Basal Cell Carcinoma of the Prostate: Case Reports Including an Unusual Presentation
Basal cell carcinoma of the prostate is a rare tumor subtype arising from the prostatic basal cells and follows a variable clinical course. We describe two cases of patients with basal cell carcinoma of the prostate treated at our center. One case involves a patient with prior radiation with brachytherapy for prostatic adenocarcinoma, who subsequently developed a locally aggressive and invasive basal cell carcinoma of the prostate that eventually required pelvic exenteration. To our knowledge, we are the first to describe a case of basal cell carcinoma of the prostate in a patient with prior radiation with brachytherapy for prostatic adenocarcinoma.
Introduction
Prostate cancer is the fourth most common malignancy worldwide and the second leading cause of cancer-related deaths among men in the Unites States [1, 2]. Though the vast majority of prostate cancer is adenocarcinoma (>95%), there remain rare clinical subtypes that have distinctive histopathologic and biological features [3]. Of these subtypes, prostate cancer derived from basal cells, known as prostatic basal cell carcinoma (BCC), is exceedingly rare, with about 100 reported cases in the literature [4]. Due to its rarity, a paucity of literature exists on how to manage these patients. Herein, we present a case series of two patients with prostatic BCC. One of these patients had a history of prostatic adenocarcinoma and radiation therapy two decades previously, and to our knowledge is the only described case of a patient with prostatic BCC following radiation with brachytherapy for prostatic adenocarcinoma.
Case One
The patient is an 84-year-old African-American man who has a history of low-risk acinar-type prostatic adenocarcinoma (PSA 6.88 ng/mL, Gleason score 3+3=6, cT1c) in 1997 and was treated with brachytherapy. His PSA nadir was 0.1 ng/mL post-brachytherapy and remained stable since then with no evidence of biochemical recurrence. He was routinely followed by urology for lower urinary tract symptoms (LUTS) over the course of the following two decades. Diagnostic work-up over this time period revealed prostatic hyperplasia and a bladder neck contracture (BNC) for which he underwent several direct visualizations and incisions. He presented to clinic twenty-three years after initial brachytherapy with worsening urinary frequency, urgency, weak stream, and incomplete emptying and with new onset bilateral hydronephrosis found on computed tomography (CT) axial imaging, consistent with bladder outlet obstruction. His serum creatinine had also increased from a baseline of 1.3 mg/dL to 2.82 mg/dL. His PSA remained undetectable (<0.014).
He then underwent transurethral resection of the prostate (TURP) for relief of symptoms. Intra-operatively, prostatic hyperplasia was noted with overgrowth of the trigone and ureteral orifices. Prostatic tissue was resected, and bilateral ureteral stents were placed to facilitate healing and drainage.
Microscopically, 98% of the TURP specimen was involved by anastomosing basaloid cells with peripheral palisading (Figure 1). Tumor nests exhibited stromal clefting against a desmoplastic stromal background. Mitotic activity within the basaloid cells was markedly elevated and peri-neural invasion was identified, but necrosis was absent. There were no foci of normal prostatic glands or evidence of recurrent acinar-type adenocarcinoma. By immunohistochemistry, the tumor had a basal cell phenotype, strong nuclear staining with p63, and focal cytoplasmic CK-903 positivity. The neoplastic cells were also positive for BCL-2. Conversely, the tumor was negative for NKX3.1, PSA, PSAP, AMACR, and ERG. The tumor cells were also negative for CK20, p53, S100, synaptophysin, chromogranin and HER2. The combination of the morphology and immunophenotype was diagnostic of prostatic basal cell carcinoma. Next Generation Sequencing was subsequently performed on the biopsy, demonstrating an ATM (Ataxia-Telangiectasia, Mutated) gene deletion.
