Role of Balloon Angioplasty in the Salvage of Impending Arteriovenous Fistula Failure for Patients Undergoing Hemodialysis
As per the guidelines issued by the Kidney disease outcome quality initiative, autologous arteriovenous fistula (AVF) is the most appropriate and best prescribed therapeutic strategy for hemodialysis procedure. Early detection of stenosed AVF increases the chances of a successful angioplasty by enhancing the patency rate for a longer period. This prospective observational study was conducted, with 87 evaluable hemodialysis patients, from September 2016 to January 2019. All patients were consented to perform endovascular intervention. The follow up was conducted at 1, 3, 6, 12 months. The mean patient age was 50.24 + 13.38.Hypertension (70.1%) and diabetes (28.7%) were noted comorbidities. About 78.1% of patients had brachiocephalic AVF, and 97.7% of lesions were stenotic juxta anastomotic. Also, 95.4% of patients had undergone hemodialysis through trans radial access. The primary and secondary patency rates at 12 months were 91.4% and 100%, respectively. Complications, including hematoma and surgical thrombectomy were noticed in 4.6% of patients. Balloon angioplasty procedure, either transradial or transbrachial, proved to be effective in all dysfunctioning AVF patients with > 30% stenosis. This can salvage the impending failure of AVF in hemodialysis patients with high primary and secondary patency rates over a year's time.
Introduction
End-stage renal disease (ESRD) is one of the most commonly reported chronic renal disorders showing an escalatory trend with an increase in the number of cases globally [1]. ESRD is clinically classified as the fifth stage of chronic renal disease, and hemodialysis is the best- prescribed treatment for many reasons. Egypt reports the most number of ESRD cases every year [2]. Hemodialysis is generally carried out either by autologous AVF and a synthetic AVF graft or by central dual catheters [3]. The therapeutic management of all the treated patients involves routine hemodialysis procedures based on autologous AVF graft in the upper limb [4]. Autologous AVF is regarded as the most effective and long-standing medical intervention procedure for ESRD and signifies the improved quality of life for treated patients. As per the guidelines issued by the Kidney disease outcome quality initiative (KDOQI), autologous AVF is the most appropriate and better procedure for hemodialysis procedure [5]. Further, regular clinical follow-up and ultrasonography examination of these patients is highly recommended for early detection of AVF stenosis before or to prevent the occurrence of total occlusion [6]. Early detection of stenosed AVF significantly improves the possibility of a successful angioplasty by enhancing the patency rate for a longer time period [7]. Management of stenosed fistulae is carried out either by endovascular (angioplasty) or by open surgery, and angioplasty was employed in the current study [8]. The present study aimed to decipher the role of balloon angioplasty in salvage of impending AVF failure for patients undergoing hemodialysis.
Methods
Investigation Plan
This prospective observational study was conducted at the vascular surgery outpatient clinic in Cairo university hospital, Egypt, with a retrospectively recorded data of 87 patients referred from the Hemodialysis unit from September 2016 to January 2019.
Selection of Study Subjects
The potential patients were identified and screened as per the clinical research team’s inclusion and exclusion criteria. Inclusion criteria: The following observations were noted in study subjects during clinical examination: Attenuated thrill, bounding pulsations, discontinuation of the fistula (interruption of the venous side of the fistula), redirection of the fistula (e.g., stenosed part of venous side of radio cephalic fistula may redirect the fistula towards the basilic vein), upper limb swelling (either proximal or distal to fistula or both), developing of collaterals over the chest wall in cases of associated central stenosis, history of difficult cannulation of the fistula for dialysis, suction on dialysis, decrease flow rate less than 300 ml/min (imminent thrombosis) [9], decrease total flow rate less than 500 ml/ sec (access dysfunction) [9], as measured by duplex in the regular visit/follow up checkup. Exclusion criteria: Absent pulsation and thrill on the fistula, long-standing occlusion, primary AVF, and dialysis were not yet prescribed for patients.
The study subjects/legally authorized representatives signed a voluntary informed consent form to facilitate the collection of necessary data from the hospital records. The data collected was compiled centrally, cleaned, and analyzed for outcome clinical report preparation.
