A Study of Improvement in the Gastro Intestinal Symptoms and Quality of Life after Laparoscopic Cholecystectomy
Objective: To observe the effects of laparoscopic cholecystectomy on gastrointestinal symptoms and improvement in Health- Related Quality of Life. Methods: 100 symptomatic patients with cholelithiasis who underwent laparoscopic cholecystectomy between November 2020 to December 2022 were evaluated for improvement in their gastrointestinal symptoms and Quality of life using the standard questionnaire entailing the Gastrointestinal Symptom Survey (GISS) score and Short Form Survey (SF-36) score from preoperative to 3 months of postoperative follow up. Results: Of 100 patients with mean age 35.16 years SD ±11.98, 82% were females with chronic cholecystitis. Laparoscopic cholecystectomy resulted in significant improvement of gastrointestinal symptoms as revealed by GISS mean scores which showed a decline. The quality of life emblematised by the mean SF-36 scores (84.11±17.31 SD) that showed slight decline from pre- operative (76.55±23.19 SD) till discharge (73.30±16.36 SD) maximally reflected in mean physical function, role limitations due to physical health and social function scores with trend towards gradual improvement from 3 weeks (83.05±15.55 SD) to 12 weeks (91.55±11.89 SD). As regards the individual symptoms constituting GISS, 15 of the 16 gastrointestinal symptoms showed significant improvement with de novo appearance of bloating (10%) and fullness after meals (8%). Conclusion: Laparoscopic cholecystectomy is immensely effective in improvement of Gastrointestinal symptoms and HRQOL.
Background
Since the era of laparoscopic revolution, laparoscopic cholecystectomy has gained widespread popularity such that open cholecystectomy has gone out of the race and has become a rescue procedure in case of difficult or inaccessible gall bladder or carcinoma gall bladder where extended cholecystectomy needs to be performed. Being a demanding and one of the most commonly performed procedure, criticism regarding it overuse has been a highlighting issue.
Cholecystectomy removes the gall stones but symptoms of gall bladder disease may still be persistent which would have an impact on the quality of life of the patients. Following laparoscopic cholecystectomy, return to the normal daily activity is early. A relatively harmless procedure like laparoscopic cholecystectomy will generally not lead to deterioration of quality of life of the patients unless there are any complications during the procedure or persistent gastrointestinal symptoms that would continue to impair the quality of life.
Methods
Subjects
Symptomatic patients diagnosed with gall stone disease between November 2020 to December 2022 at a tertiary care hospital were identified. The protocol was approved by the Institutional Ethics Committee. 100 patients who underwent laparoscopic cholecystectomy and completed the preoperative Gastrointestinal Symptom Survey (GISS) and Short Form-36 Health Survey (SF-36) were included. Pre-operative surveys were completed on admission. After surgery, similar questionnaire was administered to the patients at the time of discharge, at 3 weeks, 6 weeks, 10 weeks and 12 weeks after the procedure to assess the impact of laparoscopic cholecystectomy on improvement in the quality of life and the gastro intestinal symptoms. The subjects who were unavailable at the time of contact, or the ones who didn’t complete the survey were excluded. A chart abstraction of all the subjects was performed. Demographic information, preoperative laboratory data, surgical pathology was recorded.
Gastrointestinal Symptoms Evaluation
The gastrointestinal symptom survey (GISS) score was used to assess gastrointestinal symptoms. The validated surveys for symptoms associated with gall stone disease were studied in order to create this survey at the University of Alabama in Birmingham.16 gastrointestinal symptoms which were a part of is survey included pain upper abdomen, crampy abdominal pain, pain after fatty/rich foods, pain that waked up at night, pain radiating to the back, abdominal pain all the time, nausea, vomiting, bloating, excessive flatulence, feeling full after small meals, pressure in the chest, diarrhoea constipation and stomach contents in the throat. Many aspects of abdominal pain were researched because it was the most prevalent symptom of gallstones. The presence of the symptom(present=1,absent=0) along with their frequency(occasional=1, often=2 and very often=3) with the level of distress caused by each symptom(not bothersome=1, mildly distressing=2, moderately distressing=3 and severely distressing=4) were studied using the GISS questionnaire. Surveys were scored by multiplying the presence (0-1), frequency (1-3) and the severity of the symptoms(1-4) which was modified from the original scoring method according to our study population with our scores ranging from 0-192. The value of GISS is inversely related to the improvement of the symptoms. More the GISS score more frequent the symptoms with greater severity. Lower the GISS score, more the improvement [1].
