Igg4 Pseudo tumors Mimicking Urologic Malignancies: Comprehensive Review and Management of a Rare Infiltrative Upper Tract Lesion
Objectives: Immune-mediated fibroinflammatory conditions are known to affect multiple organ systems, as seen in the IgG-4 related disease. While tubulointerstitial nephritis and membranous glomerulonephritis are the more common intrinsic renal diseases, IgG-4 mediated disease can mimick urologic malignancies and can pose a significant management dilemma. Our goal is to understand how to better diagnose, exclude malignancy, and preserve renal function in a rare Urologic disease. Materials and Methods: A review of current literature was obtained to provide additional insight and understanding on this rarely observed Urologic disease. In discussing the case presented, a pertinent clinical history, physical exam, and review of cross-sectional imaging is presented. Immunohistochemical analysis of the specimen was thoroughly performed with expert analysis by our consulting pathologist. Results: Very rare reports of renal, ureteral, pelvic, or scrotal IgG4 mediated pseudotumors have been published. In the absence of pathologic tissue analysis of biopsy samples, the diagnosis of this rare disease can be significantly challenging. In our presentation, a male patient was noted to have a 7cm mass replacing the left renal sinus and causing moderate left hydronephrosis. Initial concern was for upper tract urothelial cell carcinoma. However, left ureteropyeloscopy demonstrated normal left renal and ureteral architecture and excisional biopsy of a PET avid left cervical lymph node was performed however pathologic diagnosis was not able to be confirmed. This led to a management dilemma due to the progressing mass size, worsening renal drainage, and symptoms. The patient opted for surgical excision. Final pathology from a left radical nephrectomy was significant for an IgG-4 related inflammatory pseudotumor. Conclusions: IgG-4 related diseases are known to represent a systemic disease that leads to lymphoplasmacystic inflammation and fibrosis within the affected tissues. At this time, there is no standardized method for the diagnosis and treatment of patients with retroperitoneal involvement. Additional research is needed to identify improved diagnostic modalities, the role of immunosuppressive therapy, and the surgical management in this disease process.
Introduction
Immune-mediated fibroinflammatory conditions are known to affect multiple organ systems, as seen in the IgG4 related diseases. Although the exact pathogenesis remains incompletely characterized, it is clear T cells play an important role, and that IgG4 antibodies themselves are not pathogenic. Furthermore, while affected tissues histologically show dense lymphoplasmacytic infiltrates with a predominance of IgG4 positive plasma cells, there are no characteristic imaging findings [1]. Many patients will be asymptomatic, but some can present with flank or abdominal pain, hematuria, or other constitutional symptoms. Since the imaging features are nonspecific, it is difficult to reliably distinguish between IgG4-related disease and cancers [2]. To that end, IgG4 related disease poses a diagnostic dilemma as it can mimic malignancies throughout the body which highlights the importance of awareness for this disease entity. For example, many patients with IgG4- related renal disease will have concomitant extrarenal lesions to include retroperitoneal fibrosis which can be quite difficult to diagnose and manage [3]. As such, we present a case of an IgG4-related inflammatory pseudotumor encasing the left renal pelvis that was incidentally noted on surveillance abdominal imaging for a pancreatic cyst. In addition to presenting a unique case, IgG4-related diseases that mimicked urologic malignancies are also discussed.
Presentation
Clinical History
A 66-year-old male was referred for urologic evaluation of an incidentally found left renal collecting system mass noted on magnetic resonance imaging (MRI) of his abdomen for surveillance of a benign appearing pancreatic cyst. This MRI noted a new 7 x 3.8 x 3.8cm infiltrating hypoenhancing mass replacing the left renal sinus and extending along the proximal left ureter causing moderate left hydronephrosis concerning for urothelial cell carcinoma. A subsequent computed tomography intravenous pyelogram (CT IVP) demonstrated a slightly enhancing left renal mass and delayed imaging illustrated filling defects in the left renal collecting system (Figures 1 & 2). At his office visit, he endorsed mild left flank pain. He denied any other urologic symptoms, including hematuria. Social and family history was remarkable for a 12 pack-year smoking history and no family history of renal failure or malignancy. Physical exam was unremarkable. Laboratory analysis was notable for a creatinine of 0.8, white blood cell count of 7.7, and atypical cells noted on his urine cytology. Of note, the patient had an abdominal CT imaging 18 month prior showing a normal left kidney and ureter except for a 4mm left upper pole nephrolith and multiple distal ureteral stones less than 6mm in size. At that time, the patient underwent an uncomplicated left ureteropyeloscopy, laser lithotripsy, and left ureteral stent placement by an endourologist.

