Aorto-Caval Fistula Following an Abdominal Infrarenal Aneurysm Rupture
Abdominal aortic aneurysms are a chronic dilation of the aorta with a natural history toward enlargement and rupture. It’s a substantial burden on health care. Their incidence has increased during the past two decades, due in part to the aging of the population and the introduction of screening programmes. Although some patients have vague symptoms, such as back pain or abdominal pain, most abdominal aneurysms are asymptomatic until rupture, which leads to death in 66% of patients. The most important complication of infrarenal aortic aneurysms is rupture into the retroperitoneal space or the abdominal cavity. Rupture into the vena cava is uncommon. The incidence of aorto-caval fistulas varies from 2 % to 4 % of the cases. In this article we describe the case of an 81 years old man who had asymptomatic infrarenal aorticaneurysm ruptured into the retroperitoneum and into the inferior veina cava.
Majdi Gueldich*, Héla Ben Jemâa, Saif Hadhri, Nawel Hchaichi, Aymen Damak and Imed Frikha
Patient Report
An 81 years old man with a history of hypertension under medical treatment, consulted at the emergency room and complained from a diffuse and intense abdominal pain progressing from 2 days with no other symptoms. The physical examination revealed a pulsatile and expansive abdominal mass with a diffusely painful abdomen on palpation. The left lower limb had no pulses and no signs of is chemia were noted [1, 2].
The patient wash emodinamically stable without need of any vasoactive drugs, the blood pressure was 110/60 mmHg and the pulse 120 per minute. The blood tests were normal.
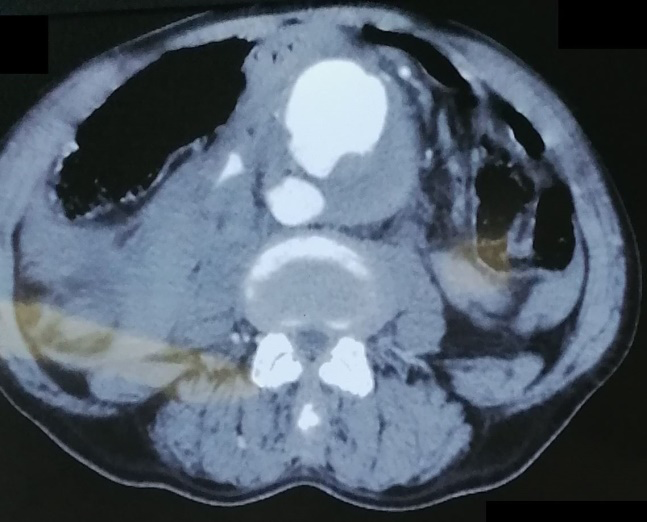
An angiotomo graphy of the aorta was urgently performed and showed a fusi form infrarenalaorticaneurysm measuring 85mm of diameter that was ruptured into the retroperitoneum (Figure 1), the veina cava was opacified in the arterial phase suggesting the presence of an aorto- cavalfistula (Figures 1 & 2). In addition, the common and external left iliacarteries were occluded which explains the absence of pulses in the left lower limb.
We decided after obtaining the patient’s consent, to undertake open repair. A standard midline laparotomy was made. The aneurysm was identified; it extended from the infrarenal level to the aortic bifurcation. The first step was to obtain a proximal and distal control, the aneurysm was then opened so a rush of veneous blood has emerged which we aspirated for later reinfusion via the self-saver. The inferior veina cava was clamped laterally and repaired via a venography. An embolectomy of the left common and external iliacarteries using a fogartycatheter was performed which allowed us to retrieve a thrombus and recover a normal blood flow. The aneurysm was then replaced with a bifurcated graft implanted on the left common femoral artery and the right common iliac artery. The patient had no post-operative events and was discharged from hospital on the 12th post-operative day.

Discussion
Atherosclerosis is the main cause of abdominal aortic aneurysms that ruptured into the inferior veinacava. There are, however, some cases in the literature about caval fistulisation of aneurysms secondary to syphilis, and mycoticarteritis [3–5]. This complication occurs in 4% of ruptured aneurysm cases (almeida 2017). The physio pathology consists of an increasing tension against the aneurysm wall which causes an inflammatory response and results to adhesion into the adjacent structure which is the inferior vena cava and results in erosion of both vessels walls and formation of the fistula [6].
