Clinical Management of Neonatal Pneumothorax using Improvised Chest Tube and Suction Machine in Delta State University Teaching Hospital, Nigeria
Neonatal pneumothorax occurs when air leaks into the pleural space. The appropriate size neonatal chest tube with its underwater seal is often not available in many institutions, so we improvise. We present a case report of the clinical management of a two day old male neonate with imperforate anus who had pneumothorax post colostomy creation and our improvised intervention using a size 3 endotracheal tube as our chest tube, 750 ml of water bottle as our underwater seal, and this connected to a suction machine for facilitated drainage of air from the pleural space. This case report is intended to provide an alternative method of intervention in areas where appropriately sized chest tubes underwater seal drainage systems are not available.
Background
Neonatal pneumothorax occurs when air leaks into the pleural space [1]. Its incidence is said to occur in about 1.5 to 7% of neonates in developed countries [2]. It is a life threatening condition that needs prompt intervention to prevent mortality [3]. A high index of suspicion is required to make a diagnosis as sometimes affected neonates are only vaguely symptomatic or they could have varying degrees of respiratory distress with an increasing need for oxygen, in such babies, cold lighting or attempting to illuminate the suspected area of the chest in a darkened room, then ultimately a chest X-ray can be life-saving as it confirms the diagnosis [4].
There are various known causes of neonatal pneumothorax, some of which are traumatic births, aspiration pneumonitis, pneumonia, and non-synchronous continuous positive airway pressure (CPAP), however, the most common attributed cause is intermittent positive pressure ventilation which is thought to over-distend and consequently causes the alveoli to rupture and cause air leak into the pleural space [5]. This is especially true in the presence of underlying lung pathology. Spontaneously occurring pneumothoraxes are not as common as other types of pneumothoraxes [6]. Tension pneumothoraxes need urgent drainage as they are life- threatening, usually first by a needle thoracostomy and thereafter definitive chest tube inserted and connected to an underwater seal with continuous suction [7].
In our institution, Delta State University Teaching Hospital (DELSUTH), and generally across Nigeria, the appropriate size neonatal chest tube with its underwater seal is often not available; so many institutions have to improvise. We describe a case report of spontaneous pneumothorax occurring in a neonate that was managed using an improvised method with a size 3 endotracheal tube as our improvised chest tube and connecting it to an improvised underwater seal which was subsequently attached to a continuous low- pressure suction machine.
This study was approved by the DELSUTH ethical committee with the number: DELSUTH/ HREC/2019/018/0311
Case Report
A two-day-old term male neonate weighing 2.58kg (below 2nd centile) presented to our facility with a history of inability to move bowels since birth due to imperforate anus. He presented with features indicative of large bowel obstruction. There was a normal-looking uncircumcised penile shaft with no passage of meconium or gas in the urine. He was observed to also have bilateral undescended testes which were palpable in the inguinal area. No other external abnormality was observed. There was a positive history in the mother of intake of alcohol-based herbal concoctions during the period of organogenesis (the first three months of pregnancy). Of note, several antenatal ultrasound scans done were reported as normal. Additional investigations done as part of dysmorphology screening on presentation revealed right renal agenesis and sinus venous atrial septal defect. Transfontanelle ultrasound done was normal, and admission chest X-ray done as part of baby gram was unremarkable. A cross-table lateral abdominal X-ray done showed a high rectal pouch so he subsequently had a divided transverse colostomy done. He initially had an uneventful postoperative period recovering fully from anesthesia and breathing spontaneously in room air.
Bowel sounds were heard first-day post-operation with colostomy being functional. Second-day post-operation oral intake was commenced with oral rehydration solution (ORS) and graduated to breast milk by the third-day post-operation.
Mother was being taught how to care for stoma on the fourth-day post-operation. Unexpectedly, on the fifth-day post-operation, the baby developed mild tachypnea with an oxygen requirement for which treatment for pneumonia was commenced. By day 6 post-op, he remains oxygen- dependent but feeds were being tolerated. However on the seventh-day post-operation baby suddenly developed difficulty in breathing with hypoxia. He stopped tolerating feeds with aspirates greater than 30mls/kg/in the 24-hours. On physical examination, the previously comfortable baby had become restless and irritable. He was grunting with make subcostal and intercostal recessions and tachypnea. There was chest wall asymmetry with the affected hemi thorax visibly bulging, desaturations, pallor, cyanosis, and prolonged capillary refill time with skin mottling. He was not pyrexic. The baby was shielded with a dark cloth and the suspected side of the chest was trans illuminated with the torch from a mobile phone. The right side lit up bright red.
