Is there an Association of Glycosylated Haemoglobin A1c and Anthropometric Measurements in Premenopausal and Postmenopausal Breast Cancer Patients?
Background: Breast cancer is the commonest malignancy among women globally. It is a leading cause of cancer death in less developed countries and the second leading cause of cancer death in developed countries. Diabetes and breast cancer are two conditions that frequently coexist, and menopause may be a metabolic watershed. The purpose of this study is to examine the relationship between glycosylated haemoglobin (HbA1c) and anthropometric measurements in premenopausal and postmenopausal breast cancer patients Methods: 100 patients diagnosed with breast cancer between December 2020 to November 2022 were evaluated and their HbA1c levels were correlated with anthropometric measurements and tumour characteristics Results: In our study mean age of the patients was 47.75 ±11.77 SD years. In patients with normal HbA1c 64% patients were pre-menopausal. In Pre-diabetic HbA1c group 70% were post-menopausal and in diabetic HbA1c group 93% were postmenopausal. Mean waist circumference was 84.56 ± 6.64 SD cms; more in pre-diabetic and diabetic patients; (p value 0.000). Most of the patients (71%) had waist to hip ratio ≥0.85 (p value 0.349). Pre-diabetic and diabetic patients were overweight (p value 0.000). 6 patients were known cases of type II diabetes mellitus and were on insulin/OHAs. T3 tumours were more common in both premenopausal and postmenopausal patients followed by T4 tumours. Stage IIB breast cancer was present in 39% of premenopausal and stage IIIA was seen in 30% of the postmenopausal patients. Grade II disease was more common in both premenopausal and postmenopausal (p value 0.858). Invasive ductal carcinoma-No special type (IDC-NST) was seen in 77% of the patients (p value 0.156). Estrogen Receptor (ER) positivity was seen in 42% of premenopausal and 33% of postmenopausal patients, negative Progesterone Receptor (PR) seen in 86% in premenopausal and 89% in postmenopausal patients and positive Her2 neu receptor was observed in 30% in premenopausal and 56% in postmenopausal patients. Conclusion: Our study demonstrated that a considerable proportion of breast cancer patients were prediabetic. Glycaemic status and HbA1c were clearly associated with measures of visceral obesity in carcinoma of breast patients. Postmenopausal patients had higher levels of HbA1c compared to premenopausal cases. However; clinicopathological and tumour characteristics in our study didn’t demonstrate any significant correlation with glycaemic status and need more research and randomized controlled trials. Collectively, findings from our study particularly emphasize the need to control hyperglycemia and identify vulnerable groups of breast cancer patients who might benefit from interventions to improve glycaemic control.
Introduction
The most common form of cancer among women, now days is breast cancer. It is the second most common cause of cancer death in affluent countries and a prominent cause in less developed nations. The burden differs significantly between nations and is steeply rising globally. Breast cancer incidence and mortality rates dropped in countries like the USA [1], but they are rapidly rising in China and South Korea. This difference could be explained by improved public health awareness, effective preventive measures, and more accessible healthcare. With an expected 2.3 million cases and 685,000 fatalities in 2020 [2], breast cancer has overtaken lung cancer as the most frequently diagnosed cancer for the first time. Breast cancer ranks fifth among all causes of cancer mortality globally. By 2070 cases are likely to reach 4.4 million [3]. Breast cancer ranks first for incidence and mortality in the majority of the world’s countries in 2020 [2], accounting for 24.5% of all cancer cases and 15.5% of cancer deaths. According to GLOBOCON data from 2020 [2], breast cancer caused 10.6% (90408) of all deaths in India and represented 13.5% (178361) of all cancer cases (Figures 1-17).
Increased risk factor prevalence, planned or unplanned mammographic screening detections, population increase, and ageing are all potential contributors to elevated incidence rates of breast cancer [4]. But differences in the primary risk factors, screening procedures, and population numbers or structures of different geographical locations contributed to discrepancies in the burden of breast cancer [5].
Materials and Methods
The prospective observational study was conducted at the tertiary care hospital between December 2020 and November 2022 at Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, INDIA. The study was approved by the Institutional Ethics Committee.
