Are Nodular Goiter Patients Previously Treated with L-Thyroxine have Unfavorable Outcomes after Surgery Compared to Patients without Medical Treatment?
This systematic review aimed to analyze the literature on PubMed Database regarding studies which compare the patient’s post-thyroidectomy outcomes, between those who were treated with L-Thyroxine prior to surgery and those who underwent to thyroidectomy without hormonal suppressive therapy. 500 articles were screened, 11 articles were selected, which were related to the outcomes of interests. Among all these articles with outcome interests, no article is appropriate to the research question of our investigation. The outcomes of surgical treatment of nodular goiter patients, depending on using L-Thyroxine treatment in anamnesis, are very interesting and could bring light to some issues of endocrinology. There is need for further research on this topic to generate relevant evidence on use of L-Thyroxine.
Introduction
Benign thyroid nodules are one of the most common pathologies among the population and the incidence is significantly higher in the areas with iodine deficit. Different sources report a wide range of thyroid nodules prevalence from 10% up to 69% [1]. Levothyroxine treatment is widely used for diminishing nodule and gland sizes [2]. However, in the American Thyroid Association Guidelines Task Force on Thyroid Nodules, hormonal suppression therapy with L-Thyroxine for benign thyroid nodules in patients who live in iodine-sufficient areas is not recommended [3]. A variety of treatment procedures has been suggested for the treatment of nodular disease of the thyroid gland [4]. Due to the fact that the malignancy rate is about 5% among benign thyroid nodules, all patients treated with minimally invasive procedures need serious follow-up with regularly fine-needle aspiration biopsies [5]. So, traditional surgical procedures like total or subtotal thyroidectomies are the dominant treatment method in patients with nodular goiter.
The recent literature review shows the controversial outcomes about the effectiveness of hormonal suppressive therapy with L-thyroxine in the treatment of nodular goiter. Patients with insufficient results after hormonal suppressive therapy have to undergo surgeries [2]. Moreover, L-Thyroxine has an adverse negative effect on bone mineral density [6] and increases the rate of cardiac arrhythmias in patients who are treated for a long time [7].
The aim of this study was systematically analyzing of literature on PubMed Database regarding studies which compare the patient’s post-thyroidectomy outcomes, between those who were treated with L-Thyroxine prior to surgery and those who underwent to thyroidectomy without hormonal suppressive therapy.
Methods
Study Design: Systematic review Eligibility Criteria Key questions are commonly formulated according to the “PICO” method, the details of which are presented below. Population: Adult patients with benign thyroid nodules. Intervention/Exposure: L-Thyroxin or hormonal suppressive therapy Comparator/Control: Non-treated patients with L-Thyroxin Outcome: Unfavorable outcomes (hepatocytes dysfunction, lipid profile changes with a high risk of cardiovascular diseases, worsened quality of life) Search Strategy: We searched published articles on the PubMed database without language restrictions. We used the below restrictions while searching for the articles,
- Inclusion Criteria: Clinical Trial, Meta-Analysis, Randomized Controlled Trial, Review, Systematic Review
- Exclusion Criteria: Books and Documents, case reports.
- Time Frame: Data published from 2012 till 2022 years.
We searched for articles based on PICO format. #1 Selection of Articles Related to Study Population: To select all the articles related to thyroid nodules, we used the below search strategy. Thyroid, nodule [MeSH] OR Thyroid nodules [MeSH] OR Goiter, Nodular [MeSH] OR Nodular Goiter [tiab] OR Nodular Goiters [tiab] #2 Selection of Article Related to Exposure: To select all the articles related to hormonal therapy with L-thyroxine, we used the below search strategy L thyroxine [MeSH] OR Thyroxine [MeSH] OR Thyroxin [tiab] OR Thyroid Hormone [tiab] OR L-thyroxine [tiab] OR Tetraiodothyronine [tiab] OR Levothyroxine [tiab] OR Levothroid [tiab] OR Levoxine [tiab] OR Levoxyl [tiab] OR Lévothyrox [tiab] OR Novothyral [tiab] OR Novothyrox [tiab] OR Oroxine [tiab] OR Levothroid [tiab] OR Levoxine [tiab] OR Levoxyl [tiab] OR Lévothyrox [tiab] OR Novothyral [tiab] OR Novothyrox [tiab] OR Oroxine [tiab] OR levothyroxine sodium [tiab] OR Euthyrox [MeSH] OR L-Thyrox* [tiab] OR Levothyroxine [MeSH] OR Levothyrox*[tiab] OR L-Thyrox*[tiab] OR Levo-T [tiab] OR Eutirox [tiab] #3 Selection of Articles Related to Thyroidectomy: Thyroidectomy [MeSH] OR thyroidectomies [MeSH) #4 Selection of articles related to outcomes of surgery: Treatment outcome [MeSH] OR treatment outcome* [tiab] OR Patient-Relevant Outcome OR Outcomes, Patient-Relevant [tiab] OR Clinical Effectiveness [MeSH] OR Treatment Effectiveness [tiab] OR Outcome, Rehabilitation [MeSH] OR Treatment Efficacy [tiab] OR Clinical Efficacy [MeSH] OR recurrence [MeSH] OR recurrence*[tiab] OR relapse*[tiab] or Quality of life [tiab] Final search strategy: We combined all the above to create a composite search strategy #1 AND #2 AND #3 AND #4
Results
Screening of Articles
The initial search results obtained the 524 articles. During the screening process 24 articles were excluded. Exclusion reasons were case reports and articles without an abstract.