Quality of Life
Health related quality of life has been studied using Short Form-36 Health Survey which is a validated survey to assess the impact of a procedure on the quality of life. Dating to 1970’s, the Santa Monica based Rand Cooperation’s Research served as the basis for the development of SF-36. It was initiated by creating an 18item scale in 1984 and progressively adding to create a 36 item short form survey in 1986 to fulfil the lacunae and the pitfalls of the SF-20 score. Rands Medical Outcomes Study emphasised on treatment of chronic medical conditions as well as psychiatric disorders. The SF-36 incorporated scores of 8 domains of quality of life: physical function, role limitations due to physical health, bodily pain, general health, vitality, social functioning, emotional health, role limitations due to emotional health, reported health transition [2]. The SF-36 surveys were scored using Ortho Tool Kit with scores of each domain ranging from 0 to maximum 100%.
Results
Age and Gender
Of the 100 patients enrolled in the study ranging from 18 -72 years of age, mean age of the patients was 35.16 years± 11.98 SD. 82% of the patients were females and 18% were males with female: male ratio of 1:4.5. The predominant histopathological finding beingchronic cholecystitis. The demographic variables of the patients are shown in Table 1.
100 patients who completed the preoperative and the postoperative GISS and SF-36 survey were included. The ones who were lost to follow up or didn’t complete the survey were excluded. A study population of 100 with a mean 3 months follow up were studied.
Gastrointestinal Symptoms and GISS
On studying the individual symptoms of GISS, it was found that upper abdominal pain (90%) was the most common symptom in patients pre operatively followed by bloating (70%), vomiting (68%), nausea and pain after fatty food in 65% with feeling of fullness after meals in 62%. Significant improvement in gastrointestinal symptoms was seen after laparoscopic cholecystectomy. On comparing the presence of 16 GI symptoms of GISS pre operatively and after 3 months of surgery, improvement in 14 of the 16 Gastro intestinal symptoms were seen. The symptoms that revealed significant improvement included pain upper abdomen which was present in 90% patients pre operatively and 24% patients post operatively, nausea in 65% preoperatively and 16 % post operatively, pain after fatty foods in 65% preoperatively and 5% post operatively, pain that waked up at night in 47% preoperatively and 2% post operatively, pain radiating to the back in 32% preoperatively and 4% post operatively , vomiting in 68% preoperatively and 6% post operatively, pressure in the chest 32% pre operatively and 2% post operatively, excessive flatulence 35% pre operatively and 5% post operatively, belching 42% pre operatively and 11% post operatively.
The symptoms of crampy and constant abdominal pain which were present in 52% and 20% of the subjects preoperatively were absolutely cured after 3 months post- operative follow up. Diarrhea although present in 17 % of the pre-operative patients was persistent in 10% patients after 3 months (p=0.147), constipation which was a distressful symptom (30%) pre operatively and 19% post operatively (p=0.071). It was shown that more than half of the patients remained to experience early satiety since the feeling of fullness following small meals or early satiety was still present in 36% of patients after surgery as opposed to 62% preoperatively. Also bloating continued to be a distressing symptom in the post-operative period with a frequency of 32% after 3 months follow up compared to 70 % pre operatively. Symptoms associated with irritable bowel syndrome including diarrhoea (p=0.147) and constipation (p=0.071) didn’t show much improvement. Figure 1 shows the presence of symptoms pre and post operatively.
On analyzing the various categories of pain described in the GISS, all the 6 indices of pain showed improvement from pre operatively to 3 months of follow up after laparoscopic. De novo appearance of symptoms post cholecystectomy included bloating (10%), feeling of fullness after small meals (8%), diarrhea (4%), nausea (3%), vomiting, belching and excessive flatulence (2%); pressure in chest (1%) pain all the time (1%) being the most significant one.
Three months following a laparoscopic cholecystectomy, the total GISS score significantly improved from a mean value of 73.36±35.61 SD to 10.79±10.43 SD. Table 3 shows the changes in preoperative and postoperative GISS scores. Reduction in scores signifies symptom improvement evidenced by decrease in frequency and distressfulness of the symptoms thereby reducing the overall GISS score.
