Rare Cases of Primary Glioblastoma Multiforme in the Cervical Spinal Cord, Report of Two Cases and Literature Review
Glioblastoma multiforme (GBM) is a highly aggressive and malignant tumor that can arise in the central nervous system, including the spinal cord. We presented two cases of GBM in spinal cord and cerebellum, respectively. First, 36-year-old female who presented to our clinic with a two-month history of progressive lower and upper extremities weakness and numbness. He also reported difficulty with urination and defecation. Second patient was 19 years-old-man with history of extremities weakness and neck pain. MRI demonstrated enhanced intra-medullary tumor in cervical spine. Both patients underwent surgical resection, followed by radiation therapy and chemotherapy. Further researches are needed to identify optimal treatment strategies and improve outcomes for patients with GBM in the spinal cord. Close monitoring and follow-up care are essential to manage potential complications and optimize quality of life for affected individuals.
Introduction
Glioblastoma multiforme (GBM) is a malignant tumor that can arise in the spinal cord. Despite its rarity, it is an aggressive cancer that progresses rapidly and can metastasize to other parts of the body [1]. GBM in the spinal cord can manifest with range of symptoms, including sensory disturbances, motor weakness, and bowel and bladder dysfunction. The diagnosis of GBM in the spinal cord is usually based on imaging studies, such as magnetic resonance imaging (MRI), and confirmed by biopsy [2]. The primary types of spinal cord tumors that are commonly found are astrocytomas and ependymomas. Spinal cord tumors are classified into two main types, namely astrocytomas and ependymomas [3]. While ependymomas are more commonly seen in adults, astrocytomas are frequently diagnosed in children [4]. Among the primary spinal cord tumors, glioblastoma multiforme (GBM) of the spinal cord is a rare subtype and accounts for only 1.5% of cases [5]. Primary spinal cord tumors can be treated with various therapies, including radiation therapy alone or in combination with chemotherapy, surgery alone, surgery with adjunct therapy, and palliative therapy [6]. Unfortunately, the prognosis for patients with primary spinal cord glioblastomas is generally poor, with less than 200 cases reported in the literature as of April 2017 [7]. A review of 190 documented cases of primary GBM of the spinal cord in the National Cancer Database found that the median survival time was 11.2 months [8, 9, 10, 11, 12]. Despite their rarity, glioblastomas in the cerebellum pose unique challenges for diagnosis and treatment due to the complex anatomy and function of this brain region. The cerebellum is responsible for motor coordination and balance, and any disruption to its normal function can have significant consequences for a person’s quality of life [13]. Symptoms of a cerebellar glioblastoma may include headaches, nausea, vomiting, difficulty with balance and coordination, and changes in vision or hearing. Diagnosis typically involves imaging studies such as MRI or CT scans, followed by a biopsy to confirm the presence of a glioblastoma. Despite advances in treatment, the prognosis for GBM in the spinal cord remains poor, with a median survival time of less than two years. However, early detection and prompt treatment can help improve outcomes for patients with this condition. Close monitoring and follow- up care are essential to manage potential complications and optimize quality of life for affected individuals. The aim of this article is to provide an overview of glioblastoma multiforme (GBM) in the spinal cord, including rare cases and their manifestations, diagnosis, and treatment options. The article will also discuss the prognosis for patients with primary spinal cord glioblastomas and highlight the challenges associated with the diagnosis and treatment of glioblastomas in the cerebellum.
Case Presentation
Case 1
The patient was a 36-year-old female who presented to our clinic with a two-month history of progressive lower and upper extremities weakness and numbness. He also reported difficulty with urination and defecation. The patient had a no past medical history and otherwise healthy. He denied any history of trauma or recent illness.