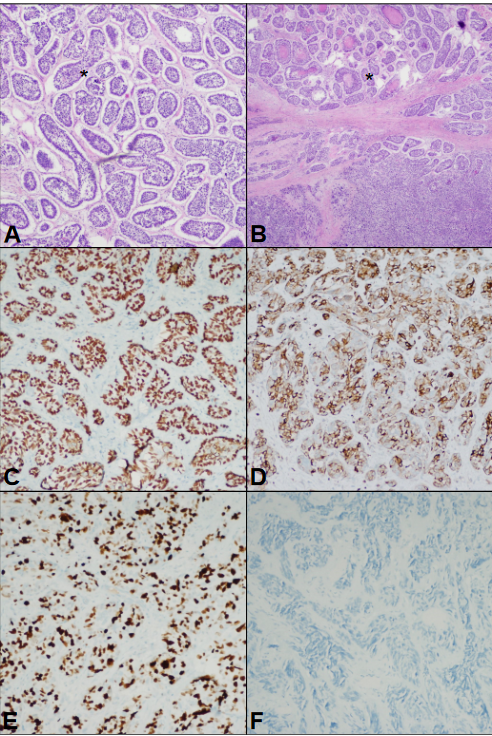
Figure 1: The biopsy and resection specimens from patient 1 demonstrated anastomosing islands of basaloid cells with peripheral palisading, stromal clefting, and desmoplastic stroma (marked with asterisk) on hematoxylin and eosin (H&E) staining (A). Focal high-grade features were noted including comedonecrosis and de-differentiation with sheet-like growth and marked pleomorphism, marked with asterisk (B). Lesional cells exhibited a staining pattern that supported basal cell carcinoma – strong nuclear positivity with p63 (C), cytoplasmic and membranous staining with BCL2 (D), markedly elevated proliferation index with Ki-67 (E), and negative PSA (F).
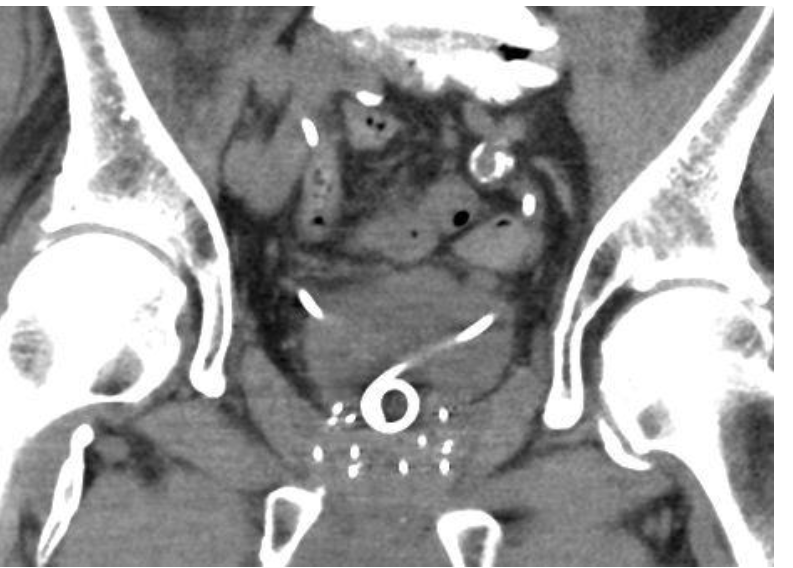
After diagnosis, post-operative staging axial imaging revealed no evidence of any metastatic disease. The patient presented nine months later with return of severe obstructive lower urinary tract symptoms and was taken back to the operating room for planned bilateral stent exchange. Intra- operatively, marked prostatic overgrowth of the trigone and ureteral orifices was again noted. Both ureteral stents were completely overgrown by prostatic tissue (Figure 2). A repeat TURP and bilateral stent exchange was performed. Tumor morphology from this TURP specimen matched that from his initial TURP, with prostatic BCC involving >98% of the submitted specimen.
The patient soon had recurrence and worsening of obstructive urinary symptoms and new obstructive bowel symptoms. Repeat axial imaging at this time revealed disease that was encroaching upon his rectum and growing into the bladder. Management options were discussed, and the patient elected to proceed with a pelvic exenteration, which he underwent one year after initial transurethral resection. In addition to the findings in the TURP, the pelvic exenteration specimen contained foci of tumor with central expansile necrosis and areas of de-differentiation with sheet-like growth, marked nuclear pleomorphism and atypical mitotic figures. Tumor extended into the bladder, seminal vesicles, and peri-rectal connective tissue. Extensive extraprostatic extension and perineural invasion was identified. No lymph nodes of 33 sampled were involved, giving a final stage of pT4N0M0. Postoperatively, the patient maintained an undetectable PSA and cross-sectional abdominopelvic imaging 3 months postoperatively showed no evidence of locally recurrent or distant metastatic disease.