SF-36
SF-36 scores from preoperative to 3 months after surgery showing the impact of laparoscopic cholecystectomy on the quality of life have been shown in table 4. 36 questions of SF-36have been aggregated to compose 8 component scales described previously. All the component scales have shown considerable improvement between pre-operative to 3 months post operatively. A domain or dimension represents the area of behavior or experience that we are trying to measure [3].
The meandomain scores of SF-36 showed decline from pre-operative (76.55±23.19 SD) to the time of discharge (73.30±16.36 SD) and then gradual improvement from 3 weeks (83.05±15.55 SD) to 12 weeks (91.55±11.89 SD). The overall mean score of physical function was found to be 85.23±24.82 SD with pre-operative score of 73.50±36.03 SD to a slight reduction to 72.75±31.00 SD at the time of discharge and reaching up to 94.10±13.62SD by the end of 12 weeks of follow up. The reduction in physical function was also reflected in role limitations due to physical health which showed a decline from preop (73.50±36.03 SD) to 72.75±31.00 SD at discharge with 84.25±21.22 SD at 3 weeks to 94.10±13.62 SD by the end of 12 weeks. The mean score of social function (88.87±15.83 SD) revealed slight reduction from with a pre-operative mean score of 78.28±19.57 SD to 77.34±17.49 SD at dischargeimproved to 86.96±13.93 SD at 3 weeks and 97.66±6.74 SD by 12 weeks. The remaining SF-36 domains showed progressive improvement from the pre-operative survey to the survey completed 12 weeks after the operation. The amount of follow-up time was found to be directly linked to improvement in the different quality of life dimensions. The scores for Quality of Life improve with the period of follow-up.
| Variable | Parameter | |
|---|---|---|
| Age | Years | 35.16± 11.98 SD |
| Gender | Male | 18 |
| Females | 82 | |
| M:F | 01:04.5 | |
| Preoperative Laboratory data | Total Leukocyte count | 7199±2028.21 SD |
| Total Bilirubin | 0.81±0.43 SD | |
| Alkaline Phosphatase | 99.6±33.83 SD |
Table 1: Study demographics of subjects undergoing laparoscopic cholecystectomy.
| Symptom | Preoperative (n=%) | Post-operative (n=%) | p-value | De novo /Emergent |
|---|---|---|---|---|
| Pain upper abdomen | 90 | 24 | <0.001 | 0 |
| Crampy pain abdomen | 52 | 0 | <0.001 | 0 |
| Nausea | 65 | 16 | <0.001 | 3 |
| Pain after fatty foods | 65 | 5 | <0.001 | 0 |
| Pain that waked up at night | 47 | 2 | <0.001 | 0 |
| Pain radiating to back | 32 | 4 | <0.001 | 0 |
| Vomiting | 68 | 6 | <0.001 | 2 |
| Bloating | 70 | 32 | 0.009 | 10 |
| Abdominal pain all the time | 20 | 0 | <0.001 | 1 |
| Pressure in the chest | 32 | 2 | <0.001 | 1 |
| Feeling full after small meals | 62 | 36 | <0.001 | 8 |
| Excessive Flatulence | 35 | 5 | <0.001 | 2 |
| Belching | 42 | 11 | <0.001 | 2 |
| Diarrhoea | 17 | 10 | 0.147 | 4 |
| Constipation | 30 | 19 | 0.071 | 0 |
| Stomach contents in the throat | 37 | 5 | <0.001 | 0 |
Table 2: GISS Parameters (Gastro Intestinal Symptom Survey).
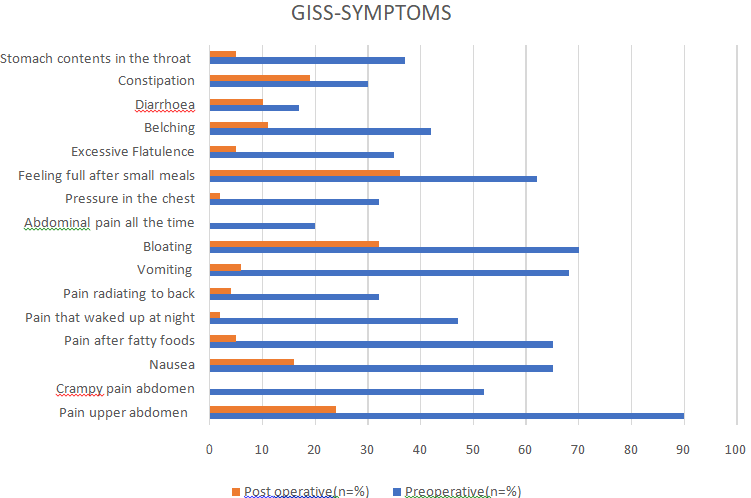
Chart 1: Comparison of Gastrointestinal Symptoms pre and post laparoscopic cholecystectomy.
