Surgical Management of Sudden Intrathoracic Hemorrhage in Two Patients with Occult Diaphragmatic Injury and Rib Fracture
Background: A sudden massive hemothorax as the initial manifestation of delayed diagnosis of blunt occult diaphragmatic injuries is extremely rare. We report our experience with two cases of sudden massive thoracic hemorrhage treated surgically for occult blunt diaphragm injury. In the present study, we aimed to present the successful rescue of two cases of sudden massive thoracic hemorrhage due to occult blunt diaphragmatic injury during hospitalization by surgical treatment. Sudden massive hemothorax a few days after hospitalization as an initial manifestation of blunt mysterious diaphragm injury is extremely rare.
Shouqiang Yu#*, Feng Liu#, Yonghui Quan* and Kunpeng Wu
#These authors have contributed equally to this work and share the first authorship
Background
A sudden massive hemothorax as the initial manifestation of delayed diagnosis of blunt occult diaphragmatic injuries is extremely rare. We report our experience with two cases of sudden massive thoracic hemorrhage treated surgically for occult blunt diaphragm injury.
Case 1 Presentation
A 49-year-old male was admitted to the hospital on 11 oct, 2010 due to “thoracoabdominal head trauma in a car accident for more than 1 hour”. There was a history of coma. Physical examination: blood pressure 57 / 30mmHg, psychic blurring. The right pupil was enlarged and approximately 5 mm in diameter with a loss of light reflex. The left chest wall collapsed, with a sense of bone friction, and the right chest wall had no sense of bone rub. Computed tomography examination suggested: bilateral multiple rib fractures, bilateral pneumothorax, pneumomediastinum, and double lung contusion. Admission diagnoses bilateral multiple rib fractures, bilateral hemopneumothorax, double lung contusion, hemorrhagic shock, and head injury. After admission, fluid replacement, blood transfusion, breathing with ventilator support, and closed chest drainage were placed at the second intercostal space in the midclavicular line bilaterally. The right thoracic cavity can have bubble overflow, with no liquid drainage out. The left thoracic drain drained hemorrhagic fluid about 450 ml per day. The patient has been hemodynamically unstable. A review chest CT on 12 OCT 2010 suggested a large amount of effusion in the right thoracic cavity. An additional lower right thoracic closed drain was placed, at that time approximately 300 ml of anticoagulant fluid was drained and 750 mL of bloody fluid was drained the following day. The neurosurgeon performed a right temporal bone debonding flap, then performed a right external dural hematoma evacuation and gave a tracheostomy. On 14 Oct 2010 07:00 am to 10:00 am, the patient elicited blood fluid of about 1500ml from the right thoracic closed drainage tube. An open chest exploration was immediately given, and about an additional 1500 ml of blood from the right chest was aspirated during the operation, and about 1500 g of the blood clot was covered on the surface of the right diaphragm, which was cleared. A full-thickness laceration wound measuring approximately 6.5 cm was located on the upper end of the right diaphragm with a small artery stump and active bleeding. Electrocoagulation was given to stop bleeding and the diaphragm was repaired with a number 7 silk suture. Intraoperative transfusion of red suspension 4.5 u and plasma 220 ml. Postoperatively the patient had central diabetes insipidus due to a traumatic head injury which improved after symptomatic treatment was given. The patient was discharged from the hospital uneventfully on 09 Nov 2010.
Case 2 Presentation
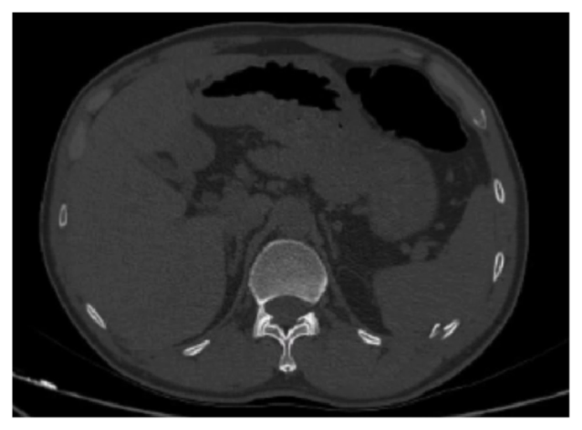
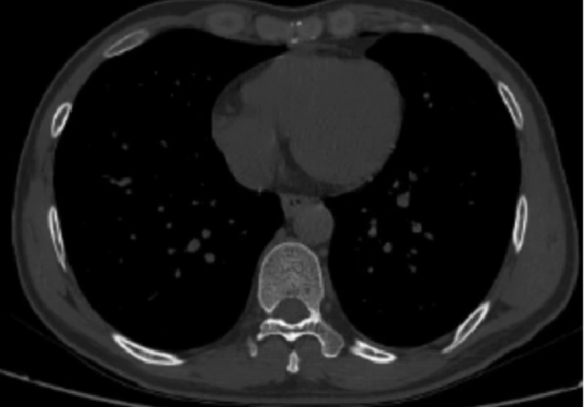
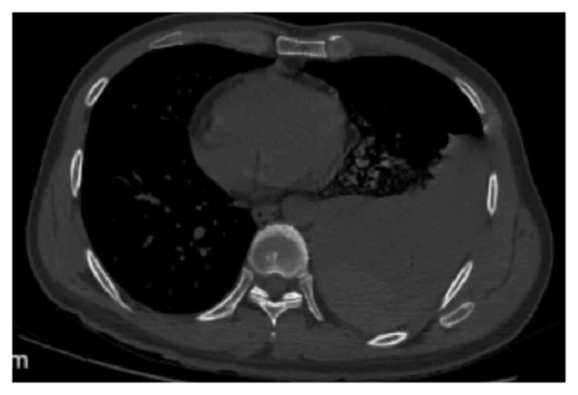