Study Population
Adult females with a breast cancer diagnosis who were older than 18 years old were enrolled in the study. The histopathologic examination of the excised tumour was used to make the diagnosis of breast cancer. 100 patients with breast cancer were included and their anthropometric measurements were recorded and post operatively their tumour characteristics were recorded. All patients were informed about the study’s objectives, methodology, and protocol before being interviewed. Prior to data collection, each participant signed a written informed consent form.
Data Collection
The data collection form was created, adjusted, and based on earlier studies that had been published. Anthropometric measurements for body height (cm), weight (kg), waist circumference (cm) and hip circumference (cm) were recorded at presentation according to recommendations by World Health Organization (WHO) [6]. Visceral obesity was assessed by measuring the waist circumference and the waist-hip ratio, which was obtained by dividing the waist circumference by the hip circumference. If the waist measurement was 80 cm or greater, it was considered to be central obesity [6]. The standard approach, which divides the weight in kilogrammes by the square of the height in metres, was used to determine the body mass index (BMI) [7] in patients. Patients were divided into groups based on WHO classification of BMI as follows: underweight (<18.5 kg/m2), normal (18.5–24.99 kg/m2), overweight (25.00–29.99 kg/ m2) and obese (≥30.00 kg/m2). In terms of menopausal status, patients were deemed postmenopausal if they indicated that they had been in the physiological menopause for at least a year. Patients were deemed diabetic if their laboratory findings indicated a diabetic state or if they had a confirmed diagnosis of diabetes and were receiving treatment with insulin and/or oral hypoglycemic medications when they presented. The American Joint Committee on Cancer’s (AJCC) tumor-node-metastasis (TNM) cancer staging approach was used to determine the clinical stage. Tumour characteristics for the patients were collected. Lymphovascular invasion (LVI), grade of tumour, stage, ipsilateral axillary lymph node status, and specific histological criteria were all included in the reports. Immunohistochemical techniques were used to assess the expression status of the progesterone receptor (PR) and the oestrogen receptor (ER). The Nottingham Combined Histologic Grade method was used to assess the grade of the tumour. Grading of tumours into Grade I (well-differentiated/ low grade), Grade II (moderately differentiated/intermediate grade), and Grade III (poorly differentiated/high grade) carcinomas was done in accordance with this. EDTA tubes were used to collect blood samples after venipuncture of the forearm’s antecubital vein for calculation of HbA1c.
Patients were categorised as normal/non-diabetic (HbA1c <5.7%), prediabetic (HbA1c 5.7-6.4%), and diabetic (HbA1c ≥6.5%) based on the American Diabetes Association (ADA) guidelines for HbA1c% blood levels.
Statistical Analysis
The presentation of the Categorical variables was done in the form of number and percentage (%). The data normality was checked by using Kolmogorov-Smirnov test. The cases in which the data was not normal, we used non parametric tests. The following statistical tests were applied for the results: The association of the variables which were qualitative in nature were analysed using Chi-Square test. If any cell had an expected value of less than 5 then Fisher’s exact test was used. Spearman rank correlation coefficient was used for correlation of waist circumference (cm) with HbA1c. The data entry was done in the Microsoft EXCEL spreadsheet and the final analysis was done with the use of Statistical Package for Social Sciences (SPSS) software, IBM manufacturer, Chicago, USA, version 25.0. For statistical significance, p value of less than 0.05 was considered statistically significant.
Results
The study was conducted for 23 months from December 2020 to November 2022.