| Timeline | GISS- Score |
|---|---|
| Mean ± Std. Deviation | |
| Pre-Operative | 73.36±35.61 |
| At Discharge | 20.98±9.82 |
| 3 Weeks | 18.43±10.80 |
| 6 Weeks | 15.11±10.09 |
| 10 Weeks | 12.67±10.98 |
| 12 Weeks | 10.79±10.43 |
| Total | 25.22±27.84 |
Table 3: Mean GISS score at different intervals.
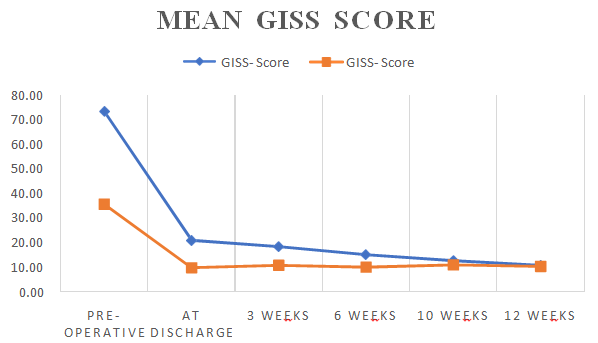
Chart 2: Mean GISS score from pre-operative to 12 weeks post operatively.
| Domains | Preop | Discharge | 3 weeks | 6 weeks | 10 weeks | 12 weeks |
|---|---|---|---|---|---|---|
| PF | 76.55±23.19 | 73.30±16.36 | 83.05±15.55 | 89.40±13.11 | 90.80±12.05 | 91.55±11.89 |
| RP | 73.50±36.03 | 72.75±31.00 | 84.25±21.22 | 92.50±13.53 | 94.25±11.71 | 94.10±13.62 |
| RE | 81.00±37.08 | 88.59±24.00 | 93.67±14.75 | 96.34±10.47 | 96.32±10.27 | 96.49±9.84 |
| VT | 71.75±13.84 | 72.20±12.66 | 82.35±11.90 | 87.00±8.82 | 88.60±7.76 | 89.17±7.76 |
| SF | 78.28±19.57 | 77.34±17.49 | 86.96±13.93 | 96.05±9.50 | 96.94±7.09 | 96.94±7.09 |
| BP | 62.72±22.22 | 69.64±18.57 | 81.27±17.30 | 92.29±12.12 | 93.24±11.18 | 93.53±10.75 |
| GH | 61.15±14.05 | 71.35±14.84 | 82.00±12.71 | 87.40±8.75 | 89.95±8.95 | 91.15±8.07 |
| HC | 45.75±26.37 | 70.25±18.01 | 85.35±17.40 | 91.50±13.86 | 93.25±12.74 | 94.50±12.09 |
Table 4: Domain scores if SF-36 from preoperative to 3 months following laparoscopic cholecystectomy PF=Physical Function; RP=Rol
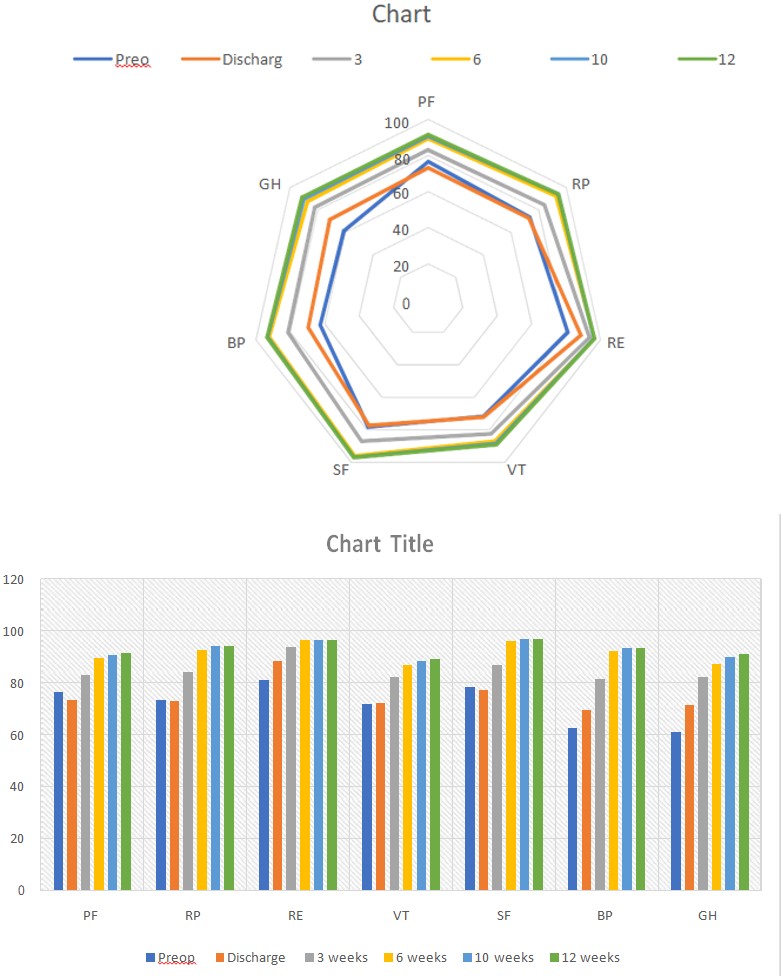
Chart 3.1: Mean domain scores of SF-36.
Chart 3.2: Mean SF-36 scores.
Changes in the domains of SF-36 from pre operatively to discharge, 3 weeks, 6 weeks. 10 weeks and 12 weeks after laparoscopic cholecystectomy. Significant changes over time by Friedman’s ANOVA are denoted by p<0.001.
Discussion
In general surgery practice, laparoscopic cholecystectomy is one of the most commonly performed procedure such that it is regarded as the bread and butter for a general surgeon. Since the advent of laparoscopy, laparoscopic cholecystectomy has shown phenomenal evolution with regards to the booming number of cases as well as improvisation of the technique. Laparoscopic cholecystectomy has revolutionized surgical practice to an enormous extent and its already claimed that laparoscopic cholecystectomy is the new gold standard for symptomatic gallstone disease [4]. Patients with gall bladder disease have an assortment of specific or non-specific gastrointestinal symptoms attributable to the presence of gallstones which may or may not have a probability of being benefitted by the surgery.
