Piezosurgery - Safe and Reliable Method for Direct Sinus Lift
Piezosurgery is an alternative technique over conventional oral surgical procedure which is gained popularity in the field of dentistry. It offers a minimally invasive technique that reduces the risk of damage to soft tissues and important structures such as nerves, blood vessels, and the mucosa. This device is being used in osteotomies, periodontology and implantology, oral surgical procedures and in sinus augmentation procedures. The most important features of Piezosurgery include the selective cutting of bone depending on bone mineralization, without damaging the adjacent soft tissue (e.g. vessels, nerves or mucosa), providing a clear visibility in the operating field, and cutting with sensitivity without the generation of heat. This case report illustrates its use in the direct sinus lift procedure.
Introduction
The maxillary and mandibular teeth are commonly associated with endodontic and periodontal problems and are often lost first. Following extraction there is residual alveolar ridge resorption. In the maxilla, pneumatization of sinus may be often seen following tooth extraction. This leads to poor bone quality and reduced bone height posing a challenge in restoration of the tooth using implants with subsequent requirement of bone graft. Sinus lift procedure in posterior maxilla is one of the most important procedures in Implantology to facilitate implant placement in patients with reduced bone height [1, 2].
There are 2 main approaches to the maxillary sinus floor elevation procedure. The first approach includes lateral antrostomy, which is the classic and the more commonly performed technique. Summers advocated the crestal approach, using osteotomes [3]. Pal found that the gain in bone height was significantly greater in direct procedure through lateral antrostomy (mean 8.5 mm) than in indirect method through crestal approach by osteotome technique (mean 4.4 mm) [4].
Schneiderian membrane perforation is one of the most common complication in maxillary sinus augmentation. The conventional approach involves rotary instruments in osteotomy which represents a risk for membrane perforation [5, 6], followed by the manual elevation of the membrane with hand instruments. On the other hand, piezoelectric devices as proposed by Torella, et al. [7] and Vercelotti, et al. [8] may be applied for osteotomy and membrane preparation. Piezoelectric devices are specially designed for osseous surgery which uses low-frequency ultrasonic vibrations that allows a precise cut of bony structures without damaging the soft tissue [9].
Piezoelectric devices usually consist of hand piece and foot control that are connected to the main power unit. It has a holder for the hand piece and contains irrigation fluids that create an adjustable jet of 0–60 ml/min through a peristaltic pump removing debris from the cutting area and maintains a blood-free operating area because of cavitation (production of imploding bubbles) of the irrigation solution giving greater visibility particularly in complex anatomical areas by dispersing coolant fluid as an aerosol [10]. The Piezosurgery device offers three specific therapeutic features attributable to the micro vibrations and to specific modulation of the ultrasound frequency. Firstly, it allows micrometric sectioning, offering superior precision in cutting and with no bone loss. Secondly, the instrument selectively sections mineralized structures, without damaging the adjacent soft tissues, which remain intact even in the case of accidental contact with the device. Lastly, the physical cavitation phenomenon produced by the device ensures less bleeding [11].
This case report presents the direct sinus lift procedure of maxillary posterior edentulous region using Acteon Piezotome Cube and Acteon tips®. The aim of this clinical case report is to illustrate the use of Piezosurgery in direct sinus lift procedure.
Case Description
A female patient, aged 48 years reported to the hospital with chief complaint of missing right upper and left lower back teeth and difficulty in chewing. She wanted to replace them with fixed artificial teeth. History revealed that the teeth were extracted due to caries 4 years back. She was systemically fit and had no history of chronic sinusitis or long-standing nasal obstruction and no other deleterious oral habits.
On clinical examination, teeth no 16, 17 were missing (Figures 1 & 2) with well healed bony ridges. RVG, orthopantomogram findings showed that the bone height was 4mm in 16 &17 regions and was insufficient to place implant. (Figures 3 & 4) So, direct sinus lift was planned with two stage surgery followed by implant placement. Informed consent was obtained after discussing the treatment plan with the patient. Blood investigations were done.
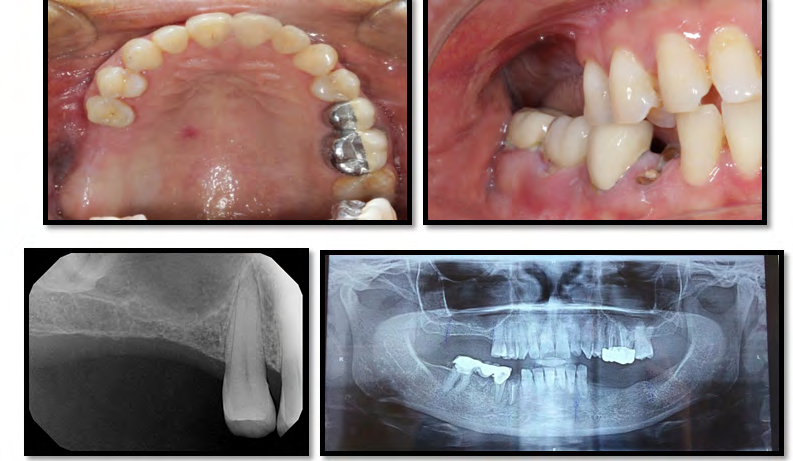
Figure 1-4: Clinical Examination.