Demographic and Anthropometric Characteristics in Breast Cancer Patients
The mean age of the patients was 47.75 ±11.77 SD years (range 18-80 years) with maximum number of patients (62%) belonging to 40-59 years age group. Among these patients 36 (36%) were premenopausal and 64 (64%) were postmenopausal. None of the patients had family history of breast cancer among first-degree relatives. Mean waist circumference was 84.56±6.64 SD cms. More than half of patients (71%) had waist-hip ratio equal to or more than 0.85. 47 patients (47%) were overweight and 3 patients (3%) were obese according to BMI calculated at the presentation.
| S.NO | CHARACTERISTICS | HbA1c (n = 100) | ||
|---|---|---|---|---|
| NORMAL | PRE-DIABETIC | DIABETIC | ||
| n=28 | n=58 | n=14 | ||
| 1 | AGE (years) | |||
| 47.75±11.77 SD | 39.57±11.37 SD | 51.17±11.08 SD | 49.93±6.84 SD | |
| 2 | Marital status | |||
| Single | 3 (10.7%) | 0 (0%) | 0 (0%) | |
| Married | 22 (78.6%) | 49 (84.5%) | 13 (92.9%) | |
| Widow | 3 (10.7%) | 9 (15.5%) | 1 (7.1%) | |
| 3 | Menopausal status | |||
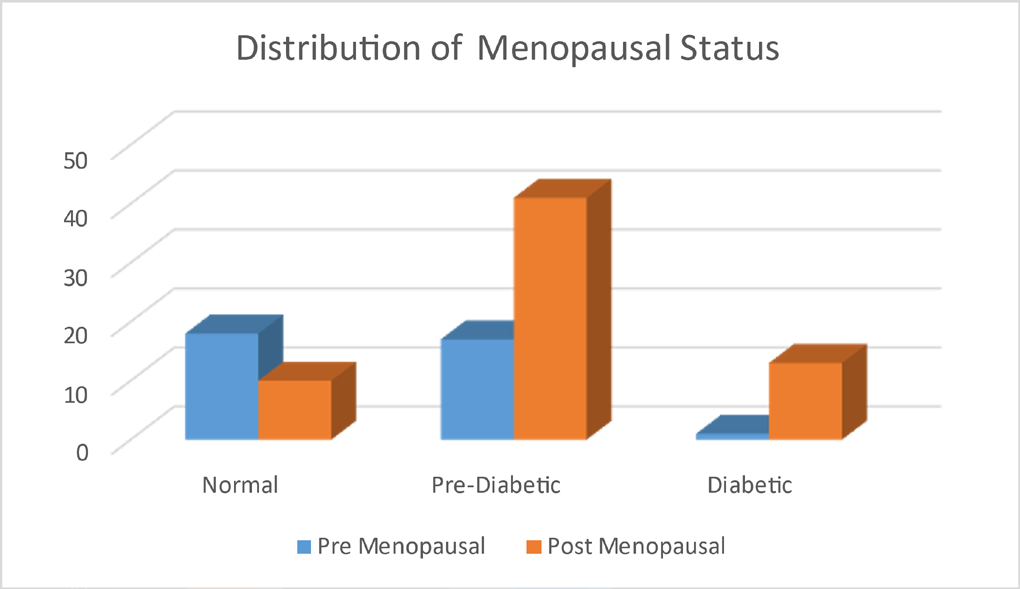
| Pre-menopausal | 18 (64.3%) | 17 (29.3%) | 1 (7.1%) | |
| Post-menopausal | 10 (35.7%) | 41 (70.7%) | 13 (92.9%) | |
| 4 | Waist Circumference (cms) 84.56 ± 6.64 SD | 79.14 ± 5.74 SD | 86.07 ± 5.55 SD | 89.14 ±6.05 SD |
| 5 | Hip Circumference (cms) 97.58 ± 6.83 SD | 91.68 ± 4.64 SD | 99.59 ± 5.59 SD | 102.71 ± 7.66 SD |
| 6 | Waist-hip ratio | |||
| <0.85 | 9 (32.1%) | 14 (24.1%) | 6 (42.9%) | |
| ≥0.85 | 19 (67.9%) | 44 (75.9%) | 8 (57.1%) | |
| 7 | BMI (Kg/m2) | |||
| Normal (18.5- 24.99) | 26 (92.9%) | 22 (37.9%) | 2 (14.3%) | |
| Overweight (25.0-29.99) | 2 (7.1%) | 35 (60.3%) | 10 (71.4%) | |
| Obese (>30) | 0 (0%) | 1 (1.7%) | 2 (14.3%) |
Table 1: Demographic and Anthropometric Characteristics of Breast Cancer Patients.