Case Two
The patient is a 63-year-old Caucasian-American man with a history of intractable LUTS who presented to clinic with a PSA of <0.1 ng/mL. He underwent a TURP for obstructing BPH. Intra-operatively, prostatic hyperplasia was noted with extension into the bladder neck. Microscopic sections from the TURP specimen demonstrated anastomosing nests and cords of basaloid cells with focal peripheral palisading and some associated stromal desmoplasia (Figure 3). Focal cribriform architecture was identified, but tumor clefting was not readily present. Extensive perineural invasion was noted. By immunohistochemistry, the neoplastic cells stained BCL-2 positive and had an immunophenotype consistent with basal cell carcinoma. BCL-2 is known to be positive in basal cell carcinoma and not in benign basal cells. Tumor cells stained positively with p63 (nuclear) in the outermost cells, CK903 (cytoplasmic), and CK7 (cytoplasmic) in the inner most cells. They were negative for NKX3.1, PSA, PSAP, AMACR and ERG. They were also negative for CK20 and GATA3.
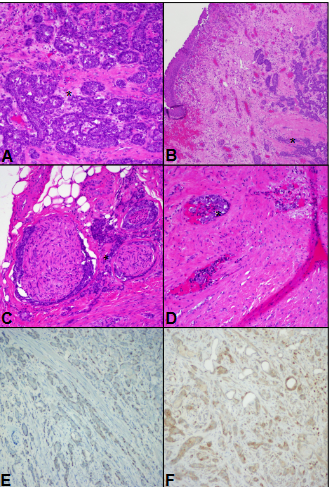
Figure 3: The biopsy and resection specimens from patient 2 exhibited anastomosing nests of hyperchromatic, basaloid cells, marked with asterisk (A), in some areas closely approaching urothelial mucosa (B). Peri-neural invasion was pervasive and involved several large-caliber nerves (C). Lymphovascular invasion was prominent, in some fields involving several adjacent blood vessels (D). Tumor cells had moderate nuclear positivity with p63 in the outermost cells (E) and cytoplasmic bcl-2 positivity (F).
After diagnosis was confirmed, post-operative staging axial imaging revealed no evidence of any metastatic disease. He was counselled extensively on treatment options and decided to pursue a radical prostatectomy. He underwent an uncomplicated robotic-assisted laparoscopic radical prostatectomy, demonstrating pT3b prostatic BCC with extra-prostatic extension, seminal vesicle invasion, lymphovascular invasion and invasion of the bladder neck. Twenty-two percent of the prostate was involved by tumor.
At his 6-month follow-up, the patient was recovering well with no evidence of any disease progression. He later moved and was lost to follow-up.
Discussion
Occurrence of prostatic BCC remains exceedingly rare, with around 100 cases documented in the literature. As with our cases, the vast majority of prostatic BCC is diagnosed in men with obstructive urinary symptoms, likely due to the tumor’s origin from the transition zone of the prostate and its local infiltrative nature. Ali et al. described the largest cohort of prostatic BCC with 29 patients [5]. They showed that these tumors predominantly are indolent with local infiltrative behavior, although a small subset behaves aggressively with local recurrences and/or distant metastases. In their cohort, most patients were managed with transurethral resection/enucleation, with only seven of the 29 patients undergoing radical prostatectomy (RP). Of these 29 patients, four developed local recurrence (two after TURP, one after enucleation, one after RP).
In addition to our two cases, a review of the literature revealed a total of 100 cases of prostatic BCC, with clinical data available for 89 cases. Of the 89 cases, 33 (37.1%) underwent RP, with three (3.3%) of those receiving pelvic exenterations. Metastasis occurred in 17 (19.1%) patients and was undetermined in 52. Nineteen (21.3%) patients had disease that remained localized. Follow-up data was available for 72 cases, for which 15 (20.8%) lived ≤1 year and only 20 (27.8%) lived ≥5 years.