Patient Treatment Procedures And Measurements
The following data were collected and analyzed for all study subjects enrolled in this study: demographic details - name, age, gender, contact no, location, diagnosis/ medical history, comorbidity associated with hypertension, diabetes mellitus, type of fistula - radio cephalic (left, right), brachiocephalic (left, right), brachiobasilic AVF with super focalization (left, right), type of lesion - duplex Juxta anastomotic stenosis, duplex venous occlusion, duplex central lesion, cephalic arch lesion, type of access-trans radial, trans venous, trans brachial and combination. Crossing of the lesion within 5 minutes, external compression needed, and inflation single were examined in patients. Distribution of study population according to complications was noted in the following variables: hematoma, pulmonary embolism, steal, thrombotic ischemia, hybrid thrombectomy, hybrid aneurysmorraphy, disappearance of artery in radial access, and nil residual outflow obstruction was examined.
Primary patency (12 months) and secondary patency (12 months) was determined as per the following set definitions and measures of clinical success and represented as Kaplen Meier curves of patency. Definition of primary patency: The durability of the AVF after angioplasty of the impending failure of AVF within a year. Definition of secondary patency: It is the cumulative durability of AVF after re-angioplasty within the year. The measure of clinical success is defined as 3 successful consecutive hemodialysis sessions of the salvaged AVF.
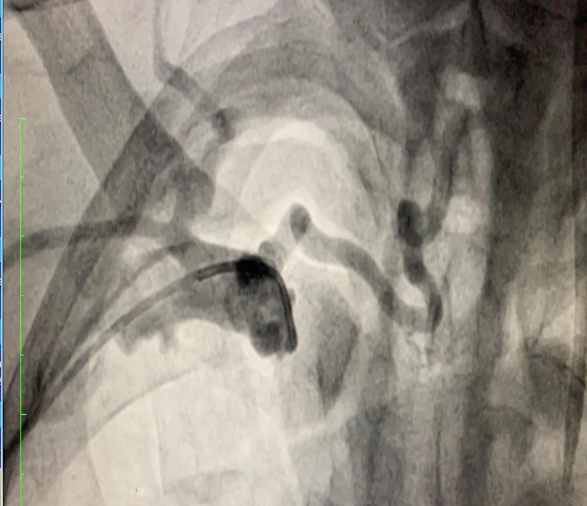
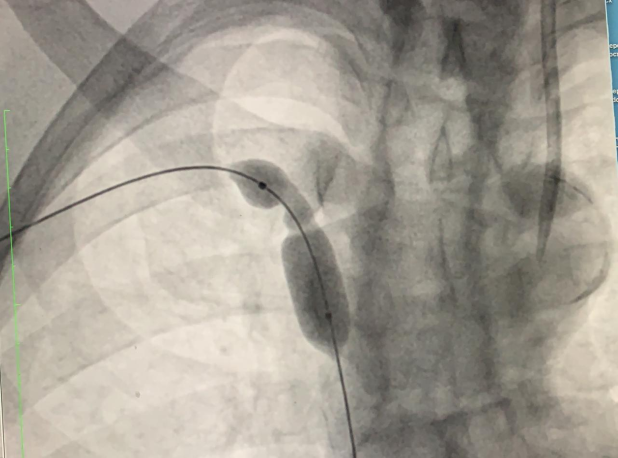
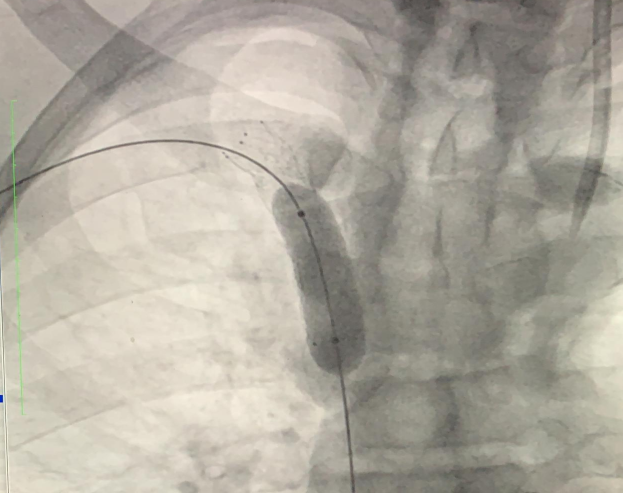
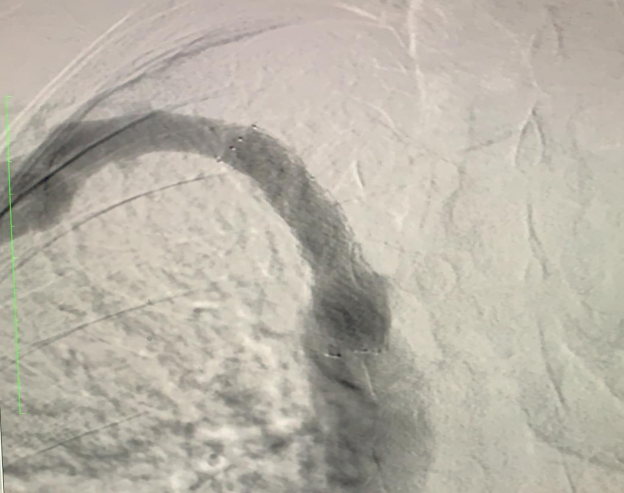
All patients were subjected to clinical examination; duplex was carried out to confirm the diagnosis. Patients were consented before performing endovascular intervention and angioplasty. All procedures were performed by Philips Allura X per FD 20/722028164, Netherlands, and GE Elite OEC 9700 (General Electric, USA). The targeted upper limb was disinfected and draped. The radial artery or the brachial artery was targeted according to the type of fistula - radio cephalic, brachiocephalic or brachiobasilic with superficialization. Local infiltration anesthesia with lidocaine (2%) 2-3 ml was infiltrated in the skin, over the artery before puncture by 20 G needle. Seldinger technique was utilized