Glycemic Status and HbA1c% Levels of Breast Cancer Patients
Six patients (6%) were known cases of diabetes mellitus. All diabetics had type II disease and almost all were diagnosed after the age of 40 years (Table 2). Most diabetics received treatment regimens composed of oral hypoglycemic agents/ insulin. HbA1c % levels revealed that most patients classified as prediabetics (58%) (Table 2). Among non-diabetic/ not known cases of diabetes cases (n=94), 58 patients 61.7%) were prediabetic and 8 patients had HbA1c% levels suggestive of diabetes (8.5%).
| S.NO | CHARACTERISTICS | HbA1c (n = 100) | ||
|---|---|---|---|---|
| NORMAL | PRE-DIABETIC | DIABETIC | ||
| n=28 | n=58 | n=14 | ||
| 1 | Known case of Diabetes | |||
| Yes | 0 (0%) | 0 (0%) | 6 (42.9%) | |
| No | 28 (100%) | 58 (100%) | 8 (57.1%) | |
| 2 | Type of Diabetes | |||
| T DM 2 | 0 (0%) | 0 (0%) | 6 (42.9%) | |
| Absent | 28 (100%) | 58 (100%) | 8 (57.1%) | |
| 3 | Age at diagnosis | |||
| <40 years | 0 (0%) | 0 (0%) | 1 (7.1%) | |
| ≥ 40 years | 0 (0%) | 0 (0%) | 5 (35.7%) | |
| Not diagnosed | 28 (100%) | 58 (100%) | 8 (57.1%) | |
| 4 | Years since diagnosis | |||
| <5 years | 0 (0%) | 0 (0%) | 5 (35.7%) | |
| ≥5 years | 0 (0%) | 0 (0%) | 1 (7.1%) | |
| Not diagnosed | 28 (100%) | 58 (100%) | 8 (57.1%) | |
| 5 | Current treatment | |||
| OHAs/Insulin | 0 (0%) | 0 (0%) | 6 (42.9%) | |
| No treatment | 28 (100%) | 58 (100%) | 8 (57.1%) |
Table 2: Description of Glycemic Status and HbA1c% Levels Among Breast Cancer Patients.
Clinicopathologic Characteristics of Breast Cancer Patients
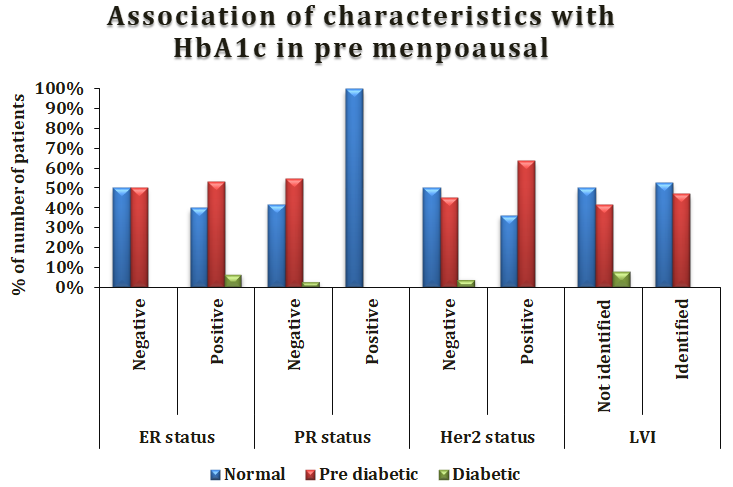
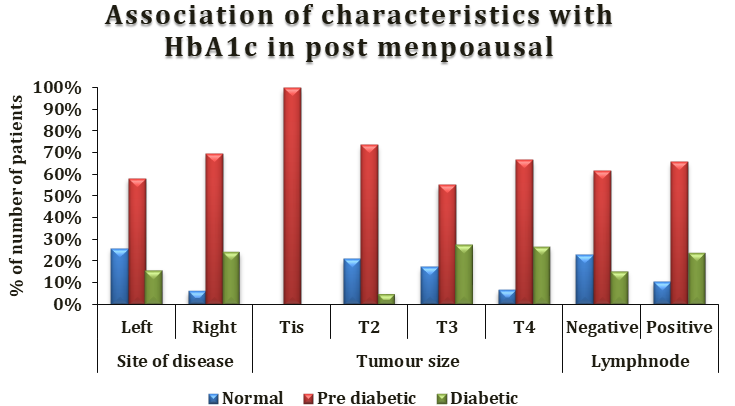
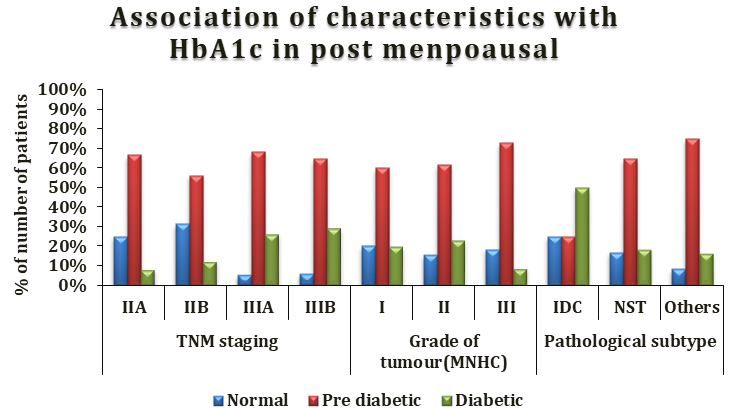