Notably, our first patient was found on next generation sequencing to harbor ATM deletion. Biallelic deletions in ATM is seen in ataxia-telangiectasia syndrome, which results in progressive neurological degeneration but also is associated with immune deficiencies and increased cancer susceptibility. Leukemias and lymphomas are most commonly described [6]. Heterozygous germline deletions in ATM are reported in 0.5%-1.0% of the population and are seen in 2%-4% of men with localized prostate cancer and in up to 8% of patients with castration-resistant prostate cancers [7]. While no studies have elucidated the genomic characterization of BCC arising in the prostate, a recent evaluation of BCC on the scalp compared those which arose after radiation therapy for ringworm treatment with those which arose sporadically without any known radiation exposure. This study showed that scalp BCC arising in post- radiated patients overexpressed ATM, FOXO3a, and TNF- alpha [8]. This suggests ATM pathway deregulation may contribute to carcinogenesis in BCC following radiation exposure. Further research in prostate BCC is needed.
Unlike previously reported cases, our first case describes a patient who had prostatic BCC following radiation therapy for acinar-type prostatic adenocarcinoma. Compared to the typical behavior of prostatic BCC, this patient’s tumor was more aggressive, with rapid local recurrence that had overgrown his ureteral stents and trigone in a short period of time and encroached upon his rectum. This aggressive pattern of local recurrence and the resultant severe obstructive and irritative lower urinary tract symptoms he experienced made management problematic, and eventually the decision was made to proceed with pelvic exenteration. It is interesting to note that he had a prior history of brachytherapy for prostatic adenocarcinoma over 20 years prior to presentation and that his prostatic BCC was locally aggressive. We cannot determine with certainty whether his prior radiation may have contributed to his prostatic BCC, but it is worth noting this possibility for future management of other patients that may present in a similar fashion.
Conclusion
Around 100 cases of prostatic basal cell carcinoma are reported in the literature, and herein we have described two additional cases. To the best of our knowledge, this is the first detailed report of the diagnosis and management for prostatic BCC in a patient previously treated with brachytherapy for prostatic adenocarcinoma. ATM related mutations may contribute to certain radiation-recurrent BCC in the prostate, and this warrants further investigation. When evaluating men with obstructive lower urinary tract symptoms, particularly if those men have low PSA or if they have received prior pelvic or prostatic irradiation, BCC prostate is an important consideration in the differential diagnosis. Further study is needed to help differentiate those BCC patients with an indolent course from those with an aggressive course and surveillance with imaging is important after primary treatment.
References
-
Mattiuzzi C, Lippi G (2019) Current Cancer Epidemiology J Epidemiol Glob Health 9(4): 217-222.
-
Jemal A, Center MM, DeSantis C, Ward EM (2010) Global patterns of cancer incidence and mortality rates and trends Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol19(8): 1893- 1907.
-
Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, (2020) Campbell-Walsh-Wein Urology. In: 12th (Edn.), Elsevier.
-
Shibuya T, Takahashi G, Kan T(2019) Basal cell carcinoma of the prostate A case report and review of the literature Mol Clin Oncol 10(1): 101-104.
-
Ali TZ, Epstein JI (2007) Basal Cell Carcinoma of the Prostate A Clinicopathologic Study of 29 Cases. Am J Surg Pathol 31(5): 697-705.
-
Choi M, Kipps T, Kurzrock R (2016) ATM mutations in cancer therapeutic implications Mol Cancer Ther 15(8): 1781-1791.
-
Kaur H, Salles D, Murali S, Hicks JL, Nguyen M, et al. (2020) Genomic and clinicopathologic characterization of ATM-deficient prostate cancer Clin Cancer Res 26(18): 4869-4881.
-
Jenni R, Chikhaoui A, Nabouli I, Zaouak A, Khanchel F, et al. (2023) Differential expression of ATM NF-KB, PINK1 and FOXO3a in radiation-induced basal cell carcinoma Int J Mol Sci 24(8): 7181.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review