At this time his vital signs were respiratory rate of 80 cycles/min, heart rate was 180 beats/min, body temperature was 37.4°C, oxygen saturation was 56% ,and in 10L/min FiO2. His skin was mottled and he was restless with subcostal and intercostal recession. Percussion on the chest revealed right lung dullness in upper and lower lung zones with reduced breath sounds on the right. There was also bilateral pitting edema with an inappropriate weight gain from 2.93kg to 3kg in 24 hours. An urgent chest X-ray was reported as right lung collapse with tension haemopneumothorax and a mediastina shift to the left (Figure 1).

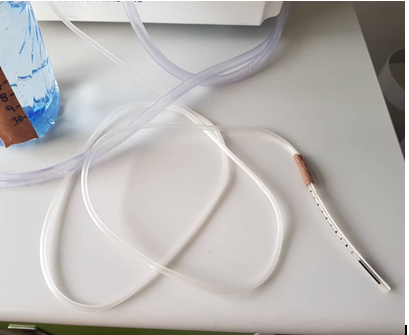
Thereafter a chest tube thoracotomy was done with a size 3 endotracheal tube being improvised as the chest drain. This was secured with purse-string sutures, gauze, and plasters and then connected to an infusion set.
This infusion-giving set was then connected to our improvised underwater seal which was a 750ml water bottle; the tubing was inserted 2cm below the water line and bubbling with 2 tight holes in the plastic cap, an inlet, and outlet. This bottle was kept upright on the floor, then another tubing (outlet) was connected to a suction machine at about -7.5cmH20 to complete the circuit. The suction machine aided in accelerating the removal of air from the pleural space. We interpreted steady, intermittent bubbling as functioning air leak drainage. Analgesia was a 100microg/ kg of morphine, then maintained on 15mg/kg of paracetamol which was given every 6 hours.
The baby was nursed mostly supine with the right side up and received 4hourly gentle chest physiotherapy with suctioning and brief position changes to forestall pressure sores. The tubing from the chest drain was secured to the radiant warmer mattress using plaster tape to reduce pulling traction to avoid the chest drain accidentally disconnecting or dislodging.
Post chest intubation radiograph done after 24 hours revealed a 75% re-expansion evidenced by the presence of broncho-vascular markings with oxygen saturation improving to 98% (Figure 2). Supportive investigations included a full blood count and serum electrolytes which revealed acidosis and anemia which were corrected with intravenous bicarbonate and fresh whole blood transfusion.

On day 13 post-colostomy creation (5th-day post chest tube), the chest X-ray showed the lungs were fully inflated and the chest drain was removed (Figure 3). Of note the vital signs were within normal limits, the stoma was pink and active and he was tolerating direct nipple feeding and expressed breast milk.
He was discharged on the 16th day post-operation and has been follow-up in the outpatient clinic twice, showing good growth and developing well with no residual respiratory compromise. The exact cause of the pneumothorax was not clear. Investigations were limited by financial constraints as parents could not fund CT scan which may have helped delineate the cause of the pneumothorax.

Discussion
This case report highlights that lack of standard equipment does not equate to poor outcomes, and that “necessity is the mother of invention”. A high index of suspicion for pneumothorax by in progressive respiratory distress and its prompt management can be lifesaving in any neonate with sudden onset or sudden worsening of respiratory distress [7]. Tension pneumothorax is a respiratory emergency that demands urgent management. Tension pneumothoraxes are uncommon in our Neonatal Unit, and at the time of managing this baby, we did not have any sort of neonatal thoracostomy pack. We had to urgently improvise and relieve the hemodynamically, respiratory compromised, and significant tension pneumothorax.