Figure1: Coronal Images of CT Intravenous pyelogram, arterial phase, demonstrating a slightly enhancing left upper tract collecting system/renal mass.
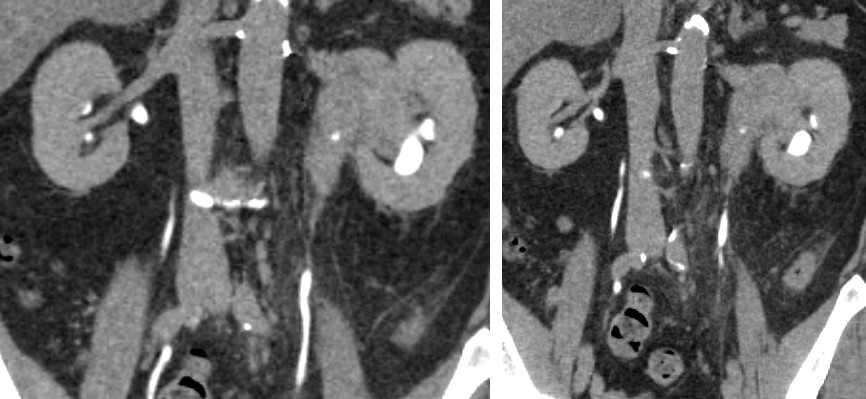
Now, due to the concerning presentation additional evaluation was performed including a cystoscopy, left retrograde pyelogram, and direct ureteroscopic visualization. The pyelogram showed narrowing of the left renal pelvis and limiting opacification of the collecting system. A left ureteropyeloscopy was performed to rule out an intrinsic collecting system lesion. This demonstrated normal appearing urothelium with narrowing of the renal pelvis and collecting system in a similar location seen on the pyelogram, consistent with extrinsic compression. Left ureteral barbotage and bladder washings were performed showing normal cytology. A positron emission tomography-computed tomography (PET-CT) noted radiotracer activity in the region of the known left renal mass (max SUV (standardized uptake value) 8.9) potentially representing malignancy, as well as a PET avid left cervical lymph node (max SUV 5.36). A core needle biopsy with CT guidance was performed showing reactive benign lymphoid tissue. For improved tissue sampling, fine-needle aspiration and excisional biopsy of the cervical lymph node was then obtained. Pathology results noted reactive follicular hyperplasia and focal nodular para-cortical hyperplasia. After appropriate counseling of the options, the patient ultimately elected for a surgical excision due to the risks of malignancy, progressing left renal obstruction and pain, and delay in diagnosis. An adrenal- sparing left radical nephrectomy and paraaortic lymph node dissection was performed through a left subcostal incision. The estimated blood loss was 180cc with an operative time 165 minutes. The patient had an uncomplicated post- operative course and was discharged on post-operative day 3. He remains free of disease recurrence at 65 months from his surgery.
Pathologic Findings
Pathologic evaluation of the surgical specimen demonstrated an ill-defined multinodular mass (6.8 x 5.9 x 5.5cm) with a glistening, homogeneous pink-yellow surface. The mass grossly did not invade into the calices, renal pelvis or ureter; and was noted to replace much of the renal sinus adipose tissue. Lastly, the mass was noted to not involve kidney parenchyma, renal vein or artery. The para-aortic lymphoid tissue was noted to have thirteen benign lymph nodes, the largest 1.4cm, with no suspicious areas concerning for malignancy.
Microscopically it was noted to have a lymphocytic infiltrate and scattered reactive germinal center. It stained grossly positive for CD 20, CD 10, and negative for BCL 2. Also noted were several areas of dense, hyalinized fibrosis that assumed a “storiform” pattern: a cartwheel appearance of the arranged fibroblasts and inflammatory cells. All of these findings are typical histopathologic features of an IgG4 related inflammatory pseudotumor [1].