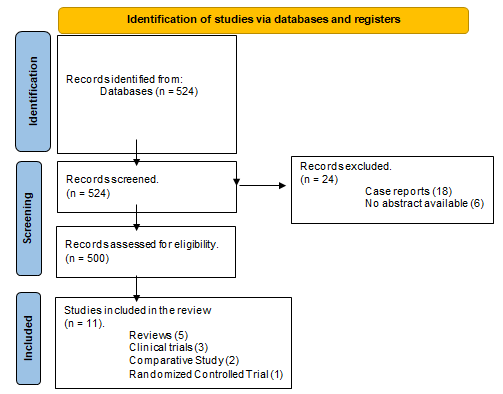
500 articles were systematized in Excel sheet. The selection of articles regarding publishing date and article types were shown in Tables 1 & 2 accordingly.
11 articles were selected, which were related to the outcomes of interests. Table 3 shows the characteristics of related articles.
| Years | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total n=500 | 13 | 55 | 55 | 55 | 48 | 51 | 45 | 63 | 51 | 62 | 2 |
Table 2: Selection results for publishing date.
| Types | Number |
|---|---|
| Clinical trial | 107 |
| Comparative Study | 15 |
| Meta-Analysis | 42 |
| Observational Study | 6 |
| Retrospective Study | 19 |
| Prospective study | 2 |
| Randomized Controlled Trial | 72 |
| Review | 228 |
| Systematic Review and Meta-analysis | 3 |
Table 1: Selection for articles type.
| Country | Article type | Outcomes | |
|---|---|---|---|
| Sjölin G, et al. [8] | Sweden | Clinical Trial | This study discusses the long-term total outcome of antithyroid drug or J131 or surgical treatment modality regarding how many require levothyroxine supplementation, the need for thyroid ablation, or the individual patient’s estimation of their recovery. |
| Tiedje V, et al. [9] | Germany | Review | This review talks about the treatment of differentiated thyroid cancer. Continued TSH suppressive levothyroxine therapy is only recommended in high-risk patients. |
| Brun VH, et al. [10] | Norway, Sweden. | Randomized Controlled Trial | This study is about the levothyroxine (LT4) replacement therapy dosage adjustment with a decision aid tool (DAT) that models LT4 pharmacometrics and enables patient-tailored dosage after total thyroidectomy. |
| Gambale C, et al. [11] | Italy | Review | The review talks about the treatment of differentiated thyroid cancer (DTC). L-T4 therapy should be personalized according to the type of surgery, the age of patients, and their comorbidities. |
| Buehler LA, et al. [12] | USA | Comparative Study | This study aimed to assess hormonal outcomes and thyroid hormone (TH) replacement after hemithyroidectomy (HT). |
| Antonelli A, et al. [13] | Italy, USA | Review | In the twelve papers that constitute this Research Topic, various innovative aspects related to therapy of hypothyroidism with L-T4 are reviewed and discussed and provide a stimulating overview of the present state of our knowledge |
| Gluvic Z, et al. [7] | Serbia, The United Kingdom, Saudi Arabia | Review | This review summarizes the relevant available data related to LT4 suppressive treatment and the associated risk of cardiac arrhythmia. |
| Leenhardt L, et al. [14] | France | Comparative Study | This study demonstrates the noninferiority of rhTSH vs thyroid hormone withdrawal (THW) in preparation for RAI regarding disease status at the first evaluation in the real-life setting in patients with N1 DTC. |
| Shin YW, et al. [15] | South Korea, USA | Clinical trial | The study examined whether thyroid hormone withdrawal affects resting state functional connectivity and the mood or QoL of the patients with thyroid hormone withdrawal status. |
| Moon JH, et al. [16] | South Korea, | Clinical trial | The association between serum thyroid hormone concentration and cognitive function was investigated. |
| Medas F, et al. [17] | Italy | Review | This review compared pathological features and surgical outcomes of hyperthyroid versus euthyroid patients. |
Table 3: Characteristics of 11 included articles on L-Thyroxine treatment in patients with thyroid diseases.
