Robotic Simple Prostatectomy for Giant Prostate
Benign prostatic hyperplasia (BPH) is a pathological process that contributes to, but is not the sole cause of lower urinary tract symptoms (LUTS) instead age-related detrusor changes and other common medical conditions are the causative factor in many cases. Despite this, benign prostatic hyperplasia (BPH) is still a significant cause of LUTS. The options for management are variable and include watchful waiting, medical therapy, and surgical intervention. Simple robotic prostatectomy was used as the treatment procedure of choice for the patient in this report since he has a large prostate, and according to the AUA and EAU guidelines, surgical management with prostatectomy is the gold standard for such cases. The benefits of using such a technique include precise removal of the prostate gland, minimal blood loss, a smaller opening, less pain, short stay in the hospital, and a reduced requirement for blood transfusion. In the end, it was one of the preferred methods to be utilized for prostate surgery.
Hani Albadawe* and Khalid Alothman#
Johns Hopkins Aramco Healthcare, Saudi Arabia
#Equally contributed towards this Article
Introduction
The condition known as benign prostatic hyperplasia (BPH) is one of the conditions that is diagnosed the vast majority of the time in urologic offices. Even though there are many more options for treating symptomatic bladder outlet obstruction now than there were several decades ago, the simple prostatectomy is still the treatment of choice for complicated bladder outlet obstruction that is associated with a large prostate volume, which is typically greater than 80 g. This is the case despite the fact that treatment options for symptomatic bladder outlet obstruction have dramatically increased over the past few decades. Transurethral resection of the prostate (TURP) is a viable alternative for the treatment of very large prostates; nevertheless, it might generate unsatisfactory outcomes, particularly with monopolar TURP, and it may put patients at risk for post-transurethral resection syndrome. It has also been found that between 12 and 15.5% of patients who underwent TURP required additional surgery, but only between 1.8 and 4.5% of patients who underwent open surgery required additional procedures after eight years. A simple prostatectomy is not simple in either its technique or its indication, and it has the potential to cause both short- term and long-term consequences, some of which may be clinically more important than those that result from a radical prostatectomy. In addition, a simple prostatectomy can be performed only when radical prostatectomy is not an option. When compared to men who undergo a radical prostatectomy, those who get a simple prostatectomy are often older and suffer from a greater number of medical issues. The use of surgery for prostatic hypertrophy, including transurethral and open procedures, has considerably changed as a result of the development of contemporary medical treatment for prostatic enlargement. When an open prostatectomy is performed today, the patient has frequently undergone years of ineffective medical treatment, may have experienced chronic urine retention, and may also be dealing with the long-term implications of chronic bladder outlet obstruction. As a result, when this procedure is performed, the patient has frequently undergone an open prostatectomy. Open surgery in these men has a long history of being associated with a higher risk of incontinence, a longer length of stay in the hospital, significant blood loss, and a transfusion rate that is more than 25 percent. Even though open prostatectomy is a viable treatment option, there are a number of significant risks involved, one of which being bleeding [1, 2, 3]. Requires a transfusion, harm to the sphincter, neurovascular bundle, or rectal area, as well as a lengthier hospital stay and more time spent catheterizing the patient. Following the development of the laparoscopic method for treating prostate cancer, the contemporary era of minimally invasive surgery for benign prostatic hyperplasia (BPH) began many years and several hundred cases later. By the year 2005, medical organisations that already had expertise doing robot-assisted laparoscopic prostatectomy (RALP) had started applying the method to treat benign prostatic illnesses like BPH. Eugene Fuller was the first person to execute an open prostatectomy by the use of cystotomy in the year 1894. Following this, Peter Freyer in the year 1900 and Robert Proust in the early 1910s popularised the procedure. In 1904, Young came up with the idea of doing a perineal prostatectomy instead of a cystotomy. Millin proposed a purely retropubic approach for more control over the prostatic apex during enucleation to avoid traction injury to the urethral sphincter, and for more adequate prostatic exposure at the expense of bladder accessibility. During the procedure, this would allow for more adequate prostatic exposure. The open surgical method remained the gold standard for one hundred years, with the majority of patients receiving suprapubic approaches, then retropubic, and finally the perineal prostatectomy, which was pioneered by Young in October of 1902. The first laparoscopic radical prostatectomy was carried out by Schuessler in 1991, and further iterations were carried out by Bertrand Guillonneau, Guy Vallencien, and Claude Abbou during the late 1990s. This marked the beginning of a significant shift in the field. Mirandolino Mariano is largely recognised as the first surgeon to purposely course down the retro-adenomatous plane to perform a pure laparoscopic simple prostatectomy (LSP) of a 173 g prostate. This was done in order to deliver obstructive adenomas and deliver a retro-adenomatous plane. According to reports, one of the advantages of this method is that it allows for better sight of the adenoma, as well as venous tamponade due to the use of pneumoperitoneum during the dissection. as well as the prevention of a significant incision in the lower abdominal region. The disadvantages included the difficultly in mechanically manipulating particularly big adenomas during laparoscopic surgery, a steep learning curve, and the necessity for sophisticated suturing during capsule plication and advancement of the bladder [4].