Laparoscopic cholecystectomy being a minimally invasive procedure, the patients usually have early return to their normal functions. The impact of laparoscopic cholecystectomy on Gastrointestinal Symptoms has been studied by using the GISS (Gastro Intestinal Symptom Survey) score and quality of life using Short Form Survey (SF-36) score. GISS, originally developed by the University of Alabama has been devised after studying the symptomatology of gall stone disease and previous symptom surveys. It was used by Finan KR, et al_._ [1] to assess improvement in the gastrointestinal symptoms after laparoscopic cholecystectomy. In our study, GISS has been modified for our set of population. The resultant scores have shown a significant decline from preoperative to 3 months post operatively, reflected by the reduction of mean GISS value which was consistent with their study. In our study, 14 of the 16 GISS symptoms showed a reduction from preop to 3 months of post op follow up.
In our study, crampy and constant abdominal pain was absolutely cured after 3 months post operatively. Diarrhoea was a persistent symptom in 10% patients after 3 months. Whereas more than half of the patients remained to experience early satiety post operatively, bloating continued to be a distressing symptom in the post-operative period. Symptoms associated with irritable bowel syndrome including diarrhoea constipation didn’t show much improvement in our study. Gui, et al. [5] follow up study revealed that bloating, fat intolerance, nausea, vomiting, heartburn, dyspepsia significantly improved after laparoscopic cholecystectomy, with the persistence of abdominal pain in 30% of subjects. Weinert, et al. [6] retrospective study showed dyspeptic symptoms (flatulence, heartburn, and belching) 5 times more likely to persist than biliary (nausea, food intolerance, vomiting, and tender to touch) after cholecystectomy. Whereas in our study, symptoms of bloating, feeling of fullness after small meals, diarrhoea, nausea, vomiting, belching, excessive flatulence, pressure in chest, pain all the time appeared de novo in decreasing order of frequency. In a study by BM Ure, et al. [7], biliary colic was significantly reduced which was at par with our study whereas flatulence persisted in 50% of the patients after laparoscopic cholecystectomy which was much higher than our study.