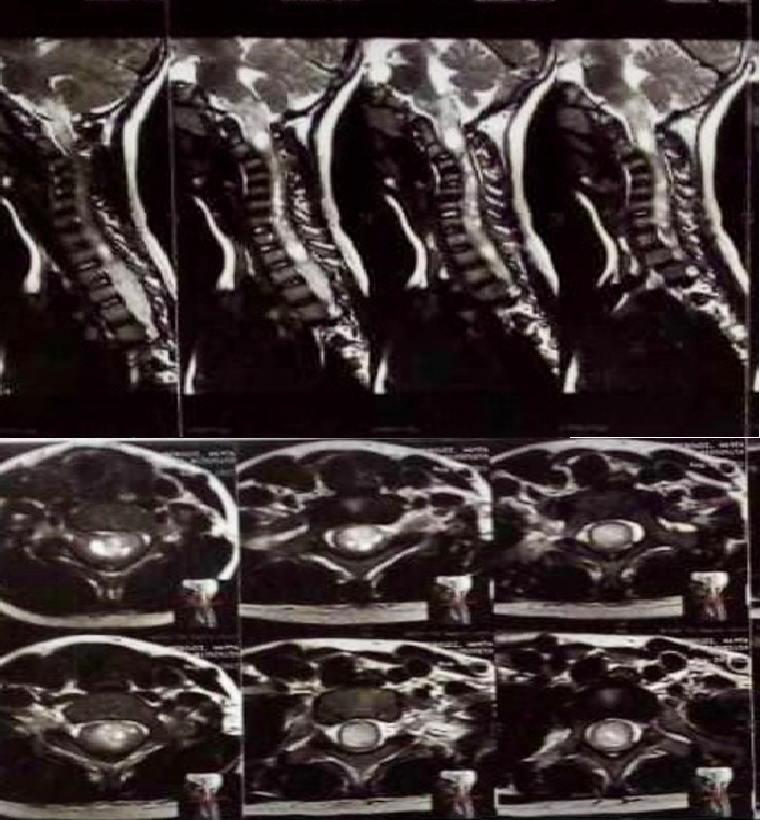
Physical examination revealed 3/5 strength in the lower and upper extremities, with reduced sensation to light touch and pinprick below the T2 level. The patient had a normal gait and no abnormalities in upper extremity strength or sensation. He had no cranial nerve deficits, and mental status was normal. The patient was referred to our hospital for further evaluation and treatment. MRI of the cervical spine revealed an enhancing mass lesion at the C1- C7 Level with significant spinal cord compression (Figure 1). The lesion appeared to be arising from the spinal cord itself, with no significant extension into the surrounding tissues. Brain MRI revealed no mass lesion. Given the concerning imaging findings, the patient underwent a spinal cord biopsy. Pathology revealed a high-grade glioma consistent with GBM. A surgical procedure was carried out to perform a laminectomy of C1-C7 and debulk an intramedullary mass. The tumor could not be completely removed due to its nature.
Case 2
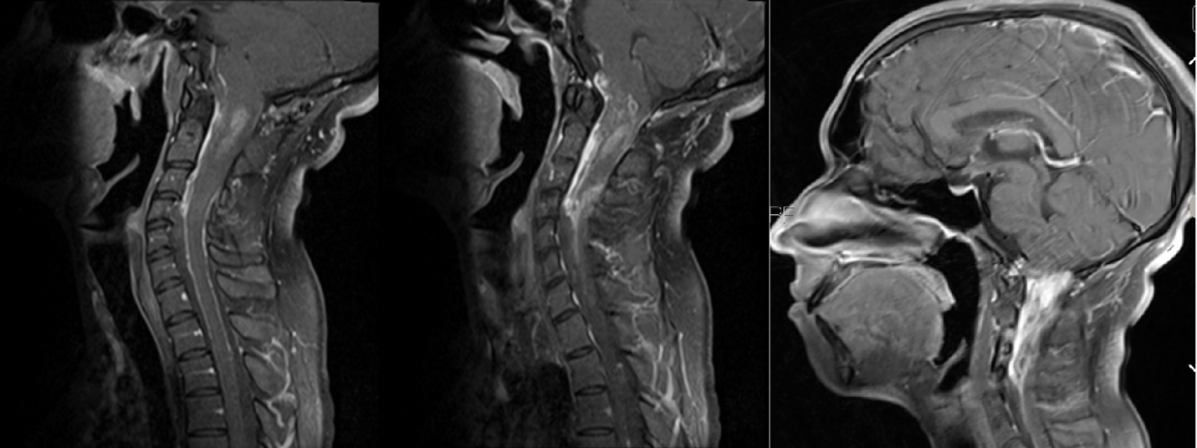
The patient was a 19-year-old male who presented to our clinic with a one-month history of progressive lower and upper extremities weakness and numbness with neck pain. The patient had a no past medical history and otherwise healthy. Physical examination revealed 4/5 strength in the lower and upper extremities. The patient had abnormalities in upper extremity strength and light sensation. He had no cranial nerve deficits, and mental status was normal. The patient was referred to our hospital for further evaluation and treatment. MRI of the cervical spine revealed an enhancing mass lesion at the C1-C4 Level with significant spinal cord compression (Figure 2). The lesion appeared to be arising from the spinal cord itself, with no significant extension into the surrounding tissues. Brain MRI revealed no mass lesion. Given the concerning imaging findings, the patient underwent a spinal cord tumor resection. A surgical procedure was carried out to perform a laminectomy of C1-C4 and debulk an intramedullary mass. As we observed during surgery total tumor resection was achieved.