51% patients had breast cancer for less than one-year duration and were diagnosed with right-sided disease (52%) (Table 3). Most patients had stage II (43%) or stage III (56%) disease at diagnosis. More than half of patients (57%) presented with grade (II) tumour. Invasive ductal carcinoma- No Specific type (IDC-NST) was the main histopathologic type identified (77%). Most patients had negative expression of both hormones (55% for ER and 83% for PR). Her2neu expression was positive in 47% patients. All patients underwent surgical tumour resection.
| S.NO | CHARACTERISTICS | HbA1c (n = 100) | ||
|---|---|---|---|---|
| NORMAL | PRE-DIABETIC | DIABETIC | ||
| n=28 | n=58 | n=14 | ||
| 1 | Laterality/Side of disease | |||
| Right | 11 (39.3%) | 32 (55.2%) | 9 (64.3%) | |
| Left | 17 (60.7%) | 25 (43.1%) | 5 (35.7%) | |
| Bilateral | 0 (0%) | 1 (1.7%) | 0 (0%) | |
| 2 | Period with Breast cancer | |||
| <1 year | 19 (67.9%) | 30 (51.7%) | 2 (14.3%) | |
| 1-5 Years | 9 (32.1%) | 28 (48.3%) | 12 (85.7%) | |
| 3 | Tumour Size | |||
| T1 | 0 (0%) | 2 (3.4%) | 0 (0%) | |
| T2 | 4 (14.3%) | 17 (29.3%) | 2 (14.3%) | |
| T3 | 17 (60.7%) | 26 (44.8%) | 8 (57.1%) | |
| T4 | 7 (25%) | 13 (22.4%) | 4 (28.6%) | |
| 4 | Lymph Node | |||
| Positive | 12 (42.9%) | 34 (58.6%) | 10 (71.4%) | |
| Negative | 16 (57.1%) | 24 (41.4%) | 4 (28.6%) | |
| 5 | TNM Staging | |||
| Stage I | 0 (0%) | 1 (1.7%) | 0 (0%) | |
| Stage II | 14 (50%) | 25 (43.1%) | 4 (28.5%) | |
| Stage III | 14 (50%) | 32 (55.1%) | 10 (71.4%) | |
| Stage IV | 0 (0%) | 0 (0%) | 0 (0%) | |
| 6 | Grade of Tumours | |||
| Grade I | 2 (7.1%) | 9 (15.5%) | 2 (14.3%) | |
| Grade II | 17 (60.7%) | 31 (53.4%) | 9 (64.3%) | |
| Grade III | 6 (21.4%) | 11 (19%) | 1 (7.1%) | |
| Missing | 3 (10.7%) | 7 (12.1%) | 2 (14.3%) | |
| 7 | Pathological Subtypes | |||