We improvised a chest drain, by using an endotracheal tube. We did not have a standard thoracostomy pack but rather we put together various consumables meant for other purposes ingeniously to save the life of the precious neonate. The endotracheal tubes (improvised chest tube) which we connected to the suction machine proved effective in draining the pleural collection, with the advantage of numbered gradations which is helpful for the nurses to record and know when traction is causing the tube to slide out and alert the clinician.
The suction machine created a gentle negative pressure accelerating the removal of fluid and air from the pleural space. The procedure showing how we set this up to create a closed circuit is outlined in the diagram below (Figures 4-6).

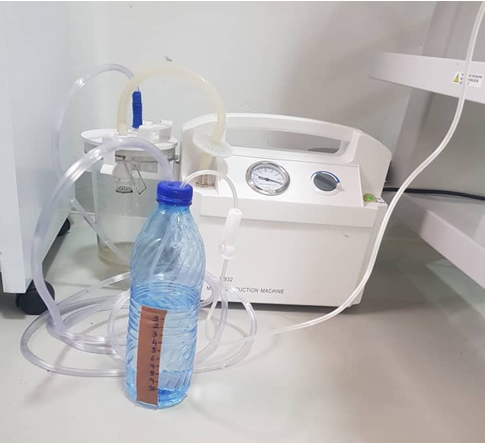
Figure 5: Infusion-giving set connected to our improvised underwater seal which was a 750ml water bottle; the tubing was inserted 2cm below the water line and bubbling with 2 tight holes in the plastic cap, an inlet(infusion set), and outlet. Bottle was kept upright on the floor, then another tubing (outlet) was connected suction machine at about -7.5cmH20 to complete the circuit.
Chest X-rays where available are a useful diagnostic tool in any neonate with respiratory distress. Our report reiterates why any baby with respiratory instability should have an urgent chest X-ray done. However, the role of a careful and detailed chest examination cannot be overemphasized and more so in a critically ill baby in a resource-limited setting where portable X-ray is not readily available and radiology services in general limited [3]. Chest examination findings suggestive of pneumothorax include reduced or absent breath sounds on a bulged hemithorax, tachypnea, and distant heart sounds, and reduced oxygen saturation in a baby with respiratory distress. An emergency needle chest decompression via the second intercostal space mid-clavicle line can be done in a critically ill neonate followed by chest drain thoracostomy [1].
Male are more predisposed, and there’s a known association of spontaneous pneumothorax with major congenital renal pathologies [8]. Our patient has right renal agenesis. There was also an association with cardiac anomalies. Cardiac echo in this case, revealed a sinus venous atrial septal defect.
Conclusion
This case report was intended to provide an alternative method of intervention for symptomatic neonatal pneumothorax in areas where appropriately sized chest tubes and underwater seals are not available.
References
-
Bruschettini M, Romantsik O, Ramenghi LA, Zappettini S, Donnell OCPF, et al. (2016) Needle aspiration versus intercostal tube drainage for pneumothorax in the newborn. Cochrane Database Syst Rev 11(1): CD011724.
-
Duong HH, Mirea L, Shah PS, Yang J, Lee SK, et al. (2014) Pneumothorax in neonates: trends, predictors and outcomes. J Neonatal Perinatal Med 7(1): 29-38.
-
Merscher Alves MB, Conte N, Sory Diallo I, Roth Kleiner M (2021) Clinical presentation and improvised management of neonatal pneumothorax in the setting of a low-resource country: Conakry, Guinea. BMJ Case Rep 14(3): e235801.
-
Huseynov M, Hakalmaz AE (2021) Neonatal pneumothorax from the perspective of a pediatric surgeon: classification and management protocol: a preliminary algorithm. Turk J Med Sci 51(3): 1201-1210.
-
Wyatt TH (1995) Pneumothorax in the neonate. J Obstet Gynecol Neonatal Nurs 24(3): 211-218.
-
Arora K, Panda SS, Das RR, Mohanty PK, Panda M (2014) Primary spontaneous bilateral pneumothorax in a neonate. APSP J Case Rep 5(3): 31.
-
Ashmore PG (1965) Spontaneous Pneumothorax in the Newborn. Can Med Assoc J 92(7): 309-311. .
-
Boone PM, Scott RM, Marciniak SJ, Henske EP, Raby BA (2019) The Genetics of Pneumothorax. Am J Respir Crit Care Med 199(11): 1344-1357.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review