Review of the Literature
IgG4-related disease is characterized by extensive IgG4- positive plasma cells and T-lymphocyte infiltration of various organs. Inflammatory pseudotumor as a manifestation of IgG4-related disease, with or without sclerosis, in the genitourinary tract is a rare entity and can often mimic a malignant or inflammatory process prior to definitive diagnosis [4]. Our literature review yielded a collection of case reports describing IgG4-retated pseudotumor of the genitourinary tract, as described below.
Renal
Renal lesions in IgG4-related disease are rare and most commonly manifest as multiple wedge-shaped or nodular cortical lesions in one or both kidneys. IgG4-related renal lesions can mimic renal cell carcinoma or transitional cell carcinoma in uncommon cases of a single unilateral mass, such as a renal lesion or focal unilateral renal pelvic wall thickening. Wang et al reported a case with CT/PET/MRI findings of a renal pelvic mass and diffuse lymphadenopathy, concerning for metastatic renal carcinoma. After completion of a nephroureterectomy with retroperitoneal lymph node dissection, the final pathology was determined to be an IgG4- related lesion. She completed a year of high dose steroid therapy for residual lymphadenopathy, with improvement in signs and symptoms [5]. Park and Kim reported a case of a 5cm renal pelvis mass, the mass was not biopsied prior to a right nephroureterectomy. Pathology subsequently revealed IgG4-related disease pseudotumor and not an upper tract urothelial cell carcinoma. Serum IgG4 levels were normal 1 month post operatively and no additional treatment was rendered [6].
Samji et al presented a case study where a patient demonstrated a suprarenal mass inseparable from the kidney. A CT-guided biopsy of the mass was performed. Hematoxylin and eosin stain sections of the core biopsy showed fibro adipose tissue with extensive fibrosis, scattered lymphoid follicles and areas of plasma cell-rich lymphoplasmacytic infiltrates. By immunohistochemistry, the IgG4 to IgG ratio was greater than 0.4 and there were more than 10 IgG4- positive plasma cells per high power field. There was no evidence of lymphoproliferative disease. The patient was tested retrospectively for IgG4 level, which was elevated to 140.7 mg/dl (normal range: 4-86 mg/dl). The patient started prednisone 20mg daily. One month after initiating steroid therapy, interval CT demonstrated decrease in the soft tissue masses [7]. This is a significant biopsy finding as it confirmed diagnosis while preventing the patient an invasive surgical procedure to rule out malignancy.
More recently, Tawhari et al. reported a case where a 55-year-old woman was found to have two ipsilateral renal masses with associated lymphadenopathy on evaluation for acute renal insufficiency. The masses were biopsied and found to be comprised of infiltrative IgG4 positive plasma cells. Treatment with corticosteroids resulted in resolution of renal masses and lymphadenopathy, however the patient ultimately progressed to end-stage renal disease requiring hemodialysis [8]. These are several instances of IgG4 pseudotumors mimicking renal and upper tract malignancies in which the lesions were biopsied and confirmed the diagnosis, thus negating a more invasive surgical procedure associate with longer recovery and higher patient morbidity.
Prostate
IgG4 related pseudotumor is also a consideration in prostate lesions. It can manifest as diffuse prostatitis or with focal lesions, mimicking prostatic adenocarcinoma. In 2023, Lee et al. published a case report describing a patient with a known history of IgG4-RD of the lacrimal gland with persistently elevated serum IgG4 after treatment. Rectal MRI performed for unrelated reasons was notable for an incidental PI-RADS 5 lesion, suspicious for primary prostatic adenocarcinoma. Serum prostate specific antigen (PSA) was normal at 1.5 mg/dL (0-4 mg/dL). Differential diagnosis of periprostatic inflammatory IgG4-RD was considered and subsequently proven on MRI-ultrasound fusion targeted biopsy [9].
Testicular/Paratesticular
Recent publications have postulated an association between paratesticular fibrous pseudotumor (PFP) and IgG4-related sclerosing fibrous lesions, given morphological similarities. PFP is a rare, intrascrotal benign fibrous mass of uncertain etiology. Given the lack of characteristic clinical signs or imaging findings, these masses can appear similar to a testicular neoplasm, leading to radical orchiectomy as opposed to a testis-sparing surgery. Frozen section assessment in testicular and paratesticular lesions may avoid unnecessary radical orchiectomy [10].
