Mesenteric Cystic Lymphangioma Induced Recurrent Abdominal Pain And Signs of Intestinal Obstruction: A Case Report
Mesenteric cystic lymphangioma is an uncommon benign abdominal mass. This is a case of a 40-year-old female who presented to the hospital with recurrent abdominal pain and distention. Computed Tomography and magnetic resonance imaging tests suggested a mesenteric cyst. The patient underwent laparotomy which confirmed the presence of a mesenteric cyst along with small bowel narrowing at the site of the cyst caused by multiple adhesive bands released during the procedure. The cyst was found and excised approximately 200 cm away from the ileocecal junction, and was pathologically confirmed to be a mesenteric cystic lymphangioma. These findings support that mesenteric cystic lymphangioma could cause chronic abdominal pain and intestinal obstruction.
Introduction
Mesenteric cystic lymphangioma is a benign fluid-filled cyst originating from a lymphatic system malformation [1]. The exact cause of cystic lymphangiomas remains unknown. However, one of the main causes of this condition, as per the scientific study of Aprea G, et al. [2] is a congenital malformation of the lymphatic system. The condition has also been associated with abdominal trauma, lymphatic obstruction and inflammation. In the abdomen, cystic lymphangiomas occur mostly in the mesentery, omentum, and mesocolon [3]. Mesenteric cystic lymphangiomas constitute an admission rate of 1/100,000 and 1/200,000 in children, according to Guachilema R, et al. [4]. The condition is also more common in men than women, with a ratio of 3:1[4]. Below is a case of a 40-year-old female who presented to the hospital with clinical manifestations of mesenteric cystic lymphangioma.
A 40-year-old female presented to hospital with recurrent abdominal pain in the right iliac fossa associated with abdominal distention and constipation. On examination, the patient was vitally stable; Laboratory tests were within the normal ranges except the presence of luekocytosis of 14.9 result value. Upon physical exam, patient was alert, conscious and oriented in time, place and person. The patient was systematically normal expect having abdominal distention and severe defused abdominal pain mostly at the right iliac fossa region. Firstly, computed tomography (CT) of the pelvis and abdomen showed an oblong-shaped cystic lesion in the suprapubic area related to the anterior aspect of the urinary bladder inferiorly, fundus of the uterus, posteriorly and bowel loops antero-superiorly. It measured about 2.6 X 4.9 X 6.2 cm. In addition, the lesion showed dense peripheral calcification with no CT evidence of septation or enhancing soft tissue component. There was another notable cystic lesion at the right iliac fossa region with small bowl loops insinuated among them. This lesion measured 5.5 X 6.2 X 1.04 cm in the maximum diameter with no calcification (Figure 1).
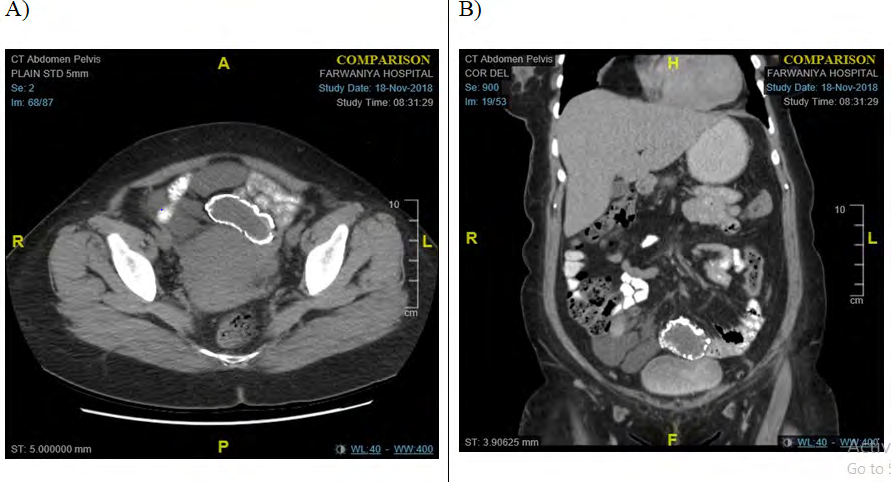
A) Plain axial view; B) Delyed coronal view Figure 1: CT abdomen and pelvis showing suprapubic and right iliac fossa cysts.