Additional drawbacks included the typical laparoscopic instruments’ inability to articulate, as well as the restricted working space, which made it difficult to insert plicating, anastomotic, and hemostatic sutures. LSP did, however, improve upon blood loss and length of stay when compared to similar series of open prostatectomy and may be performed safely and successfully for the treatment of bladder outlet obstruction that is caused by BPH. The introduction of robotic surgery has largely replaced traditional laparoscopic procedures for the treatment of benign diseases, much in the same way that robotics has done the same for radical surgery. Binder et al. successfully carried out the very first radical robotic prostatectomy in Hanover in the year 2000 as part of a group effort that was a pioneering endeavor in the utilization of the da Vinci platform. Laparoscopic procedures for cancer surgery were significantly simplified with the introduction of robotic prostatectomy, which also facilitated greater patient access to the procedure. As the use of robotics in cancer surgery became more widespread, the possibility of its application in benign surgery also emerged. After years of expertise performing prostatectomy procedures laparoscopic ally, Sotelo et al. are credited with being the first group to conduct a basic robotic prostatectomy in 2008. In comparison to laparoscopy, robotic surgery has the potential to have a shorter learning curve, particularly in terms of suturing techniques. In addition, robotic surgery may share some of the advantages of laparoscopy, such as a lower risk of perioperative morbidity, increased visibility and precision, a quicker recovery time, and the capacity to demonstrate surgical techniques and disseminate surgical skills through the sharing of surgical videos on the internet and various social media platforms. The cost of the equipment, lengthier surgical periods, the possibility of partial resections, and the trans peritoneal invasiveness of the procedure are all drawbacks of the robotic technique.
Benign prostatic hyperplasia (BPH) is a common ailment that occurs in males as they get older. It is also sometimes referred to as prostate gland enlargement. In people with an enlarged prostate gland, Lower urinary tract symptoms can occur [5]. Treatment for the BPH is Variable including watchful waiting in the mild symptoms, medical therapy and surgical intervention. The Urologist select the best option for the patients for dealing with the symptoms. Based on the size of the prostate, patient health condition and the preferences of the treatment [5].
In this report, the case of the patient with benign prostatic hyperplasia is discussed along with the treatment. The treatment that was given is a robotic simple prostatectomy.
Case Report
78-year-old Saudi male patient. He has a past medical history of TIA (transient ischemic attack), carotid stenosis, and coronary artery disease status post-percutaneous coronary angioplasty.
Presented initially to us in the urology clinic with a long- standing history of obstructed lower urinary tract symptoms with severe IPSS, we started him on an alpha-blocker and then added a 5-alpha reductase inhibitor to control his symptoms.