to insert standard 11 cm 6 FG sheath into the artery, and later wires and introducers were withdrawn, followed by little withdrawal of the sheath until the opening of the sheath was just distal to the anastomosis in case of trans radial access in radio cephalic in AVF, or distal to brachial anastomosis in brachiocephalic, or brachiobasilic AVF. In some cases, 7 FG was utilized to accommodate larger balloons for central lesions. The access was either trans arterial alone or combined arterial and antegrade venous. Heparin 5000 IU was administered inside the sheath, and then an angiogram was carried out to show the arteriogram, AV anastomosis, and the steno tic segment on the vein side. Later, the passage of standard Terumo wire 0.035 J tip through the stenotic lesion and the passage of vertebral catheter 5 FG was carried out for identification of more proximal lesions. Any stenosis >30% was dilated repeatedly till the maximum pressure of the balloon was attained. Further, angiography was performed to ensure that there was no significant residual stenosis > 30%. Later, the catheter was withdrawn, and a balloon catheter was inserted to pass through the stenotic lesion and inflated until the lesion was dilated. Now, the balloon catheter was withdrawn, and a completion angiogram was performed to evaluate any residual lesion or thrombi to ensure free flow up to the central veins. Later, the sheath was withdrawn, followed by compression bandage. A
few cases were scheduled for another set to be performed by general anesthesia because of pain management for patients with central lesions (Figures 1-6).


Regular follow-up of patients was carried out monthly with the attendance of a vascular surgeon, nephrologist, radiologist, the nursing staff of the dialysis unit, to have a multidisciplinary approach to direct the patient to either regular follow up, prescribe endovascular management, or the surgical AVF reconstruction. The follow up was conducted at 1, 3, 6, 12 month time period accompanied by clinical examination and a duplex scan.
Statistical Analysis
The recorded study data was compiled and recorded in Microsoft Excel 2010 program and later exported to the data editor page of statistical software, SPSS version 20.0 (Armonk, NY, USA: IBM Corp.). Frequency distribution was calculated for qualitative data. Kaplan Meier survival analysis was conducted for the determination of primary and secondary patency rates.