Pathology
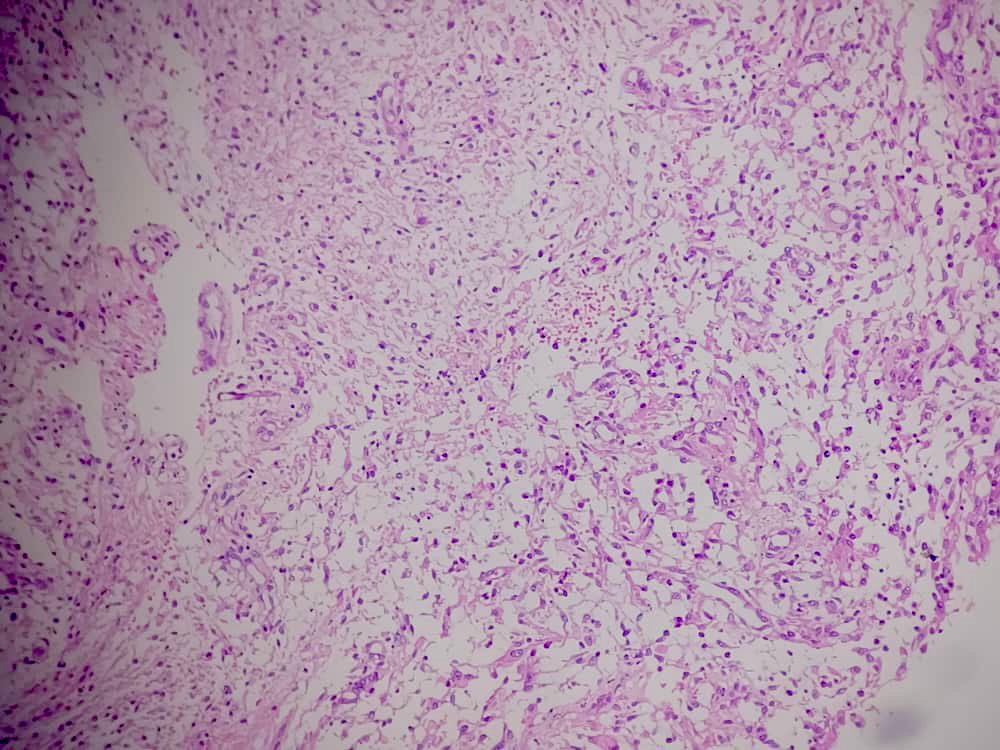
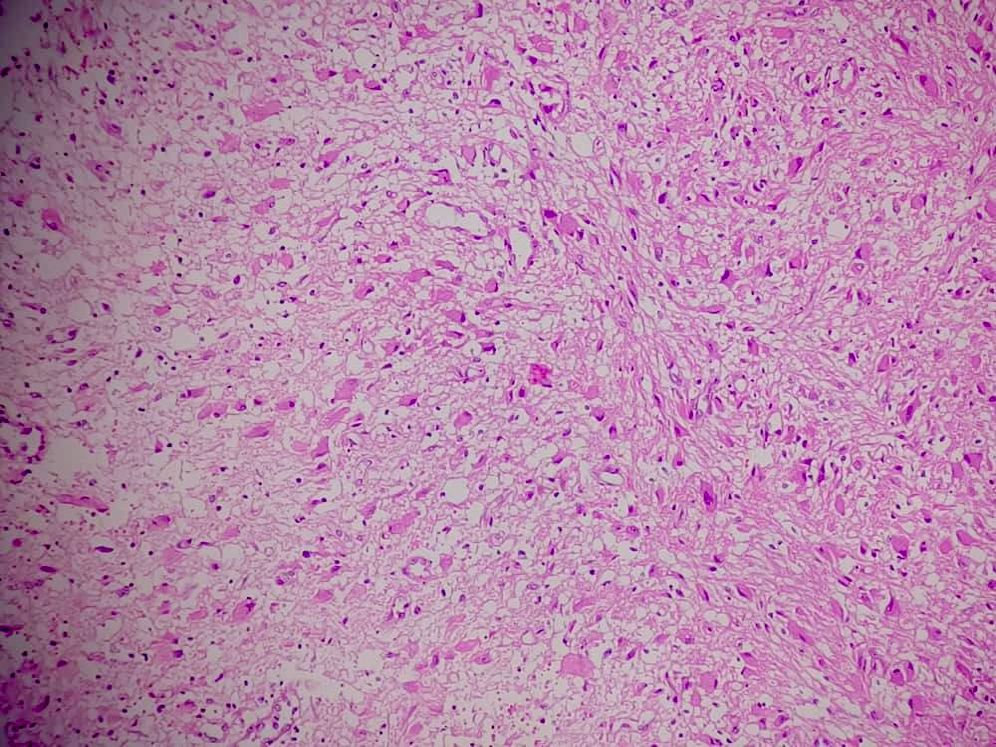
Both tumors specimens were referred to pathological assessment. Microscopic analysis of the biopsy showed the presence of neoplastic cells with vascular proliferation and focal necrosis when viewed under hematoxylin and eosin stains (Figures 3). Isocitrate dehydrogenase-1 (IDH1) was not detected upon immunohistochemical staining (Figure 4). These findings indicate the presence of giant cell glioblastoma, IDH wild-type, World Health Organization grade IV in the thoracic spinal cord. Genetic testing for mutant-type IDH1 was not performed on the tumor biopsies due to the negative IDH1 immunohistochemical staining.
Postoperative MRI showed significant improvement in spinal cord compression, with no evidence of residual tumor. The patient was then started on a course of radiation therapy and chemotherapy, consisting of temozolomide. He initially showed some improvement in neurological symptoms, with increased lower extremity strength and sensation.
Discussion
GBM in the spinal cord is a rare and challenging condition to manage. The clinical presentation can vary widely, with symptoms depending on the location and extent of the tumor [13]. In this case, the patient presented with lower extremity weakness and numbness, as well as bowel and bladder dysfunction, which are common symptoms of spinal cord compression.
Spinal cord tumors may arise within or near the spinal cord, categorized as either primary or metastatic, and situated intra-axially [14]. Primary spinal cord tumors account for a small percentage of all primary central nervous system tumors, with roughly one third situated in the intramedullary compartment [15]. Among adults, ependymoma is the most common intramedullary spinal cord tumor, typically presenting between the ages of 30 and 40. In children and young adults, intramedullary spinal cord tumors are less common, accounting for 1% to 10% of diagnosed central nervous system neoplasms [16]. Astrocytomas are the most common subtype among intramedullary spinal cord tumors in this age group [17].
Our patient, at the age of 19, was diagnosed with high- grade glioblastoma (GBM) after experiencing subacute back pain that progressed to neurological deficits such as urine retention and lower extremity motor weakness. The presentation of back pain in a young adult is rare, and a presentation of intramedullary giant cell GBM is even rarer.