| IDC | 2 (7.1%) | 1 (1.7%) | 3 (21.4%) | |
| ILC | 0 (0%) | 1 (1.7%) | 0 (0%) | |
| NST | 23 (82.1%) | 45 (77.6%) | 9 (64.3%) | |
| Others | 3 (10.7%) | 11 (19%) | 2 (14.3%) | |
| 8 | ER Status | |||
| Positive | 10 (35.7%) | 19 (32.8%) | 7 (50%) | |
| Negative | 14 (50%) | 35 (60.3%) | 6 (42.9%) | |
| Missing | 4 (14.3%) | 4 (6.9%) | 1 (7.1%) | |
| 9 | PR Status | |||
| Positive | 2 (7.1%) | 1 (1.7%) | 0 (0%) | |
| Negative | 22 (78.6%) | 53 (91.4%) | 13 (92.9%) | |
| Missing | 4 (14.3%) | 4 (6.9%) | 1 (7.1%) | |
| 10 | Her2 neu | |||
| Positive | 10 (35.7%) | 29 (50%) | 8 (57.1%) | |
| Negative | 14 (50%) | 25 (43.1%) | 5 (35.7%) | |
| Missing | 4 (14.3%) | 4 (6.9%) | 1 (7.1%) | |
| 11 | LVI | |||
| Identified | 11 (39.3%) | 28 (48.3%) | 6 (42.9%) | |
| Not Identified | 13 (46.4%) | 23 (39.7%) | 7 (50%) | |
| Missing | 4 (14.3%) | 7 (12.1%) | 1 (7.1%) | |
| 12 | Breast Cancer Management | |||
| Surgery | 13 (46.4%) | 30 (51.7%) | 7 (50%) | |
| Surgery + Neo Adjuvant Chemotherapy | 8 (28.6%) | 13 (22.4%) | 1 (7.1%) | |
| Surgery + Adjuvant Chemotherapy | 1 (3.6%) | 7 (12.1%) | 4 (28.6%) | |
| Surgery + Neo Adjuvant Chemotherapy + AC - Adjuvant Chemotherapy | 6 (21.4%) | 8 (13.8%) | 2 (14.3%) |
Table 3: Clinicopathologic Characteristics of Breast Cancer Patients.
Correlation between HbA1c Levels and Anthropometric Measurements of Breast Cancer Patients
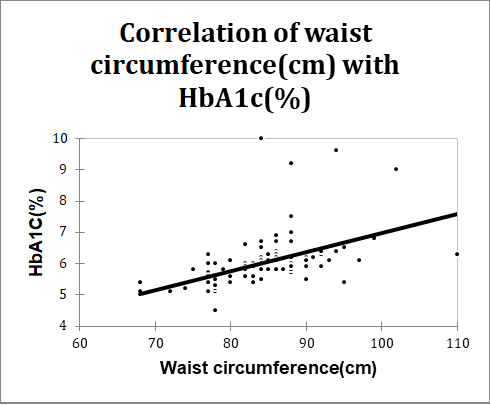
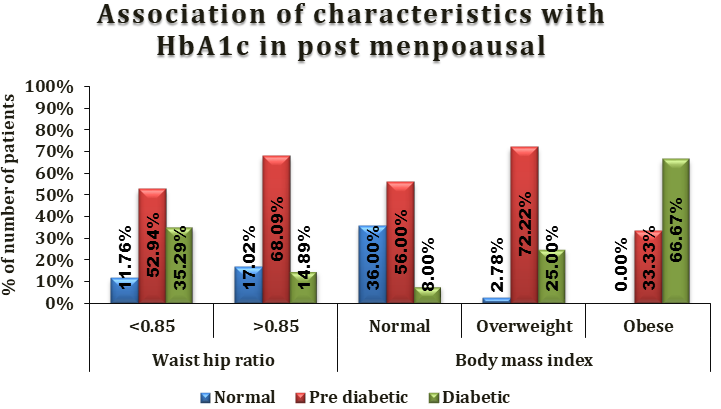
HbA1c levels were positively and significantly correlated with waist circumference (correlation coefficient 0.644, p value <0.0001) and Body mass index (p value <0.0001) respectively. However, HbA1c levels were not significantly correlated with waist to hip ratio (p value 0.315).