Results
Demographic details of study subjects
The study was conducted in 87 patients; the majority of study participants were males (male, n=61; female, n=26). The mean age of the study population was 50.24 + 13.38 in the age range of 24-76 years (Table 1). Regarding the comorbidities, 70.1% of patients were hypertensive, and 28.7% of patients had diabetes.
| Number | Percentage | |
|---|---|---|
| Sex | ||
| Male | 61 | 70.1 |
| Female | 26 | 29.9 |
| Diabetes Mellitus | 25 | 28.7 |
| Hypertension | 61 | 70.1 |
| Radiocephalic | ||
| Left | 9 | 10.3 |
| Right | 8 | 9.2 |
| Brachiocephalic | ||
| Left | 45 | 51.7 |
| Right | 23 | 26.4 |
| Brachiobasilic AVF with superficialization | ||
| Left | 2 | 2.3 |
| Right | 0 | 0 |
| Duplex Juxtaanastmotic stenosis | 85 | 97.7 |
| Duplex Venous occlusion | 86 | 98.9 |
| Duplex Central Lesion | 6 | 6.9 |
| Cephalic Arch lesion | 5 | 5.7 |
| Access | ||
| Transradial | 83 | 954 |
| Transvenous | 7 | 8 |
| Transbrachial | 2 | 2.3 |
| Combined | 8 | 9.2 |
| Crossing of the lesion within 5 minutes | 74 | 85.1 |
| External compression needed | 49 | 56.3 |
| Inflation single | 0 | 0 |
| Mean Age | 50.24 + 13.38 |
Table 1: Patient demographics.
The total prevalence of radiocephalic AVF (9 left, 8 right), brachiocephalic (45 left, 23 right) and brachiobasilic AVF with superficialization (2 left, 0 right) were 19.5%, 78.1%, and 2.3%, respectively. Most of the lesions (97.7%) were steno tic juxta anastomotic, only 5.7% were in the cephalic arch, and 6.9% were central (all were associated with juxta anastomotic).
Most of the patients were performed through transradial access (95.4%) alone, 8% through transvenous access, 2.3% were performed through transbrachial access, and 9.2% were performed through combined (transvenous and transradial) access (Table 1).
The inflow problem was not noticed in any of the cases. Post dilatation, the radial artery’s disappearance was found during an angiogram in 97.7% of patients (n=85) (Table 2). Most patients (n=86) were clinically with good thrill, and all study subjects had adequate 3 consecutive dialysis procedures.
| Number | Percentage | |
|---|---|---|
| Hematoma | 4 | 4.6 |
| Pulmonary embolism | 0 | 0 |
| Steal | 0 | 0 |
| Thrombotic Ischemia | 0 | 0 |
| Hybrid Thrombectomy | 4 | 4.6 |
| Hybrid Aneurysmorraphy | 0 | 0 |
| Disappearance of artery in radial access | 85 | 97.7 |
| No residual outflow obstruction | 0 | 0 |
Table 2: Distribution of study population according to complications.
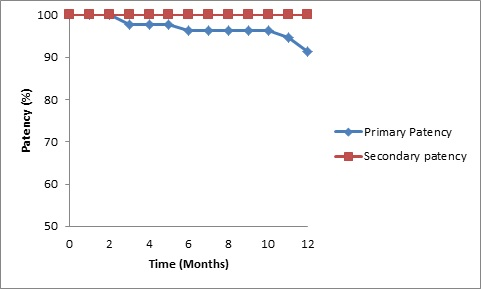
During 3-month follow-up, one case of reangiography was reported, and balloon angioplasty was carried out. Mortality was observed in 2 patients, and 3 patients were converted to open repair as reversed saphenous interposition used as a conduit, not for puncture. During the 6-month follow-up, nil cases of reangiography were noted. However, one patient had venous hypertension (central stent occlusion). Mortality was observed in1 patient, and none of the patients were converted to open repair. During the 9-month follow-up, no significant observation was noted in the study subjects. During 1-year follow-up, one patient had of reangiography, one patient reported venous hypertension, and mortality was observed in 1 patient. The primary patency rate at 12 months observed was 91.4%, and the secondary patency rate at 12 months observed was 100% (Figure 7).
Major of the lesions (85.1%) needed less than 5 minutes to cross, and the rest crossed within 30 minutes. External compression was needed in 56.3% of patients. Repeated inflation (2-5 times) was mandatory for all patients, even with different balloon diameters (Table 1).
Distribution of Study Population According to Complications
Regarding the complications, 4.6% of patients developed a hematoma at the stenosis site related to the hemodialysis, cannulation site, and 4.6% cases needed surgical thrombectomy (hybrid) technique caused due to residual thrombus post dilatation angioplasty. There were no recorded pulmonary emboli. The mortality recorded by the end of the year was 4 cases (4.6%). The disappearance of the artery in radial angiography was observed in 97.7% of patients (Table 2).