Among all these articles with outcome interests, no article is appropriate to the research question of our investigation. Most articles present the outcomes of the L-Thyroxine therapy after surgery. However, the main aim of our study was the compare the outcomes of the L-Thyroxine therapy before thyroidectomy.
Discussion
Nodular goiter is the most common disease of the thyroid gland with a prevalence of 5-7%, increasing up to 70% among the population of endemic zones [18]. Ultrasound investigation, fine needle biopsy, hormonal analysis of blood, radioisotope scintigraphy, and computer tomography are the main methods in the diagnosis of thyroid nodules [5]. Fine needle biopsy of small nodules detected by USM reveals tumor cells or undifferentiated cytological structures in up to 12% of cases [19]. Among patients with negative needle biopsy results, malignant transformation is recorded in 10- 20%. After surgeries regarding suspicious nodules, thyroid cancer is identified in 8.5% - 10% of pathomorphological evaluation of the removed gland tissue [20].
Depending on the size of the nodule and the results of fine-needle aspiration biopsy, there are 4 main approaches to the treatment of nodular disease: clinical observation, hormonal suppressive treatment with L-Thyroxin, treatment with Radioactive J131 and surgical procedure [1]. Hormonal suppressive treatment with L-Thyroxine recommended in small-sized nodules. However, the effectiveness of hormonal treatment with L-Thyroxin in reducing the size of nodes and glands is controversial. In addition, L-Thyroxine, has adverse effects on cardiac function and changes bone mineral composition [21, 22, 23]. Moreover, levothyroxine therapy for a long time, has a risk of losing time in cases of tumor transformation of nodules [24].
Long-term levothyroxine treatment costs a lot of money and loaded the health resources. L-Thyroxine therapy in most cases shows not effective outcomes regarding the decreasing nodule size, and most patients must be undergone to surgical procedures, which causes a violation of the patients’ quality of life [25].
Liver is responsible for the metabolism of the thyroid hormones and long-term levothyroxine intake negatively influences the hepatocytes. This may result in the insufficient outcomes of the replacement hormone therapy after surgery and lead to increased dosage [26, 27].
We tried to compare the literature dedicated to the outcomes of the patients with nodular goiter, who previously treated with levothyroxine for a long time and those who underwent to thyroidectomy without hormonal suppressive therapy. Unfortunately, there was no article with outcomes of studies regarding our research question.
Conclusion
Thyroid nodules smaller than 1 cm were treated with L-Thyroxine, with so-called hormonal suppressive treatment. The effectiveness of hormonal suppressive treatment is disputed in publications. Among some effects on decreasing the nodule size, L-Thyroxine has adverse effects such as a negative influence on the bone mineral density and an increase in the cardiovascular diseases risk.
Patients, with nodular goiter, should be differentiated regarding the use of hormonal suppressive therapy. The outcomes of surgical treatment of nodular goiter patients, depending on using L-Thyroxine treatment in anamnesis, are very interesting and could bring light to some issues of endocrinology. Unfortunately, literature research in PubMed and analyses of all screened articles shows that, there aren’t any articles in the context of the impact of L-Thyroxine therapy on surgical management outcomes. There is need for further research on this topic to generate relevant evidence on use of L-Thyroxine.
Conflict of Interest
Authors declare no conflict of interest.
Sources of Financial Support
The study did not have sponsorship.
References
-
Unlu MT, Kostek M, Aygun N, Isgor A, Uludag M (2022) Non-Toxic Multinodular Goiter: From Etiopathogenesis to Treatment. Sisli Etfal Hastan Tip Bul 56(1): 21-40.
-
Bandeira‐Echtler E, Bergerhoff K, Richter B (2014) Levothyroxine or minimally invasive therapies for benign thyroid nodules. Cochrane Database Syst Rev CD004098.
-
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, et al. (2016) 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 26(1): 1-133.
-
Baldwin CK, Natter MB, Patel KN, Hodak SP (2022) Minimally Invasive Techniques for the Management of Thyroid Nodules. Endocrinol Metab Clin North Am 51(2): 323-349.
-
Durante C, Grani G, Lamartina L, Filetti S, Mandel SJ, et al. (2018) The Diagnosis and Management of Thyroid Nodules: A Review. JAMA 319(9): 914-924.
-
Schneider R, Schneider M, Reiners C, Schneider P (2012) Effects of levothyroxine on bone mineral density, muscle force, and bone turnover markers: a cohort study. J Clin Endocrinol Metab 97(11): 3926-3934.
-
Gluvic Z, Obradovic M, Stewart AJ, Essack M, Pitt SJ, et al. (2021) Levothyroxine Treatment and the Risk of Cardiac Arrhythmias - Focus on the Patient Submitted to Thyroid Surgery. Front Endocrinol (Lausanne) 12: 758043.