In our study, SF-36 which is an effective, generic QOL measure was used to measure and compare the scores of Quality of Life in patients pre and post laparoscopic cholecystectomy. An important component of a questionnaire’s appropriateness in accurately measuring over time in the same patient, assessing prospective changes in the patient’s health status [8]. SF-36 is a validated survey which has been used previously and provided fruitful results in studying the impact of disease or intervention on the quality of life. Several studies have been conducted till date utilising SF-36 for assessing and comparing the quality of life in patients undergoing laparoscopic cholecystectomy with some of them described. In Finanet KR, et al. [1] study described previously, improvement in scores of role limitations caused by physical health, bodily pain, and social function were seen after laparoscopic cholecystectomy whereas in our study physical function, role limitations due to physical function and social function scores of SF-36 showed a decline from preoperative to discharge followed by gradual improvement of all sub scores. In a study by Lien HH, et al_._ [9] using SF-36, it was seen that preoperative SF-36 scores from gallstone patients were significantly inferior to the age and sex matched norms in all the dimensions than the post-operative scores. Similar findings were observed in our study where the most domain scores of SF-36 showed improvement from preoperative to 12 weeks post operatively. Simon Henry Palsson, et al. [10] study on registration of Health-Related Quality of Life in patients undergoing cholecystectomy using SF-36 as an instrument for measuring the impact of gallstone surgery on HRQOL revealed improvement in SF-36 scores with highest responsiveness observed for bodily pain. Their study showed that HRQOL in a population undergoing gallstone surgery equalled or exceeded the age and gender matched general population for all subscales. These were consistent with our study. Another longitudinal QOL study from Taiwan by Shi HY, et al. [11] using SF-36 and GIQLI questionnaire, the preoperative SF-36 scores were lower for an age and gender matched population and laparoscopic cholecystectomy led to improvement in the physical and mental well-being. Quintana, et al. [12] study showed that low risk surgical patients with symptomatic cholelithiasis had better quality of life gains than the asymptomatic high risk patients. In our study, all the domains of SF-36 showed progressive improvement from pre-operative to 3 months after the surgery.
| Authors | Year | Study | Instruments used | Follow up | Results | Our Study |
|---|---|---|---|---|---|---|
| K.R Finan, et al. [1] | 2006 | Improvement in gastrointestinal symptoms and quality of life after cholecystectomy | GISS, SF-36 | 1 month | Improvement in the role limitations caused by physical health ,bodily pain, and social function scores after LC | Reduction in the physical function, role limitations due to physical function and social functions from pre operativeto discharge followed by gradual improvement |
| HH Lien, et al. [9] | 2010 | Changes in quality-of-life following laparoscopic cholecystectomyin adult patients with cholelithiasis | SF-36 | Role physical, role-emotional, and bodily pain | ||
| Simon Henry Palsson, et al. [10] | 2011 | Registration of health- related quality of life in a cohort of patients undergoing cholecystectomy | SF-36 | 1 month | Preoperative subs cores were significantly lower than postoperative | Postoperative sub scores improved from discharge to3 months except physical function, Role limitations due to physical health and social function which showed a decline at discharge followed by gradual improvement |
| Quintana, et al. [12] | 2005 | Health-related quality of life and appropriateness of cholecystectomy. | SF-36 GIQLI | 1 year | Improvement in bodily pain and social function as well as vitality scores but not physical health in subjects undergoing cholecystectomy | Reduction in scores of physical and social function scores of vitality and bodily pain improved |
Table 5: Studies using SF-36 to assess and compare the quality of life in patients who underwent laparoscopic cholecystectomy Men
Table 5: Studies using SF-36 to assess and compare the quality of life in patients who underwent laparoscopic cholecystectomy Mentes, et al. [13] study showed significant improvement in gastrointestinal symptoms in both symptomatic and asymptomatic patients with gallstones with more marked improvement in symptomatic patients. However they used GIQLI (Gastrointestinal Quality of Life Index) as a measure to detect improvement in gastrointestinal symptoms. Many other studies have also used GIQLI. Whereas in our study GISS has been used Eupasych EMD, et al. [14] study revealed that laparoscopic cholecystectomy resulted in immediate and effective improvement of quality of life both with respect to dimensions and single factors reflecting quality of life which was also reflected in our study. Plaisier et al studied the Quality of Life and the Course of Biliary and Gastrointestinal Symptoms after Laparoscopic and Conventional Cholecystectomyand demonstrated that laparoscopic cholecystectomy improves quality of life but they used Nottingham Health Profile for assessing the quality of life whereas our study used SF-36 score [15].