Urethra
IgG4 related pseudotumor has also been documented to occur in the urethra. Choi et al describe a case report of IgG4 related pseudotumor, in a patient who initially presented with lower urinary tract symptoms. Her past medical history was significant for eyelid inflammatory pseudotumor and pancreatitis over a decade prior. Urinalysis revealed hematuria and a firm urethral mass was discovered on cystoscopy. Core needle biopsy findings were consistent for an IgG4 pseudotumor. Pt underwent steroid therapy for several months, with marked improvement on follow up MRI [4].
As there is a paucity of research, information regarding recurrence rates is limited. It is important to keep in mind that prior medical history, including history of autoimmune pancreatitis or other inflammatory mass lesions, could suggest IgG4 related disease processes. In most cases, a needle biopsy under or intraoperative frozen sectioning can be helpful to establish a pathologic diagnosis prior to extirpative surgery. There are three key histopathologic findings of this disease: [1] dense lymphoplasmacytic infiltration, [2] storiform-type fibrosis, and [3] obliterative phlebitis [11]. If two of the three key histologic findings are present, the possibility of IgG4-related disease is strongly suggested pathologically. The most essential criterion to diagnose the disease is the detection of IgG4-positive plasma cells in the lesion [7].
Discussion
IgG4-related disease is a recently acknowledged systemic disease that is characterized by lymphoplasmacytic inflammation and fibrosis in the affected tissues. The prevalence of urologic IgG4-related disease is not known, likely due to the lack of familiarity and being under-reported. Most patients are men and over the age of 50 years and most of the IgG4-related disease presents subacutely and often identified through radiologic findings or unexpectedly in pathologic specimens [2]. Radiographically, arterial lesions are characterized on CT by homogeneous wall thickening and enhancement in the last phase after contrast administration, corresponding to sclerosing inflammation involving the adventitia [12]. The closest histopathological mimickers of IgG4-related disease are lymphomas, and as such, clonality studies are necessary to rule out these cancers. Furthermore, there is great difficulty distinguishing infiltrates caused by IgG4-related disease and other inflammatory infiltrates, such as those adjacent to neoplastic lesions [2]. Therefore, a biopsy of the target lesion must be accurately performed in order to rule out the target lesions as malignant or disease mimicker such as an IgG4 pseudotumor. While no randomized treatment trials have been conducted, first like treatment with glucocorticosteriods is typically the first line option when vital organs are involved to prevent serious organ dysfunction and failure. In addition, azathioprine, mycophenolate mofetil, and methotrexate as steroid-sparing treatment options or remission-maintenance therapy after steroid-induced remissions but treatment efficacy has yet to be tested in clinical trials.
Evans et al. recently reported on the long-term outcomes of IgG4-related kidney and retroperitoneal involvement in the United Kingdom via a retrospective observational study [13]. This study included twenty-eight patients (eighteen with intrinsic renal disease, ten with retroperitoneal fibrosis). All patients had either renal biopsies or biopsies of distant sites that were consistent with IgG4-related disease. Twenty-five (89.3%) were treated with immunosuppression, whereas three patients were not. Treatment consisted of tapering prednisolone at a mean starting dose of 40 +/- 16 mg/day. One patient received 3 doses of intravenous methylprednisolone prior to oral prednisolone treatment, and four patients received a steroid-sparing agent (azathioprine) as part of initial treatment alongside prednisolone. The mean follow- up was noted to be 60 months (12-108 months). Thirteen patients (46.4%) had a relapse at any site following initial treatment (ten (55.6%) with intrinsic renal disease, 3 (30%) with retroperitoneal fibrosis). All patients noted to have a relapse were treated with immunosuppression and no deaths were noted.