A male, 42 years old, was admitted to our hospital due to “pain in the left chest and left elbow caused by falling down into a 0.5 m deep pit by stepping on inverting Transwell cap for 17 hours “on 14 October 2021. Physical examination on admission: blood pressure 112 / 76mmhg, left chest wall tenderness. About 10cm * 10cm skin ecchymosis was seen on the left side of the abdomen (Figure 1). Skin abrasions were seen over the left elbow joint. Admission thoracoabdominal computed tomography showed a rib fracture visible posterior to the left hemidiaphragm but no diameter sign of diaphragm injury also no left pleural effusion visible (Figures 2 & 3). On 16 OCT 2021 15:17 excluded thoracic spine fracture CT scan tips: fracture of left two ribs and left pleural small amount of effusion. On 17 OCT 2021 at 09:00 am, the patient went to the toilet fainting in the bathroom, blood pressure was measured 60 / 45mmhg, thoracic CT scan suggested a large left pleural effusion (Figure 4). After giving rehydration and blood preparation, at the same time, the family signed informed consent, then immediately under anesthesia, the left thoracoscopic exploration was applied, the left thoracic blood accumulation was removed about 1200 ml, and the left posterior costophrenic angle was cleared about 300 g of the blood clot, then the diaphragm at the site of the left costophrenic angle has a long about 2.0 cm non-full-thickness tear, the muscle is bleeding, and 3-0 Prolene suture was given to stop bleeding. Postoperatively the patient recovered uneventfully and was discharged on the 10th postoperative day.

Discussion
There were two patients in this report, one due to a high- energy car accident resulting in occult diaphragm injury, multiple rib fractures, and severe head injury, and the other due to a low-energy fall resulting in two left rib fractures, with no obvious hemothorax on admission, no intra-abdominal visceral herniation into the thoracic cavity on imaging, and occult diaphragm injury was not easily diagnosed. Until more than 72 h of admission with diaphragmatic hemorrhage causing shock and massive thoracic hemorrhage treated by open or thoracoscopic surgery, it was clear that the massive thoracic hemorrhage originated from occult diaphragmatic injury and diaphragm repair was performed with satisfactory results [1].
A study from Stockholm, Sweden reported that chest trauma accounted for 32% (768 / 2397), blunt injury accounted for 83% (634 / 768), sharp injury accounted for 17% (134 / 768), and chest injury was an independent risk factor for mortality within 30 days after injury. In that study, rib fractures accounted for 57% (343 / 768) and hemothorax for 23% (174 / 768), while in that study, whether or not there was combined diaphragm injury was not reported [2]. There is the potential for diaphragmatic injury from either high - or low-energy trauma [3, 4]. Diaphragm injury is rare (<1%) following blunt trauma, whereas penetrating thoracoabdominal trauma has an incidence of 24% to 38% [5]. And, diaphragmatic injuries accounted for 4.06% (23 / 566) of rib fractures [1]. Most traumatic diaphragm injuries are identified through surgical exploration. The overall accuracy of the chest X-ray or CT is quite poor and unreliable [5, 6]. The only direct sign of diaphragmatic injury is the visualization of herniated abdominal viscera into the chest [7]. Turhan K, et al. [8] reported the first traumatic septal hernia in the world [8]. Repair of the acutely blunt-injured diaphragm is best performed via laparotomy, although the laparoscopic or thoracoscopic repair is feasible [5].
Diaphragmatic injury resulting in sudden massive thoracic hemorrhage is as life-threatening and more urgent than acute septal hernia resulting in herniation of abdominal organs into the thorax causing incarceration of abdominal organs [9]. Hemostasis by repair within 24 h of thoracic open hemorrhage or aortic rupture was diagnosed in 8.3% (5/60) of cases, while the literature of sudden massive hemorrhage in the thorax caused by diaphragm injury was rare [10], especially when the patient was admitted more than 72 h. Preparation was insufficient, and emergency rescue was slightly passive, under these circumstances, which should be paid more attention to [11]. Delayed emergent thoracic major hemorrhage due to diaphragm injury especially when the diaphragm is incompletely lacerated on one side of the thoracic cavity, hemostasis and repair by the transthoracic route are only possible, video thoracoscopic hemostasis and repair when the condition permits [12, 13].