Conclusion
Laparoscopic cholecystectomy results in immediate and effective improvement in quality of life with respect to overall dimensions and individual domains. This was reflected in all the domains of SF-36 pre operatively to 3 months of follow up after surgery. Our study led to the conclusion that laparoscopic cholecystectomy is immensely effective in improvement of Gastrointestinal symptoms and health related quality of life.
Ethical Approval
The study was approved by the Jawaharlal Nehru Medical College and Hospital Institutional Ethics Committee
Conflict of Interest
Authors declare no conflict of interest.
Sources of Financial Support
The study did not have sponsorship.
References
-
Finan KR, Leeth RR, Whitley BM, Klapow JC , Hawn MT (2006) Improvement in gastrointestinal symptoms and quality of life after cholecystectomy. The American journal of surgery 192(2): 196-202.
-
Ware J, Kosinski, Dewey M, Gandek JE (2000) BSF-36 Health Survey Manual & Interpretation Guide Boston. QualityMetric Incorporated.
-
Guyatt GH, Feenyd DH, Donald L, Patrick (1993) Easuring Health-Related Quality of Life.Annals of Internal Medicine118(8): 622-629.
-
Schirmer BD, Edge SB, Dix J, Hyser MJ, Hanks JB, et al. (1991) Laparoscopic cholecystectomy: Treatment of choice for symptomatic cholelithiasis Ann Surg 213(6): 665-677.
-
Gui GP, Cheruvu CV, West N, Sivaniah K, Fiennes AG (1998) Is cholecystectomy effective treatment for symptomatic gallstones? Clinical outcome after longterm follow-up Ann R Coll Surg Engl 80(1): 25-32.
-
Weinert CR, Arnett D, Jacobs D Jr, Kane RL (2000) Relationship between persistence of abdominal symptoms and successful outcome after cholecystectomy Arch Intern Med 160(7): 989-995.
-
Ure BM, Troidl H, Spangenberger W, Lefering R, Dietrich A, at al (1995) and others Long-term results after laparoscopic cholecystectomy. British Journal of Surgery 82(2): 267-270.
-
Carraro S, El Mazloum D, Bihl F (2011) Health-related quality of life outcomes after cholecystectomy. World J Gastroenterol 17(45): 4945-4951.
-
Lien HH, Huang CC, Wang PC, Huang CS, Chen YH, et al. (2010) Changes in quality-of-life following laparoscopic cholecystectomy in adult patients with cholelithiasis. Journal of Gastrointestinal Surgery 14(1): 126-30.
-
Pålsson SH, Rasmussen I, Lundström P, Österberg J, Sandblom G (2011) Registration of health-related quality of life in a cohort of patients undergoing cholecystectomy. International Scholarly Research Notices.
-
Shi HY, Lee HH, Chiu CC, Chiu HC, Uen YH, et al (2008) Responsiveness and minimal clinically important differences after cholecystectomy: GIQLI versus SF-36. Journal of Gastrointestinal Surgery 12(7): 1275-1282.
-
Quintana JM, Cabriada J, Aróstegui I, Oribe V, Perdigo L, et al. (2005) Health-related quality of life and appropriateness of cholecystectomy. Ann Surg 241 (1): 110118.
-
Mentes BB, Akin M, Irkörücü O, Tatlicioğlu E, Ferahköşe Z, et al. (2001) Gastrointestinal quality of life in patients with symptomatic or asymptomatic cholelithiasis before and after laparoscopic cholecystectomy. SurgEndosc 15(11): 1267-1272.
-
Eupasych E, Kärkkäinen J, Harju J, Juvonen P, Kokki H, et al. (1993) Immediate improval in the quality of life after laparoscopiccholecystectomy. Minimally Invasive Therapy 26(3): 139-146.
-
Plaisier PW, Van der Hul RL, Nijs HG, Den Toom R, Terpstra OT, et al. (1994) Quality of life after reatment of gallstones: results of a randomised study of lithotripsy and open cholecystectomy. The European journal of surgery Acta chirurgica 160(11): 613-617.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review