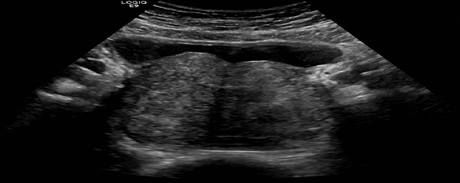
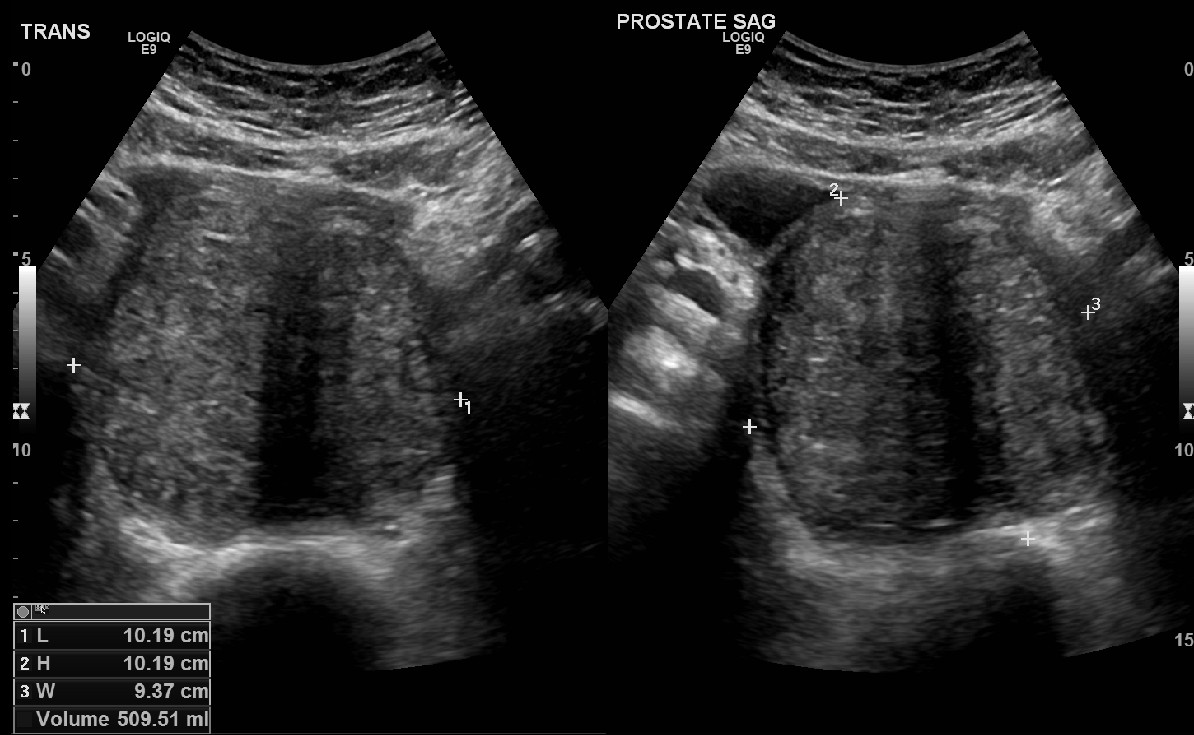
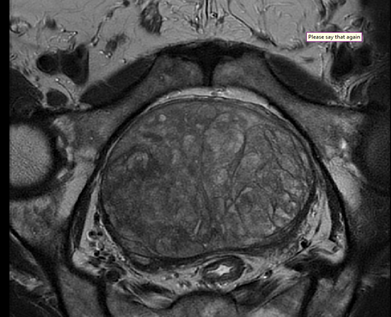
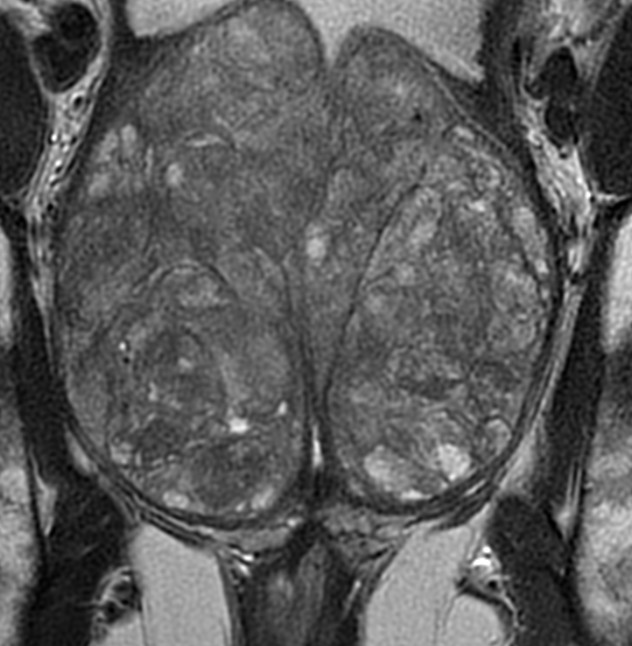
Recently, the patient’s symptoms aggravated, and he went on multiple episodes of recurrent urinary retention, which required catheterization. Initial Renal Ultrasound showed normal upper tract system without sign of hydronephrosis, huge enlarged prostate measuring around 509 g with postvoid residual around 40%. MRI was done for more clarification of the underlying prostate pathology it showed benign prostate with PI-RAD 1 with estimated prostate size at around 500 g . We proceeded with a diagnostic flexible cystoscopy. The cystoscopy showed a hugely enlarged prostate, and we were able to reach the bladder. The bladder was moderately trabeculated we didn’t see any lesions in the bladder (Figures 1-6).
The patient’s PSA level was 9.7ng/dl and then trended down to 3.7ng/dl after initiation of the 5 alpha reductase inhibitors.
MRI Results
Procedure
Post-operative Condition/Outcomes of the Surgical Procedure.
Patient and Methods
A comprehensive clinical description of our patient, including all relevant symptoms, PSA levels, uroflow measurements, cystoscope images, US bladder images, and MRI results.
Surgical Technique
The procedure was carried out using the da Vinci Surgical System Xi (Intuitive Surgical, Sunnyvale, California, United States), and patients were positioned in lithotomy and steep Trendelenburg positions during the operation. Our method includes performing a radical prostatectomy through a transperitoneal incision, using a six-port placement that is comparable to that of a robotic procedure. The dome of the bladder has been located, and a cystotomy in the midline has been performed. Two stay sutures made of 2-0 Vicryl and placed on a CT-1 needle are utilized in order to maintain the openness of the edges of the