-
Sjölin G, Holmberg M, Törring O, Byström K, Khamisi S, et al. (2019) The Long-Term Outcome of Treatment for Graves’ Hyperthyroidism. Thyroid 29(11): 1545-1557.
-
Tiedje V, Schmid KW, Weber F, Bockisch A, Führer D (2015) Differentiated thyroid cancer. Der Internist 56: 153-166.
-
Brun VH, Eriksen AH, Selseth R, Johansson K, Vik R, et al. (2021) Patient-Tailored Levothyroxine Dosage with Pharmacokinetic/Pharmacodynamic Modeling: A Novel Approach After Total Thyroidectomy. Thyroid 31(9): 1297-1304.
-
Gambale C, Elisei R, Matrone A (2020) Management and follow-up of differentiated thyroid cancer not submitted to radioiodine treatment: a systematic review. Minerva Endocrinol 45(4): 306-317.
-
Buehler LA, Madhun NZ, Bena J, Nasr C, Scharpf J, et al. (2021) Hormonal Outcomes Following Hemithyroidectomy. Otolaryngol Head Neck Surg 164(5): 1011-1018.
-
Antonelli A, Wartofsky L, Miccoli P (2021) Editorial: Levothyroxine Therapy in Patients With Hypothyroidism. Front Endocrinol 12: 734895.
-
Leenhardt L, Leboulleux S, Bournaud C, Zerdoud S, Schvartz C, et al. (2019) Recombinant Thyrotropin vs Levothyroxine Withdrawal in 131I Therapy of N1 Thyroid Cancer: A Large Matched Cohort Study (ThyrNod). J Clin Endocrinol Metab 104: 1020-1028.
-
Shin YW, Choi YM, Kim HS, Kim DJ, Jo HJ, et al. (2016) Diminished Quality of Life and Increased Brain Functional Connectivity in Patients with Hypothyroidism After Total Thyroidectomy. Thyroid 26(5): 641-649.
-
Moon JH, Hyun MK, Lee JY, Shim JI, Kim TH, et al. (2018) Prevalence of thyroid nodules and their associated clinical parameters: a large-scale, multicenter-based health checkup study. Korean J Intern Med 33(4): 753- 762.
-
Medas F, Tuveri M, Canu GL, Erdas E, Calò PG (2019) Complications after reoperative thyroid surgery: retrospective evaluation of 152 consecutive cases. Updates Surg 71: 705-710.
-
Iwata AJ, Bhan A, Lahiri S, Williams AM, Taylor AR, et al. (2018) Comparison of incidental versus palpable thyroid nodules presenting for fine-needle aspiration biopsy. Head & Neck 40(7): 1508-1514.
-
Yalcin M, Altinova AE, Ozkan C, Toruner F, Akturk M, et al. (2016) Thyroid Malignancy Risk of Incidental Thyroid Nodules in Patients with Non-Thyroid Cancer. Acta Endo (Buc) 12(2): 185-190.
-
Rosario PW, Silva AL, Calsolari MR (2017) Is fine needle aspiration really not necessary in patients with thyroid nodules ≤ 1 cm with highly suspicious features on ultrasonography and candidates for active surveillance? FNA and Active Surveillance. Diagn Cytopathol 45(4): 294-296.
-
Effraimidis G, Watt T, Feldt Rasmussen U (2021) Levothyroxine Therapy in Elderly Patients with Hypothyroidism. Front Endocrinol 12: 641560.
-
Flynn RW, Bonellie SR, Jung RT, MacDonald TM, Morris AD, et al. (2010) Serum Thyroid-Stimulating Hormone Concentration and Morbidity from Cardiovascular Disease and Fractures in Patients on Long-Term Thyroxine Therapy. The Journal of Clinical Endocrinology & Metabolism 95(1): 186-193.
-
Ochani S, Siddiqui A, Adnan A (2022) Adverse effects of long-term Levothyroxine therapy in Subclinical Hypothyroidism. Annals of Medicine and Surgery 76: 103503.
-
Knobel M (2016) Which Is the Ideal Treatment for Benign Diffuse and Multinodular Non-Toxic Goiters?. Front Endocrinol 7.
-
Qian J, Tanni KA (2021) Real world evidence in effectiveness, safety, and cost savings of generic levothyroxine: a systematic review. Endocrine 74: 228- 234.
-
Wilder VN, Bravenboer B, Herremans S, Vanderbruggen N, Velkeniers B (2017) Pseudomalabsorption of Levothyroxine: A Challenge for the Endocrinologist in the Treatment of Hypothyroidism. Eur Thyroid J 6(1): 52-56.
-
Russ G (2016) Risk stratification of thyroid nodules on ultrasonography with the French TI-RADS: description and reflections. Ultrasonography 35(1): 25-38.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review