Studies have shown that primary intracranial GBM has a relatively high incidence of spinal metastasis, indicating the need for spinal screening to detect early asymptomatic spinal metastasis [18]. However, intracranial metastasis from a spinal source is uncommon, with only a few reported cases of primary GBM spinal cord tumors exhibiting metastasis to the brain. MRI with T1- and T2-weighted sequences and/ or perfusion imaging can aid in identifying whether the neoplasm is a primary lesion or a secondary metastasis [19].
A review of the National Cancer Database revealed that primary spinal cord GBM had a greater mean survival of 11.2 months compared to primary cranial GBM, with a median survival age of 9.2 months [20]. Among patients aged 18 to 65, a longer survival time of 13.2 months was reported compared to patients younger than 18 and older than 65, who had survival times of 11.9 and 3.9 months, respectively. The reason for these differences remains unclear [21].
Upon further investigation of 95 patients with spinal cord GBM who received various treatments between 2004 and 2014, it was discovered that the survival rate was not significantly different among the five treatment options studied, including radiation with or without chemotherapy, surgery alone or with adjunct therapy, and palliative therapy [22]. However, the study did reveal that complete or partial resection of the spinal cord resulted in greater morbidity, and that GBMs are highly infiltrative malignancies. The study also found that overall survival was worse in patients under 18 years old compared to those between 18 and 65 years old, but the possibility of recurrence was not investigated. [23].
Due to the rarity of primary spinal cord GBM, there is limited information available about its management in the literature. No clinical trials have been conducted to date for the management of primary GBM spinal cord neoplasms [24]. Historically, spinal cord GBM has been treated similarly to intracranial GBM, with a combination of radiation therapy and temozolomide. Current management of these patients involves a multimodal approach of surgery, chemotherapy, and radiation therapy, which does not provide a cure for spinal cord GBM but has been shown to improve the overall quality of life for patients [25]. Diagnosis of GBM in the spinal cord is typically confirmed through imaging studies and biopsy. MRI is the preferred imaging modality for evaluating spinal cord tumors, as it provides detailed information about the location, size, and extent of the lesion. Biopsy is necessary to confirm the diagnosis and determine the grade of the tumor.
Nowadays, the standard treatment for spinal GBM usually involves surgery, radiotherapy, and sometimes chemotherapy. Although researchers have not found a significant link between radiation and prognosis, many people believe that radiation can increase survival time in malignant spinal tumors [26]. The optimal dosage of radiotherapy is uncertain, but it is almost always used. Shirato et al recommended that radiation can be given in 2.5- Gy fractions 4 times weekly to total doses of 40 to 50 Gy over 4 to 5 weeks [27]. In some cases, higher doses (59.4 Gy) may perform better in symptom improvement. However, total radiation dosage must be controlled to minimize adverse effects on growing and fertility, especially in teenagers [28].
Linsenmann T, et al. [29] 55-year-old woman who had a tumor in the cranio-cervical junction, causing compression of the medulla oblongata and resulting in hydrocephalus. Based on the radiological findings, a tentative diagnosis of meningioma was made. The tumor was removed through microsurgery and subsequent histopathological examination confirmed the presence of GBM WHO IV. The patient underwent percutaneous radiotherapy and received chemotherapy with temozolomide after the surgery. It is important to consider GBM in the differential diagnosis of cerebellar tumors [29]. The use of chemotherapy for spinal GBM remains controversial, but a retrospective series of 8 cases showed that both TMZ and bevacizumab were useful in improving survival. TMZ is generally used as adjuvant therapy to surgery and radiation in spinal GBM [30]. For patients with spinal GBM, it is recommended that TMZ be used concomitantly during and after radiotherapy, but at different dosages. In a study consisting of 6 patients, TMZ seemed to prolong survival time of primary spinal GBM [30]. However, both these patients revealed new intracranial lesions during follow-up. Chamberlain and Johnston found that bevacizumab may have some effects in those who failed to respond to radiation and TMZ therapy. Patients who received either adjuvant radiotherapy or chemotherapy had a better survival trend than those with surgery alone. Treatment for GBM in the spinal cord typically involves a combination of surgical resection, radiation therapy, and chemotherapy. However, the optimal management strategy remains unclear. Despite aggressive treatment, the prognosis for GBM in the spinal cord is generally poor, with a median survival time of less than two years. Possible future directions could include investigating novel targeted therapies, developing more efficient drug delivery methods to the spinal cord, and identifying genetic and molecular biomarkers that could help personalize treatment approaches. The development of animal models that accurately recapitulate the disease’s characteristics could also aid in preclinical studies, and clinical trials involving larger cohorts could help identify the most effective treatment strategies. These efforts could pave the way for improved outcomes and better quality of life for affected individuals.