cystotomy for access to the prostate. Both of the ureteral orifices were located, and a feeding tube with a diameter of 5 French was inserted into each ureter. We have discovered that feeding tubes are preferable to ureteral stents because they can be adjusted more readily and do not impede prostate dissection. To facilitate the dissection process, a traction suture made of 2-0 Vicryl threaded via a CT-1 needle is put through the median lobe of the adenoma. This is followed by the placement of a second suture inferiorly as the dissection process continues. An incision is created in the mucosa that is covering the adenoma, beginning in the back of the mouth. Enucleation is conducted with monopolar scissors and blunt dissection after it has been determined where the plane is that is between the prostatic capsule and the adenoma. The dissection will begin in the posterior region, then go laterally, and then move forward into the anterior region. Due to the enormous size of the adenoma, after dividing the anterior commissure, the adenoma was cut into two sections, and each of those parts was placed in a separate bag. Hemostasis was achieved by direct cautery and suture ligation of specific bleeding spots in the prostatic fossa, which was then followed by continuous prostatic fossa closure using 2.0 V-lock suture (Covidien, Norwalk, Connecticut, United States). A 22F three-way catheter is inserted, and both of the patient’s feeding tubes are withdrawn. The balloon inside the catheter is inflated to 30 ml. in addition, 2-0 V-Loc sutures are used to seal the cystotomy (Covidien, Norwalk, CT, USA). The procedure is finished by inserting a Jackson-Pratt drain into the rectovesical pouch, which is then followed by the removal of the specimen and the closure of the fascia and skin.
The patient was progressing well and was discharged home with foley catheter witch was removed later on in the clinic.
