caused by compressed gas was managed through clearing the catheter and system by flushing them with 10 ml of CO2. However, the existing literature suggested the application of only 3-5 ml of CO2 to flush the catheter [9].
Moreover, the automated process injected in small volumes for the automatically targeted preset pressure yielded better imaging quality and lesser pain to the patient.
The volume used was only 20 ml of CO2 with 30 mmHg pressure exceeding the systolic pressure of the patients. Therefore, customization was done for each of the patients for a better outcome. The followed intervals of 2 min also supported the outcomes. Besides, the imaging of the infrapopliteal arteries using a catheter placed in the lower popliteal allowed better visualization of infrapopliteal arteries and also provided better visualization of the whole popliteal artery due to the reflux criteria. Such criteria were not present in other iodinated contrast as mentioned by Giordano, et al. [10] Other reports suggested the use of the old mechanical injector that remained comparatively complicated to handle and were having an effect on the outcome as well [13].
However, we have adopted the selective angiography process similar to the study by Cheng-Feng, et al. unlike the external bandage, patient alignment at the 30 degrees Trendelenburg position. Interestingly, in their experiments 3 patients were unable to complete the procedure due to the intense leg pain, however, they have mentioned that reduction of the CO2 volume from 80-100 ml to 40-60 ml yielded some benefits and relief in the leg pains of the patients. Similarly, we have also used a reduced volume that helped us made the pain of the patients bearable. Another study conducted by Fujihara, et al. excluded the patient having infrapopliteal disease, but the study reported the benefit of using the CO2 angiography in infrainguinal disease [8]. Our outcomes were comparatively better with such complicated angioplasty. However, the present study is having certain limitations. The study is a single armed registry and was conducted on only a small number of patients who are known to have an allergy to iodinated contrast or who have renal impairment of Rutherford V and VI-grade. Also, the evaluation of images was done by a single operator, hence, manual expertise was considered. On the contrary, the present study followed almost a standard process for all the patients, thus, ensuring the high quality of the angiographic images and the diagnosis outcomes.
Conclusion
The trial elaborated on the safety of using CO2 angiography in the diagnosis and management of CLI with infrapopliteal disease which remains a challenge in medicine even now. The procedure causes some leg pain and requires caution in the adjustment of the administered CO2 volume and pressure. In the future, with the precise tuning of the volume and pressure, the outcome may become much favorable to the patient and the radiologist. Moreover, the CO2 may replace other iodinated contrast as it is cheaper than the iodinated contrast. Good quality images, nontoxic property, the repetitive possibility of application, absence of renal complication, higher solubility, injection through small diameter catheters, can make this process a game-changer in this specific type of diagnosis and procedure. More future experiments can also allow standardizing the application of CO2 angiography and helping in numerous patient CLI treatment, management, and recovery.
References
-
Shu J, Santulli G (2018) Update on peripheral artery disease: Epidemiology and evidence-based facts. Atherosclerosis 275: 379-81.
-
Wright LB, Matchett WJ, Cruz CP, James CA, Culp WC, et al. (2004) Popliteal artery disease: Diagnosis and treatment. Radiographics 24(2): 467-479.
-
Rana MA, Gloviczki P (2012) Endovascular Interventions for Infrapopliteal Arterial Disease: An Update. Semin Vasc Surg 25(1): 29-34.
-
Back MR, Caridi JG, Hawkins IF, Seeger JM (1998) Angiography with carbon dioxide (CO2). Surg Clin North Am 78(4): 575-591.
-
Abdelbary MH, Mohamed AE, Abdel Hamid A (2018) Accuracy and safety of CO2 digital subtraction angiography during endovascular treatment of symptomatic peripheral artery occlusive disease. A prospective study on Egyptian patients. Egypt J Radiol Nucl Med 49(1): 76-84.
-
Grossman PM, Ali SS, Aronow HD, Boros M, Nypaver TJ, et al. (2017) Contrast-induced nephropathy in patients undergoing endovascular peripheral vascular intervention: Incidence, risk factors, and outcomes as observed in the Blue Cross Blue Shield of Michigan Cardiovascular Consortium. J Interv Cardiol 30(3): 274- 280.
-
Gupta RK, Bang TJ (2010) Prevention of contrast-induced nephropathy (CIN) in interventional radiology practice. Semin Intervent Radiol 27(4): 348-359.
-
Fujihara M, Kawasaki D, Shintani Y, Fukunaga M, Nakama T, et al. (2015) Endovascular therapy by CO2 angiography to prevent contrast-induced nephropathy in patients with chronic kidney disease: A prospective multicenter trial of CO2 angiography registry. Catheter Cardiovasc Interv 85(5): 870-877.
-
Cho KJ (2015) Carbon Dioxide Angiography: Scientific Principles and Practice. Vasc Spec Int 31(3): 67-80.
-
Giordano A, Messina S, Polimeno M, Corcione N, Ferraro P, et al. (2015) Peripheral diagnostic and interventional procedures using an automated injection system for carbon dioxide (CO2): case series and learning curve. Heart Lung Vessels 7(1): 18-26.
-
Azzalini L, Spagnoli V, Ly HQ (2016) Contrast-Induced Nephropathy: From Pathophysiology to Preventive Strategies. Can J Cardiol 32(2): 247-255.
-
Toprak O (2007) Risk markers for contrast- induced nephropathy. Am J Med Sci 334 (4): 283-290.
-
Ho CF, Chern MS, Wu MH, Wu HM, Lin WC, et al. (2003) Carbon Dioxede Angiography in Lower Limbs: A Prospective Comparative Study with Selective Iodinated Contrast Angiography. Kaohsiung J Med Sci 19(12): 599- 607.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review