Conclusion
GBM in the spinal cord is a rare and challenging condition that requires prompt diagnosis and management. Early detection and aggressive treatment can improve outcomes for affected individuals, but the prognosis remains poor. Primary glioblastoma multiforme (GBM) in the spinal cord is a rare type of spinal cord tumor. Just like primary cranial GBM, the available treatment options are limited to neurosurgery, radiation therapy, and chemotherapy. The effectiveness of treatment for primary cranial GBM cannot be assumed to be the same for primary spinal GBM. Hence, there is a need for further research and exploration to develop more effective therapies for GBM, especially for primary spinal GBM.
References
-
Shen CX, Wu JF, Zhao W, Cai ZW, Cai RZ, et al. (2017) Primary spinal glioblastoma multiforme: a case report and review of the literature. Medicine (Baltimore) 96: e6634.
-
Louis DN, Perry A, Reifenberger G, Deimling AV, Figarella-Branger, et al. (2016) The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol 131(6): 803-820.
-
Chamberlain MC, Johnston SK (2011) Recurrent spinal cord glioblastoma: salvage therapy with bevacizumab. J Neurooncol 102(3): 427-432.
-
Behmanesh B, Setzer M, Konczalla J, Harter P, Quick- Weller J, et al. (2017) Management of patients with primary intramedullary spinal cord glioblastoma. World Neurosurg 98: 198-202.
-
Hernández-Durán S, Bregy A, Shah AH, Hanft S, Komotar RJ, et al. (2015) Primary spinal cord glioblastoma multiforme treated with temozolomide. J Clin Neurosci 22(12): 1877-1882.
-
Chan KM, Fang D, Gan H, Hashizume R, Yu C, et al. (2013) The histone H3.3K27M mutation in pediatric glioma reprograms H3K27 methylation and gene expression. Genes Dev 27(9): 985-990.
-
Wan YCE, Liu J, Chan KM (2018) Histone H3 mutations in cancer. Curr Pharmacol Rep 4(4): 292-300.
-
Wu G, Broniscer A, McEachron TA, Lu C, Paugh BS, et al. (2012) Somatic histone H3 alterations in pediatric diffuse intrinsic pontine gliomas and non-brainstem glioblastomas. Nat Genet 44(3): 251-253.
-
Lu VM, Alvi MA, McDonald KL, Daniels DJ (2018) Impact of the H3K27M mutation on survival in pediatric high- grade glioma: a systematic review and meta-analysis. J Neurosurg Pediatr 23(3): 308-316.
-
Yi S, Choi S, Shin DA, Kim DS, Choi J, et al. (2019) Impact of H3.3 K27M mutation on prognosis and survival of grade IV spinal cord glioma on the basis of new 2016 World Health organization classification of the central nervous system. Neurosurgery 84(5): 1072-1081.
-
Daoud EV, Rajaram V, Cai C, Oberle RJ, Martin GR, et al. (2018) Adult brainstem gliomas with H3K27M mutation: radiology, pathology, and prognosis. J Neuropathol Exp Neurol 77(4): 302-311.
-
Buczkowicz P, Bartels U, Bouffet E (2014) Histopathological spectrum of paediatric diffuse intrinsic pontine glioma: diagnostic and therapeutic implications. Acta Neuropathol 128(4): 573-581.