| Variables | HbA1c (%) |
| Waist circumference (cm) | |
|---|---|
| Correlation coefficient* | 0.644 |
| P value | <0.0001 |
| *Spearman rank correlation coefficient | |
Table 4: Correlation of waist circumference (cm) with HbA1c (%) in total study subjects.
| Characteristics | Normal | Pre diabetic | Diabetic | Total | P value |
|---|---|---|---|---|---|
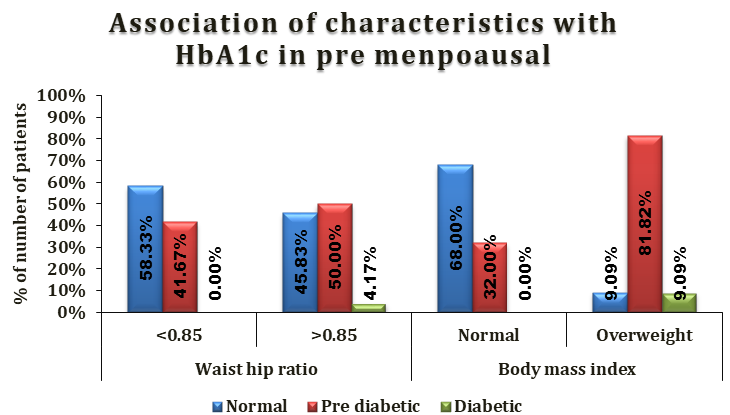
| Waist hip ratio | |||||
| <0.85 | 9 (31.03%) | 14 (48.28%) | 6 (20.69%) | 29 (100%) | 0.315* |
| >0.85 | 19 (26.76%) | 44 (61.97%) | 8 (11.27%) | 71 (100%) | |
| Body mass index | |||||
| Normal | 26 (52%) | 22 (44%) | 2 (4%) | 50 (100%) | <.0001* |
| Overweight | 2 (4.26%) | 35 (74.47%) | 10 (21.28%) | 47 (100%) | |
| Obese | 0 (0%) | 1 (33.33%) | 2 (66.67%) | 3 (100%) |
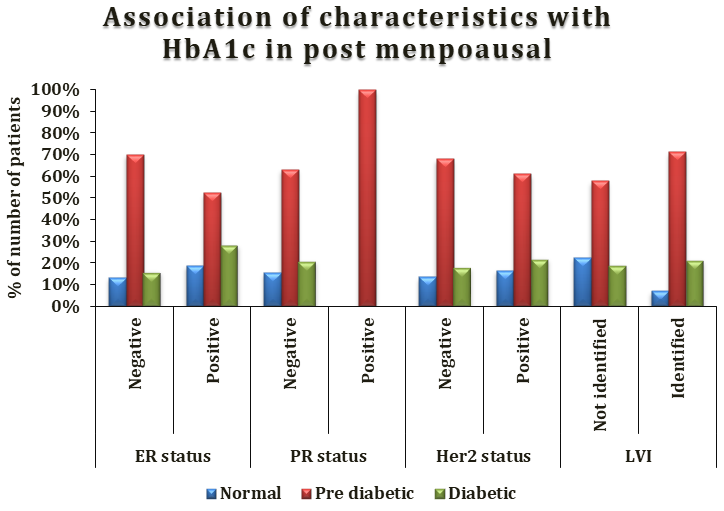
Table 5: Association of characteristics with HbA1c in total study subjects.