Discussion
ESRD is the most devastating disease, and most of the patients are on regular hemodialysis, which signifies and represents the quality of life of patients. Continuous AVF functioning is the only hope of every physician & patient. The early medical intervention of stenosed AVF will salvage the fistula, thereby providing more time to perform dialysis for the patient. In the current study, most of the patients were associated with medical comorbidities, including hypertension and diabetics. Sedlacek, et al. reported no significant difference between diabetic and non-diabetic AVF in hemodialysis patients [10]. However, hypertension was always accounted for as a factor responsible for cardiovascular deaths in these patients [11]. As per the latest KDOQI guidelines, it was recommended to treat the stenosed segment associated with AVF [12]. However, most of the patients were concerned about losing their fistula, and the catheter had to be inserted during the dialysis procedure until the fistula was repaired. Therefore, there was a greater need to keep the fistula functioning for hemodialysis. Regular follow-up clinical examination and diagnosis by duplex are necessary for the detection of early failing AVF [13]. In the current study, all the patients were subjected to elective angioplasty with regular, not high-pressure balloons, mostly through a transradial approach that allowed better visualization of the whole fistula; inflow, anastomosis, and outflow up to the central veins. Kritikou et al. evaluated a series of angioplasties in AVF over a year time period and reported primary patency of 91%.
This study’s indication was patients with stenosis more than 50%, in contrast to our study, where we noticed more than 30% stenosis [14]. Chang, et al. reported a comparative study between statin-treated and nonstatin patients with AVF, revealing an 18% risk reduction in patients treated with a statin [15]. Although the antegrade transvenous approach is considered the gold standard access [16], it showed the disadvantage of not accessing the anastomosis, risk of embolization, and risk of occlusion of the fistula occurring due to compression [16]. This study’s mode of access was either transradial, transbrachial, transvenous (antegrade, retrograde), or a combination of both the methods. The significant advantage of utilizing the transradial or transbrachial approach was its ability to diagnose and intervene with inflow, anastomosis, and outflow problems. Few studies have reported against the usage of transbrachial access because of the need to insert 7FG to accommodate large balloons, in cases of associated central vein occlusion. However, in the current study, transbrachial access was carried out by the utilization of 6FG guided by ultrasound, further completion angiography established no further noticeable clinical complication [17]. Further, in the current study, no ischemic complications were noticed in either transradial or transbrachial access. In the present study, the balloon employed in angioplasty was always 4-6 mm in diameter with different lengths, introduced through 6 FG in all angioplasties. This process was repeated multiple times until less than < 30% residual stenosis was noticeable. None of the high-pressure balloons or cutting balloons was utilized in our study due to their non-availability. The primary patency rate of 89.6% and secondary patency rate of 90.8% were noted. Aftab, et al. reported a comparative study on 516 patients with AVF, suboptimal results were observed with the conventional balloon, which was further randomized into 2 groups, high-pressure balloon, and cutting balloon, showed primary patency rate of 39.4%and 66.4%, respectively at 6 months [18].
In the present study, we utilized only conventional (plain) balloons without any drug-coated balloons (DCB) angioplasty. Lucev, et al. performed a comparative study between the angioplasty of conventional balloons and drug- coated balloons in patients with stenosed, failing AVF with respect to the primary patency, secondary patency rate, and primary assisted patency of the target lesion. Observations revealed that no difference in primary assisted patency and secondary patency was noted. However, there was a significant difference between the angioplasty of DCB and the angioplasty of conventional balloons. Hence, in comparison to conventional angioplasty, DCB angioplasty was the most favorable treatment approach noticed during 6 months (90.3 vs. 61.3%), 12 months (77.4 vs. 29%), and 24 months (45.2 vs. 16.1%) follow-up period [19]. In accordance with the above findings, the future prospect of the current study can involve performing DCB angioplasty for the angioplasty of failing AVF. Although this may increase treatment expenses, it has the potential to yield significantly better results.