-
Mattos JP, Marenco HA, Campos JM, Faria AV, Queiroz LS, et al. (2006) Cerebellar glioblastoma multiforme in an adult. Arquivos de neuro-psiquiatria 64: 132-135.
-
Williams MJ, Singleton WGB, Lowis SP, Malik K, Kurian KM (2017) Therapeutic targeting of histone modifications in adult and pediatric high-grade glioma. Front Oncol 7: 45.
-
Weller M, Gorlia T, Cairncross JG, Bent MJVD, Brandes AA, et al. (2011) Prolonged survival with valproic acid use in the EORTC/NCIC temozolomide trial for glioblastoma. Neurology 77(12): 1156-1164.
-
Tseng JH, Chen CY, Chen PC, Hsiao SH, Fan CC, et al. (2017) Valproic acid inhibits glioblastoma multiforme cell growth via paraoxonase 2 expression. Oncotarget 8(9): 14666-14679.
-
Orillac C, Thomas C, Dastagirzada Y, Hidalgo ET, Golfinos JG, et al. (2016) Pilocytic astrocytoma and glioneuronal tumor with histone H3 K27M mutation. Acta Neuropathol Commun 12(4): 84.
-
López G, Bush ONA, Berger MS, Perry A, Solomon DA ( 2017) Diffuse non-midline glioma with H3F3A K27M mutation: a prognostic and treatment dilemma. Acta Neuropathologica Communications 5(1): 38.
-
Pratt D, Natarajan SK, Banda A, Giannini C, Vats P, et al. (2018) Circumscribed/non-diffuse histology confers a better prognosis in H3K27M-mutant gliomas. Acta Neuropathol 135(2): 299-301.
-
Morais N, Mascarenhas L, Soares-Fernandes JP, Silva A, Magalhaes Z, et al. (2013) Primary spinal glioblastoma: a case report and review of the literature. Oncol Lett 5(3): 992-996.
-
Shen CX, Wu JF, Zhao W, CAi ZW, Chen CM, et al. (2017) Primary spinal glioblastoma multiforme. Medicine 96(16): e6634.
-
Timmons JJ, Zhang K, Fong J, Lok E, Swanson KD, et al. (2018) Literature review of spinal cord glioblastoma. Am J Clin Oncol 41(12): 1281-1287.
-
Louis DN, Perry A, Reifenberger G, Deimling AV, Dominique FB, et al. (2016) The 2016 World Health organization classification of tumors of the central nervous system: a summary. Acta Neuropathol 131(6): 803-820.
-
Onda K, Tanaka R, Takeda N (1986) Spinal metastases of cerebral glioblastoma: the value of computed tomographic metrizamide myelography in the diagnosis. Surg Neurol 25(4): 399-405.
-
Wolff B, Ng A, Roth D, Parthey K, Monika WM, et al. (2012) Pediatric high grade glioma of the spinal cord: results of the HIT-GBM database. J Neurooncol 107(1): 139-146.
-
Tendulkar RD, Pai PA, Wu S, Kun LE, Broniscer A, et al. (2010) Irradiation of pediatric high-grade spinal cord tumors. Int J Radiat Oncol Biol Phys 78(5): 1451-1456.
-
Ozgiray E, Akay A, Ertan Y, Cagli S, Oktar N, et al. (2013) Primary glioblastoma of the medulla spinalis: a report of three cases and review of the literature. Turk Neurosurg 23(6): 828-834.
-
Linsenmann T, Monoranu CM, Westermaier T, Varallyay C, Ernestus RI, et al. (2013) Exophytic glioblastoma arising from the cerebellum: case report and critical review of the literature. Journal of Neurological Surgery Part A: Central European Neurosurgery 74(4): 262-264.
-
Shirato H, Kamada T, Hida K, Koyanagi I, Iwasaki Y, et al. (1995) The role of radiotherapy in the management of spinal cord glioma. Int J Radiat Oncol Biol Phys 33(2): 323-328.
-
Kaley TJ, Mondesire-Crump I, Gavrilovic IT (2012) Temozolomide or bevacizumab for spinal cord high- grade gliomas. J Neurooncol 109(2): 385-389.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review