Surgical Phase
The maxillary posterior segment was anesthetized with buccal and palatal infiltration using local anesthesia of 2% lignocaine with 1:80,000 adrenaline. An incision was made using #15 surgical blade extending from the distal surface of premolar to the tuberosity region. A vertical incision was placed from premolar to the sulcus. A full thickness buccal flap was raised, and a bony window was then traced using Acteon Piezotome Cube ® and Acteon tips. The initial bone marking was done using tip #BS5. This was followed by the deepening with SL1 tip (Figures 5 & 6). The bone tracing was made until a very thin plate of buccal bone remained over the sinus lining (Figure 7). The lining in the vicinity of the bony window was partially raised and lifted using the SL3 tip. The sinus floor was elevated using sinus floor elevators (Figure 8). The space between bone and sinus lining was filled with PRF (Platelet rich fibrin) and a collagen membrane was placed on top (Figure 9).
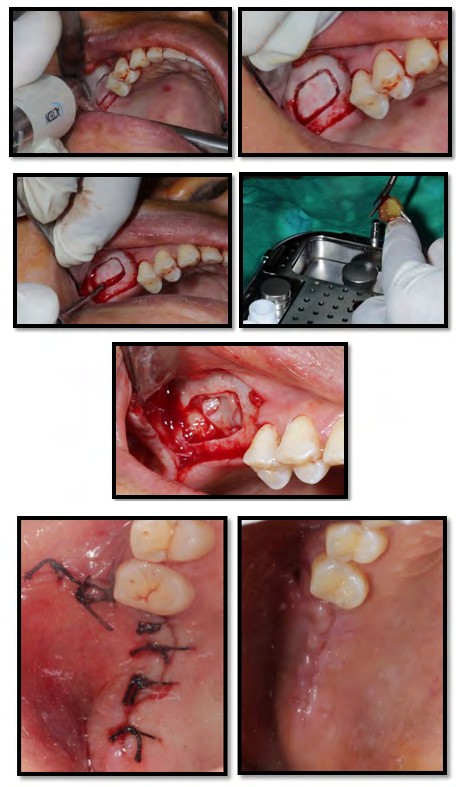
Figure 5-9: Bone Tracing.
Flaps were approximated, and sutured with 3-0 silk (Figure 10). The patient was given postoperative instructions with antibiotic and anti-inflammatory coverage. The patient was recalled after 7 days for evaluation and suture removal (Figure 11).
Figure 10,11: Sutured Structure.
Postoperative assessment of following parameters was done after 1week (Tables 1 & 2).
- Swelling (Present/Absent)
- Complication – If any
| 0 | No pain |
| 3-Jan | Mild pain |
| 7-Mar | Moderate pain |
| 10-Jul | Severe pain |
Table 1: Pain (by Visual Analogous Scale).
| 0 | No inflammation |
| 1 | Mild inflammation |
| 2 | Moderate inflammation |
| 3 | Severe inflammation |
Table 2: Gingival Inflammation Status: Gingival Index.
Postoperatively the patient reported no pain or any inconvenience during the healing period.
On the VAS, score 0 was recorded. Patient took analgesics for only two days. Gingival Index of the surgical site was 0- no inflammation. There was excellent wound healing, with no swelling or nerve and soft tissue injuries. Post-op OPG was obtained after 6 months showed 2mm increase of bone height from the original 4mm .
Discussion
Iatrogenic perforation of sinus lining is higher with the use of rotary instruments. Piezosurgery instrument does not cut the soft tissues had made the surgery easy. It provided a clear vision in our mind as well as on the site due to the bloodless field. Acteon piezotome cube and tips were very easy to handle and are similar to ultrasonic scaler, it was highly precise and were safe during cutting of hard tissue,the hand piece was light in weight the LED light was very convenient in accessing the site during the procedure as there was no need to adjust the light of the dental chair. The selective and thermally harmless nature of Acteon piezotome cube resulted in a low bleeding with clean and smooth cut during surgery. The effects of mechanical instruments on the vital structures such as bone and the viability of cells are important in regenerative surgery. Relatively high temperatures, applied even for a short time, are dangerous to cells, leading to cell death and thereby causing necrosis of tissue [12].
Chiriac, et al., in his research had shown that the healing process after the surgical procedure is facilitated with the use of piezoelectric surgery and reduces inflammatory reaction when the graft is healing, which helps in stabilizing the live bone tissue after it has been grafted [13]. Penarrocha-Diago found perforations of Schneider’s membrane with the rotary technique and ultrasound in 7% and 1.7% of the cases, respectively, with membrane integrity being preserved in 91.2%. The rotary technique afforded a bone gain of 5.9 mm, versus 6.7 mm with ultrasound [14].