The classic symptom atology consists of a pulsatile abdominal mass, a thrill can be perceived, a right heart failure and signs of venous hypertension. Paradoxical pulmonary embolism may sometimes occur due to thrombi migration from the aneurysmal sac enters in gvenous circulation [7]. Other signs include jugular stasis, dyspnoea, pleural effusion, hepaticstasis, and hematuria [8].
Due to their severity, aortocaval fistulae should be treated as soon as possible.
Open repair is the gold standard treatment but it’s associated with high perioperative mortality that can reach up to 66%. It’s usually due to relatively old patients with several comorbidities especially right heart failure secondary to system is hemodynamic changes caused by a high flow fistula [9]. Intensive and detailed anesthesic management are essential to increase success rate and reduce complications, especially when the fistula is occluded and an acute cardiac decompensation may happen [10].
Other modality of treatment is the endovascular aorticre pair, it gained interest through the recent years and became an interesting alternative, the stent graft deployment effectively seals the fistula in majority of cases [11]. Even though retrograde flow from the inferior mesenteric artery and other collaterals may causes type II endo leak in 20% cases [12]. Some authors [13] start endovascular treatment as a “bridging” procedure to gain time for cardiac recompensation, to allow preparation for later classic surgery [14].
Conclusion
Spontaneous aorto-caval fistula due to the rupture of abdominal aortic aneurysm is a rare but serious condition in vascular surgery with serious outcomes. Open repair remains the gold standard treatment but is associated with mortality rate. The endovascular approach is actually more and more performed due to its simplicity and lower mortality rate.
References
-
Lopes JA, Mansilha A, Teixeira JF (2014) Fístulaaorto- cava-Casoclínico. Angiol E Cir Vasc Mars 10(1): 25‑29.
-
Woolley DS, Spence RK (1995) Aortocaval fistula treated by aortic exclusion. J Vasc Surg 22(5): 639‑642.
-
Landes RG, Trumbull HR, Nicoloff DM (1978) Abdominal aortic aneurysm with rupture into the inferior vena cava associated with horseshoe kidney. Ann Surg Mars 187(3): 329‑331.
-
Reckless JPD, McColl I, Taylor GW (1972) Aorto-Caval Fistulae: An Uncommon Complication of Abdominal Aortic Aneurysms. Br J Surg juin 59(6): 461‑462.
-
Dardik H, Dardik I, Strom MG, Attai L, Carnevale N, et al. (1976) Intravenous rupture of arteriosclerotic aneurysms of the abdominal aorta. Surgery 80(5): 647‑651.
-
Almeida BL de, Rossi FH, Rodrigues TO, Ahouagi LB, Cavalcante SFA, et al. (2017) Tratamento endovascular de aneurisma de aorta abdominal com fístula aorto-cava utilizando oclusor vascular concomitante a endoprótese bifurcada: relato de caso. J Vasc Bras 16(2): 168‑173.
-
Tsolakis JA, Papadoulas S, Kakkos SK, Skroubis G, Siablis D, et al. (1999) Aortocaval fistula in ruptured aneurysms. Eur J Vasc Endovasc Surg 17(5): 390‑393.
-
Rajmohan B (2002) Spontaneous aortocaval fistula. J Postgrad Med 48(3): 203‑205.
-
Cinara IS, Davidovic LB, Kostic DM, Cvetkovic SD, Jakovljevic NS, et al. (2005) Aorto-caval fistulas: a review of eighteen years’ experience. Acta Chir Belg 105(6): 616‑620.
-
Jakanani GC, Chong PL (2008) Pre-operative diagnosis of an unusual complication of abdominal aortic aneurysm on multidetector computed tomography: a case report. Cases J 1(1): 231.
-
Salem RJ (2012) Arteriosclerotic Abdominal Aortic Aneurysm Rupture into the Vena Cava. Tex Heart Inst J 39(6): 866–867.
-
Jones JE, Atkins MD, Brewster DC, Chung TK, Kwolek CJ, et al. (2007) Persistent type 2 endoleak after endovascular repair of abdominal aortic aneurysm is associated with adverse late outcomes. J Vasc Surg. 46(1): 1‑8.
-
Purdy MR, Lutrin DL, Veller MG (2009) Aortocaval fistula--rare complication of ruptured abdominal aortic aneurysms S Afr J Surg 47(3): 86‑88.
-
Siepe M, Koeppe S, Euringer W, Schlensak C (2009) Aorto-caval fistula from acute rupture of an abdominal aortic aneurysm treated with a hybrid approach. J Vasc Surg 49(6): 1574‑1576.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review