Secondly, magnetic resonance imaging (MRI) revealed multi-loculated peritoneal cystic lesions located anteriorly in the pelvic region deep to the anterior abdominal wall with small bowel loops seen insinuated among them, with the largest locule seen in the right iliac fossa. These lesions measured 5.4 X 4.5 X 3.6 cm in the maximum dimensions with no definite encasement or solid component. Besides these lesions, another oblong cystic lesion was identified superiorly to the uterine fundus. The lesion measured 2.8 X 4.6 X 6.2 cm, showing mixed signal intensity denoting marginal calcification and no detected internal septation or enhancing soft tissue component (Figure 2).
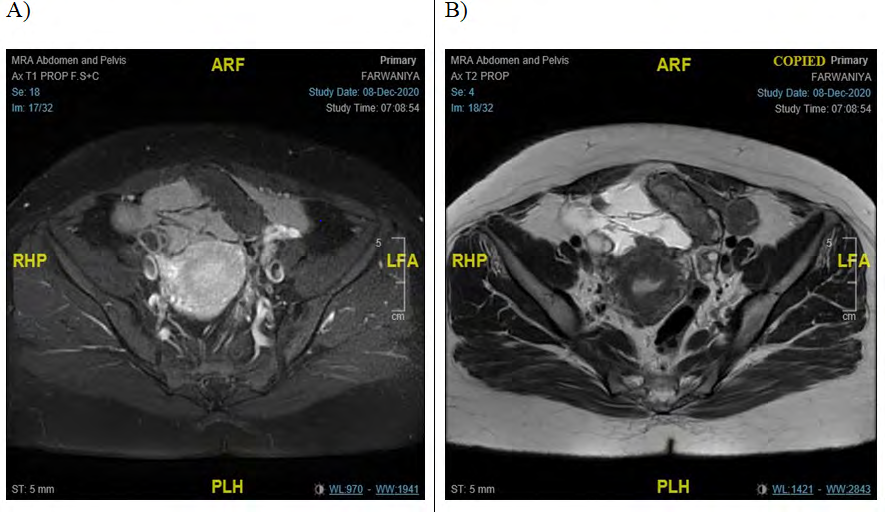
A) Axial T1 PROP F.S+C view; B) Axial T1& T2 PROP view Figure 2: MRI showing multi-loculated peritoneal cystic lesions.
A diagnostic laparoscopic exploration was performed which established a large multi-loculated cyst related to the small bowl with one calcified area. A decision was made to convert to open laparotomy with a lower midline incision. Besides this cyst, there were multiple adhesive bands with one proximal to the cyst causing small bowl narrowing, which were all released. The cyst was approximately 200 cm away from the ileocecal junction; due to the caution of compromising the vascular supply to the bowel, resection and hand-sewn end-to-end anastomosis were done. A histopathological examination was then carried out. The resection specimen confirmed the diagnosis of a small intestine segment with mesenteric cyst: in keeping with a mesenteric lymphangioma (Figure 3).

Figure 3A: Laparoscopic view of a large multi-loculated cyst related to the small bowl with one calcified area.
Figure 3B: Multiple adhesive bands with one proximal to the cyst causing small bowl narrowing. The cyst was approximately 200 cm away from the ileocecal junction.

Figure 3C: Multiple adhesive bands with one proximal to the cyst causing small bowl narrowing. The cyst was approximately 200 cm away from the ileocecal junction.
Figure 3D: Multiple adhesive bands with one proximal to the cyst causing small bowl narrowing. The cyst was approximately 200 cm away from the ileocecal junction.