Literature shows controversial opinions regarding the osteogenic ability of PRF. PRF alone is mainly used for treatment of maxillary sinus augmentation, intrabony defects (IBD), and tooth extraction. Some studies concluded that PRF alone can improve bone formation, but many scientists doubted this finding [15]. Our case findings showed a bone gain of 2mm only in the augmented region and this is insufficient for implant placement. Thus, we advocate the use of bone graft with PRF for better osteogenic potential.
Harder compared the bone-cutting performance and intraosseous temperature of three modern ultrasonic devices for bone surgery and found that the Piezotome and the Piezosurgery II showed a significantly higher cutting performance than the SurgySonic. The Piezotome produced the smallest increase in intraosseous temperature [16]. Delilbasi compared the intraoperative and postoperative effects of Piezosurgery and conventional rotary instruments in direct sinus lifting procedure and concluded that Sinus lifting procedure performed with Piezosurgery causes less pain and swelling postoperatively compared with conventional technique [17].
Conclusion
Piezosurgery helps in reducing the complications, post- operative complaints and increases the patient’s comfort and efficiency of the novice operator. We feel that Piezosurgery with its ease of cutting and exclusive targeting of hard tissue, its use must be extended to more complexes oral surgery cases and be an essential instrument of every dental operatory.
References
-
Tatum JH (1986) Maxillary and sinus implant reconstructions. Dent Clin North Am 30(2): 207-229.
-
Boyne PJ, James RA (1980) Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg 38(8): 613-616.
-
Woo I, Le BT (2004) Maxillary sinus floor elevation: review of anatomy and two techniques. Implant Dent 13(1): 28-32.
-
Pal US, Sharma NK, Singh RK, Mahammad S, Mehrotra D, et al. (2012) Direct _vs._ indirect sinus lift procedure: A comparison. Natl J Maxillofac Surg 3(1): 31-37.
-
van den Bergh J, ten Bruggenkate C, Krekeler G, Tuinzing D (1998) Sinusfloor elevation and grafting with autogenous iliac crest bone. Clin Oral Implants Res 9(6): 429-435.
-
Kasabah S, Krug J, Simunek A, Lecaro MC (2003) Can we predict maxillary sinus mucosa perforation? Acta Medica (Hradec Kralove) 46(1): 19-23.
-
Torrella F, Pitarch J, Cabanes G, Anitua E (1998) Ultrasonic ostectomy for the surgical approach of the maxillary sinus: a technical note. Int J Oral Maxillofac Implants 13(5): 697-700.
-
Vercellotti T, De Paoli S, Nevins M (2001) The piezoelectric bony window osteotomy and sinus membrane elevation: introduction of a new technique for simplification of the sinus augmentation procedure. Int J Periodontics Restorative Dent 21(6): 561-568.
-
Eggers G, Klein J, Blank J, Hassfeld S (2004) Piezosurgery: an ultrasound device for cutting bone and its use and limitations in maxillofacial surgery. Br J Oral Maxillofac Surg 42(5): 451-453.
-
Deepa D, Jain G, Bansal T (2016) Piezosurgery in dentistry. Journal of Oral Research and Review 8(1): 27- 27.
-
Gupta SJ, Gupta A, Gautam V, Nangia R, Verma P (2015) Stipulative Interdisciplinary Approach Of Piezosurgery In Modern Dentistry. J Pharm Biomed Sci 05(08): 624-
-
Srinivasan S, Ganapathy D, Jain AR (2019) Applications of piezoelectric surgery in dentistry. Drug Invention Today 11(1):122-125.
-
Chiriac G, Herten M, Schwarz F, Rothamel D, Becker J (2005) Autogenous bone chips: influence of a new piezoelectric device (Piezosurgery®) on chip morphology, cell viability and differentiation. J Clin Periodontol 32(9): 994-999.
-
Penarrocha-Diago M, Sanchez-Recio C, Penarrocha-Oltra D, Romero-Millan J (2012) Osteotomy in direct sinus lift. A comparative study of the rotary technique and ultrasound. Med Oral Patol Oral Cir Bucal 17(3): e457- 461.
-
Liu Y, Sun X, Yu J, Wang J, Zhai P, et al. (2019) Platelet-Rich Fibrin as a Bone Graft Material in Oral and Maxillofacial Bone Regeneration: Classification and Summary for Better Application. Biomed Research International.
-
Harder S, Wolfart S, Mehl C, Kern M (2009) Performance of ultrasonic devices for bone surgery and associated intraosseous temperature development. Int J Oral Maxillofac Implants 24(3): 484-490.
-
Delilbasi C, Gurler G (2013) Comparison of Piezosurgery and Conventional Rotative Instruments in Direct Sinus Lifting. Implant Dent 22(6): 662-665.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review