The complication observed in the current study was hematoma reported in 4 patients not related to the access site. The possible advantage of salvaging the AVF by performing angioplasty provides more time for the fistula’s utilization and avoids usage of central lines. The mortality rate observed in the current study was 4.6%, as earlier studies had shown that ESRD patients on hemodialysis are 30 times more liable to die due to cardiovascular complications in comparison to other patients [11].
Conclusion
Balloon angioplasty procedure, either transradial or transbrachial, proved to be effective in all dysfunctioning AVF patients with > 30% stenosis. This can salvage the impending failure of AVF in a hemodialysis patient with high primary and secondary patency rates over a year’s time period.
References
-
Luyckx VA, Tonelli M, Stanifer JW (2018) The global burden of kidney disease and the sustainable development goals. Bull World Health Organ 96(6): 414- 422.
-
Soliman AR, Fathy A, Roshd D (2012) The Growing Burden of End-Stage Renal Disease in Egypt Ren Fail 34(4): 425-428.
-
Thomas M, Nesbitt C, Ghouri M, Hansrani M (2017) Maintenance of Hemodialysis Vascular Access and Prevention of Access Dysfunction: A Review. Ann Vasc Surg 43: 318-327.
-
Segal M, Qaja E (2020)Types of Arteriovenous Fistulas. Stat Pearls. Stat Pearls Publishing.
-
Inker LA, Astor BC, Fox CH, Isakova T, Lash JP, et al. (2014) KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis 63(3): 713-735.
-
Bjorkman P, Weselius EM, Kokkonen T, Rauta V, Alback A, et al. (2019) Drug-Coated Versus Plain Balloon Angioplasty In Arteriovenous Fistulas: A Randomized, Controlled Study With 1-Year Follow-Up (The Drecorest Ii-Study). Scand J Surg 108(1): 61-66.
-
Falk A (2006) Maintenance and salvage of arteriovenous fistulas. J Vasc Interv Radiol 17(5): 807-813.
-
EBPG on Vascular Access. Nephrology Dialysis Transplantation. Oxford Academic.
-
Zamboli P, Fiorini F, D’Amelio A, Fatuzzo P, Granata A (2014) Color Doppler ultrasound and arteriovenous fistulas for hemodialysis. J Ultrasound 17(4): 253-263.
-
Sedlacek M, Teodorescu V, Falk A, Vassalotti JA, Uribarri J (2001) Hemodialysis access placement with preoperative noninvasive vascular mapping: Comparison between patients with and without diabetes. Am J Kidney Dis 38(3): 560-564.
-
Agarwal R, Lewis RR (2001) Prediction of hypertension in chronic hemodialysis patients. Kidney Int 60(5): 1982-1989.
-
Fistulography - an overview, ScienceDirect Topics.
-
Siddiqui MA, Ashraff S, Santos D, Rush R, Carline T, et al. (2018) Predictive parameters of arteriovenous fistula maturation in patients with end-stage renal disease. Kidney Res Clin Pract 37(3): 277-286.
-
Bountouris I, Kritikou G, Degermetzoglou N, Avgerinos KI (2018) ND-IJ of, 2018 U. A Review of Percutaneous Transluminal Angioplasty in Hemodialysis Fistula. Int J Vasc Med 1: 1-5.
-
Chang HH, Chang YK, Lu CW, Huang CT, Chien CT, et al. (2016) Statins Improve Long Term Patency of Arteriovenous Fistula for Hemodialysis. Sci Rep 6: 22197.
-
Rundback J (2011) Today KH-E, May undefined, 2011 undefined. TRA for hemodialysis access interventions.
-
Trerotola SO, Turmel Rodrigues LA (2001) Off the beaten path: Transbrachial approach for native fistula interventions. Radiology 218(3): 617-619.
-
Aftab SA, Tay KH, Irani FG, Lo RHG, Gogna A, et al. (2014) Randomized clinical trial of cutting balloon angioplasty versus high-pressure balloon angioplasty in hemodialysis arteriovenous fistula stenoses resistant to conventional balloon angioplasty. J Vasc Interv Radiol 25(2): 190-198.
-
Lucev J, Breznik S, Dinevski D, Ekart R, Rupreht M (2018) Endovascular Treatment of Haemodialysis Arteriovenous Fistula with Drug-Coated Balloon Angioplasty: A Single- Centre Study. Cardiovasc Intervent Radiol 41(6): 882- 889.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review