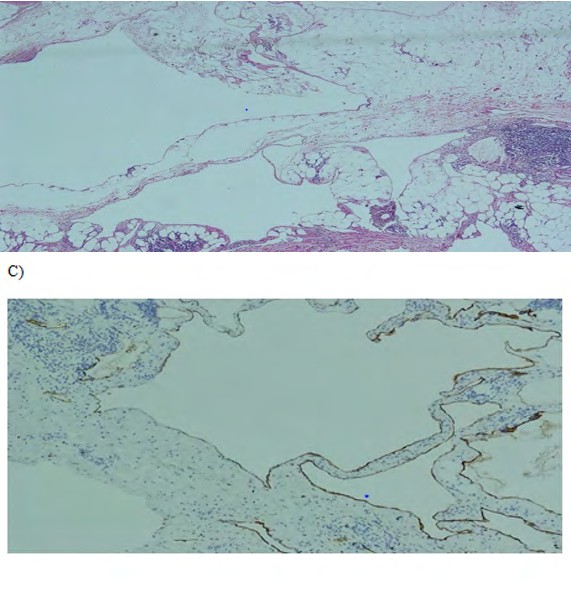
Figure 4B: Dilated lymphatic spaces associated at foci with lymphoid aggregates and smooth muscle (Haematoxylin and Eosin stain, x40).
Figure 4C: Immunohistochemical study of the lining cells of the cystic spaces show strong immunoreactivity with D2-40 (D2- 40 Immunohistochemical stain, x100).
Discussion
Four types of intra-abdominal lymphangiomas are identified; pedicled, sessile, retroperitoneal, and multicentric. Cystic lymphangiomas are usually asymptomatic, one of the main reasons they reach a large size. However, patients may later present with abdominal discomfort, distention, or any complications in the peritoneal cavity such as infection, rupture, hemorrhage, and intestinal obstruction, all possible pointers that the patient may have an intra-abdominal lymphangioma [5].
In agreement with the study of Guachilema R et al. [4] laboratory tests are not always useful [4]. The ultrasonography presentation of a mesenteric lymphangioma is described as a cystic lesion (honeycomb pattern). On CT imaging, the mesenteric lymphangiomas are observed as uni- or multi- locular masses with an enhancement of the wall and septum by contrast medium. However, these investigation help to identify if the mass is cystic, its size, and location, but they are futile in establishing an accurate diagnosis. Magnetic resonance tests are one of the most useful and reliable radiological methods for diagnosis and surgical decisions. Magnetic resonance imaging is likely to be considered in differentiating the mesenteric cyst from lymphangioma because it shows the differences between cystic and septal structures [2].
The definitive diagnosis of lymphangioma is based on histopathology and immunochemistry. The vague scenarios of intra-abdominal lymphangiomas, when presented to the emergency room with complications such as hemorrhage and/or intestinal obstruction, will lead many physicians to approach urgent surgical interventions. While most mesenteric cystic lymphangiomas require simple surgical excision, it is sometimes required to perform partial bowel resection. Most post-operative patients do well with a very low recurrence rate [6].
Conclusion
This case report highlights that intra-abdominal lymphangiomas can sometimes be life-threatening if not diagnosed and treated correctly. The clinical condition has been established to have a low recurrence rate post-operatively with good prognosis. Most of the case presentations are vague with many differential diagnoses, and the definitive one is based on histopathology. The most appropriate treatment choice is surgical excision.
References
-
Kashogi G, Prasetya D, Fauzi AR, Daryanto E, Dwihantoro A (2019) Pediatric patients with mesenteric cystic lymphangioma: a case series. International Journal of Surgery Case Reports 64: 89-93.
-
Aprea G, Guida F, Canfora A, Ferronetti A, Giugliano A, et al. (2013) Mesenteric cystic lymphangioma in adult: a case series and review of the literature. BMC Surgery 13(1): 1-5.
-
Aliukonis V, Lasinskas M, Pilvelis A, Gradauskas A (2021) Pathological discrepancy: simple mesenteric cyst vs. mesenteric lymphangioma. Case Rep Surg, pp: 1-5.
-
Guachilema RA, Monard ART, Endara MC, Garcia CG, Sandoval MO, et al. (2020) Intra-abdominal cystic lymphangioma of the mesocolon sigmoids: a rare entity in adult patient woman. J Surg Case Rep (5): rjaa031.
-
Banerjee JK, Bharathi RS, Venkatesan S, Singh G (2016) Abdominal lymphangioma. Med J Armed Forces India 72(S1): S70- S73.
-
Abdulraheem AK, Al Sharie AH, Al Shalakhti MH, Alayoub SY, Al Domaidat HM, et al. (2021) Mesenteric cystic lymphangioma: A case. Int J Surg Case Rep (80): 105659.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review