Conclusion
A sudden diaphragmatic active bleeding resulting in hemothorax may be the initial presentation of occult diaphragmatic injury with rib fractures. Even if the patient is admitted without any clinical signs of diaphragmatic injury, occult injury to the diaphragm and later sudden onset of intrathoracic massive hemorrhage should be anticipated. On admission, blood preparation is required, and patients are asked not to be discharged within a week, to keep their stools normal, and once patients experience syncope or hypotension, bedside chest radiographs or CT suggest pleural effusion, rehydration, timely blood transfusion, and other necessary anti-shock treatment measures should be given immediately. Meanwhile, emergency thoracotomy can clarify the diagnosis of occult diaphragmatic injury, and in turn, the diaphragm can be repaired for hemostasis, resulting in satisfactory therapeutic outcomes.
Acknowledgments
Not applicable.
Authors’ Contributions
Shouqiang Yu collected the data of the patient, consulted literature, and wrote the manuscript; Feng Liu edited the manuscript and dealt with the Figures. Yonghui Quan also gave useful suggestions on writing and improved the manuscript. Kunpeng Wu was the consultant in charge of the case, established the diagnosis, and approved the submitted version. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
This study was approved by the ethics committee of the Lishui branch of Zhongda Hospital Affiliated to Southeast University, Nanjing 211200, China, with approval number (2021sq15). The publication of this article was exempt from the patient’s signing of written informed consent, as approved by the hospital ethics committee.
Data Availability Statement
The datasets used and analyzed in the current study are available from the corresponding author on demand.
References
-
Powell L, Chai J, Shaikh A, Shaikh A (2019) Experience with acute diaphragmatic trauma and multiple rib fractures using routine thoracoscopy. J Thorac Dis 11(S8): S1024-S1028.
-
Lundin A, Akram SK, Berg L, Göransson KE, Enocson A (2022) Thoracic injuries in trauma patients: epidemiology and its influence on mortality. Scand J Trauma Resusc Emerg Med 30(1): 69.
-
Wemeijer TM, Hogeboom W, Steenvoorde P, Withaar DS, Groot RD (2022) Missed injuries in trauma patients: the value of a diagnostic thoracotomy or thoracoscopy during surgical stabilisation of rib fractures. Ir J Med Sci 191(3): 1285-1289.
-
Al-Kahwa AA, Lauritzen JB (2015) Blunt diaphragmatic rupture following low-energy trauma. Ugeskr Laeger 177(8): V11140590.
-
Biffl WL, Cioffi WG (2021) Diaphragm. In: Feliciano DV, Mattox KL, Moore EE, (Eds.), TRAUMA. New York McGraw Hill.
-
Shapiro MJ, Heiberg E, Durham RM, Luchtefeld W, Mazuski JE (1996) The unreliability of CT scans and initial chest radiographs in evaluating blunt trauma induced diaphragmatic rupture. Clin Radiol 51(1): 27- 30.
-
Kozak O, Mentes O, Harlak A, Yigit T, Kilbas Z, et al. (2008) Late presentation of blunt right diaphragmatic rupture (hepatic hernia). Am J Emerg Med 26(5): 638e3-638e5.
-
Turhan K, Makay O, Cakan A, Samancilar O, Firat O, et al. (2008) Traumatic diaphragmatic rupture: look to see. Eur J Cardiothorac Surg 33(6): 1082-1085.
-
Karangelis D, Karkos C, Tagarakis G, Papadopoulos D, Tsilimingaset N, et al. (2011) Traumatic diaphragmatic rupture: a silent killer. Am Surg 77(3): E55-E56.
-
Muronoi T, Kidani A, Oka K, Konishi M, Kuramoto S, et al. (2020) Delayed massive hemothorax due to diaphragm injury with rib fracture: A case report. Int J Surg Case Rep 77: 133-137.
-
Rodriguez-Morales G, Rodriguez A, Shatney CH (1986) Acute rupture of the diaphragm in blunt trauma: analysis of 60 patients. J Trauma 26(5): 438-444.
-
Yokosuka T, Kobayashi T, Fujiogi M, Nakano T, Shirokawa M, et al. (2014) Clinical analysis of delayed hemothorax due to diaphragmatic injury treated by emergent video- assisted thoracic surgery. Kyobu Geka 67(11): 954-958.
-
Park CH, Kim KE, Chae MC, Lee JW (2022) Delayed massive hemothorax after blunt thoracic trauma requiring thoracotomy by VATS: a case report. J Surg Case Rep 2022(1): rjab537.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review