The case we present is unlike previously described cases for several reasons, and why it is important to present. Multiple attempts were made to obtain a histopathological diagnosis. However, the biopsies did not demonstrate findings consistent with IgG4 related disease. The patient in our case represents a difficult to diagnose and treat clinical scenario since biopsy data was not conclusive, unlike the patients discussed by Evans et al. While ruling out urothelial carcinoma, the ureteropyeloscopy findings were concerning for extrinsic mass effect, potentially due to malignancy. Coupled with his imaging concerning for upper tract urothelial cell carcinoma, including a PET avid left renal lesion, the patient ultimately underwent an open radical left nephrectomy with lymph node dissection. The diagnosis of an IgG4-related inflammatory pseudotumor was able to be determined only after surgical pathology was obtained. Of note, this patient has been radiographically disease free and has required no immunosuppression, meaning there is no evidence of systemic disease progression, and the patient has been able to avoid the short and long-term risks of immunosuppression. Also, while previously not reported, it is worth considering how, if any, the patient’s previously left ureteropyeloscopy for his kidney stone removal played a role in stimulating the IgG4 psuedotumor growth. Regardless, the growth of the left renal lesion evident on CT imaging over a period less than 18 months shows the aggressive nature of the disease.
Conclusion
We present the disease process, imaging findings, pathologic analysis, and treatment of a rare disease found in Urology. IgG4-related diseases are known to represent a systemic disease that leads to lymphoplasmacytic inflammation and fibrosis within the affected tissues. Although renal involvement via intrinsic kidney disease and/or retroperitoneal fibrosis has been well described, we presented a rare case of a peri-renal mass masquerading as upper tract urothelial cell carcinoma. Currently, there is no standardized method for the diagnosis and treatment for these patients. This disease process represents a challenge to Urologists due to the difficulty in diagnosis, possible inability to exclude malignancy, and concern for progressive renal obstruction even if benign. A published response rate of less than 50% with immunosuppression also complicates the surgical decision-making process with respect to delay in diagnosis and treatment, as well as the added surgical difficulties associated with progressive inflammation. Additional research in the field of IgG4-related disease is needed to identify improved diagnostic modalities, the role of immunosuppressive therapy, and the surgical management in this disease process.
• Author Note: The contents of this publication are the sole responsibility of the author (s) and do not necessarily reflect the views, opinions, or policies of Uniformed Services University of the Health Sciences (USUHS), the Department of Defense (Do D) or the Departments of the Army, Navy, or Air Force.
References
-
Deshpande V (2012) Consensus statement on the pathology of IgG4-related disease. Mod Pathol 25(9): 1181-1192.
-
Stone JH (2012) IgG4-related disease. N Engl J Med 366(8): 1460-1471.
-
Cortazar FB (2015) IgG4-related disease and the kidney. Nat Rev Nephrol 11(10): 599-609.
-
Choi (2012) Immunoglobulin G4-Related Sclerosing Disease Involving the Urethra: Case Report. KJR 13(6): 803-807.
-
Wang Y, Chen X, Luo R, Wang H, Wang G, et al. (2014) IgG4-related systemic disease mimicking renal pelvic cancer: a rare case. World J Surg Oncol 12: 395.
-
Park HG, Kim KM (2016) IgG4-related inflammatory pseudotumor of the renal pelvis involving renal parenchyma, mimicking malignancy. Diag Path 11-12.
-
Samji V, Haykal T, Danish R (2020) A Case of an IgG4- Related Disease Mimicking Malignancy and Resolving with Steroids. Cureus 12(7): e9476.
-
Tawhari M, Al Oudah N, Al Zahrani Y, Radwi M (2022) IgG4-related kidney disease associated with end-stage kidney disease, renal pseudotumor, and renal vein thrombosis. Cureus 14(3): e22837.
-
Lee (2023) Focal IgG4-related periprostatic “PI-RADS 5” pseudotumor mimicking prostatic adenocarcinoma. Rads CR 18(6): 2158-2164.
-
Crestani (2023) Paratesticular fibrous pseudotumor with histologcal features of IgG4-related disease: two case reports and review of the literature. Glnd Sg 12(3): 426-431.
-
Montironi R, Scarpelli M, Cheng L, Lopez-Beltran A, Burattini M, et al. (2013) Immunoglobulin G4– related disease in genitourinary organs: an emerging fibroinflammatory entity often misdiagnosed preoperatively as cancer. Eur Urol 64(6): 865-872.
-
Inoue D, Zen Y, Abo H (2011) Immunoglobulin G4-related periaortitis and periarteritis: CT findings in 17 patients. Radiology 261(2): 625-633.
-
Evans (2019) Clinical manifestations and long-term outcomes of IgG4-related kidney and retroperitoneal involvement in a United Kingdom IgG4-Related Disease Cohort. Kidney International Reports 4(1): 48-58.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review