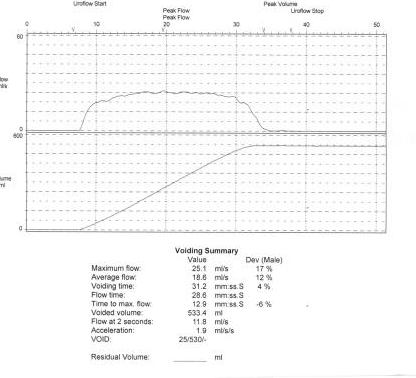
Follow up Uroflow was done witch showed significant improvement in his voiding stream with Qmax: 25.1 ml/s, voidied volume 533 ml and with no significant post void residual.

Discussion
The prostatic enlargement that weighs more than 500 grams, commonly known as Giant Prostatic Enlargement (GPE), is an extremely uncommon form of the condition [6, 7]. Even fewer publications have been published that describe the function that robotic surgery plays in the management of this condition.
Our case report demonstrates that robotic simple prostatectomy is an effective treatment for benign prostatic hyperplasia (BPH), with favorable perioperative outcomes and great short-term symptomatic and functional improvements. Men who have a prostate that weighs more than 100 grams typically benefit from open surgical prostatectomy (OSP) or holmium laser enucleating as their therapy of choice. These laser therapies have been shown to have equal short-term effects when compared with OSP for large glands in randomized clinical studies. This was demonstrated in terms of improvements in IPSS, Qmax, and PVR. The high incidence of bleeding during surgery is one of the most significant issues associated with OSP. A randomized experiment that compared open prostatectomy with HoLEP for glands greater than 100 g found that open prostatectomy had a higher rate of adverse events (26.7% vs. 15%), partly as a result of the 13.3% rate of perioperative blood transfusions. HoLEP had a lower rate of adverse events (5%).
When compared to open surgical prostatectomy (OSP), laparoscopic surgical prostatectomy (LSP), which is a minimally invasive method, has been demonstrated to have less pain and a shorter convalescence period than OSP. On the other hand, a study demonstrated that perioperative bleeding that resulted in the requirement of a blood transfusion was still a worrisome issue with LSP.
This is probably due to the poor ergonomics of pure laparoscopy when doing surgery within the confined space of the pelvis, as well as the following difficulties of dissecting and suturing blood veins inside the body. The capacity to locate small bleeding vessels and exert control over them is much improved by the use of robotic systems, which also enable clear vision and make intracorporal suturing much simpler to accomplish. This makes it easier to control bleeding and lessens the likelihood that perioperative blood may need to be transfused.
Conclusion
Simple Robotic prostatectomy is a safe, efficient, and well-tolerated BPH treatment that can be carried out in a number of ways. Costs are playing a bigger role in decision-making in the modern healthcare environment. A comparison between perceived and actual benefits of various technologies must be made when determining whether it is cost-effective to invest in new technology or go to remote locations. Robotic simple prostatectomy has the advantage of shortening hospital stays and catheter stays while producing results similar to those shown by open simple prostatectomy in terms of reduced symptoms of the lower urinary tract and appropriate bladder emptying.
References
-
Lim KB (2017) Epidemiology of clinical benign prostatic hyperplasia. Asian journal of urology 4(3): 148-151.
-
Langan RC (2019) Benign Prostatic Hyperplasia. Primary care 46(2): 223-232.
-
Lokeshwar SD, Harper BT, Webb E, Jordan A, Dykes TA, et al. (2019) Epidemiology and treatment modalities for the management of benign prostatic hyperplasia. Translational Andrology and Urology 8(5): 529-539.
-
Miernik A, Gratzke C (2020) Current Treatment for Benign Prostatic Hyperplasia. Deutsches Arzteblatt international 117(49): 843-854.
-
Ng M, Baradhi KM (2022) Benign Prostatic Hyperplasia. StatPearls Publishing.
-
Vasanwala FF, Wong M, Ho H, Foo KT (2017) Benign prostatic hyperplasia and male lower urinary symptoms: A guide for family physicians. Asian Journal of Urology 4(3): 181-184.
-
Jiwrajka M, Yaxley W, Ranasinghe S, Perera M, Roberts MJ, et al. (2018) Drugs for benign prostatic hypertrophy. Australian Prescriber 41(5): 150-153.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review