* Fisher’s exact test
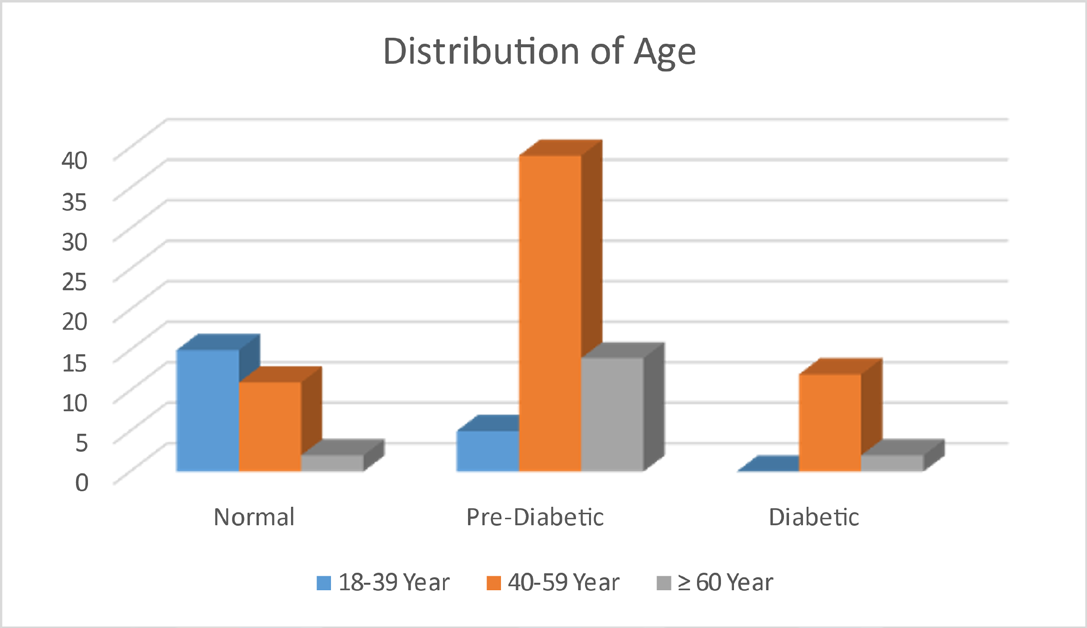
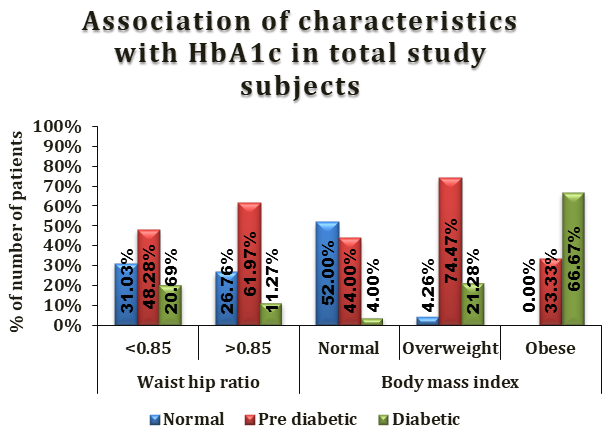
HbA1c levels were higher among elderly patients compared to other younger age groups (Figure 3). In breast cancer patients with greater waist circumference had significantly higher HbA1c levels (Figure 1). Obese and overweight patients had higher HbA1c, these differences were of statistical significance (p<0.0001) (Table 5 & Figure
4). HbA1c blood levels were significantly higher among postmenopausal compared to premenopausal patients (p=0.000) (Figure 5). Waist to hip ratio ≥0.85 was seen in
71% patients however these differences did not reach the level of statistical significance (p=0.315).
| Characteristics | Premenopausal (n=36) | Postmenopausal (n=64) | ||||||
|---|---|---|---|---|---|---|---|---|
| HbA1c status | HbA1c status | |||||||
| Normal | Prediabetic | Diabetic | p value | Normal | Prediabetic | Diabetic | p value | |
| (n=18) | (n=17) | (n=1) | (n=10) | (n=41) | (n=13) | |||
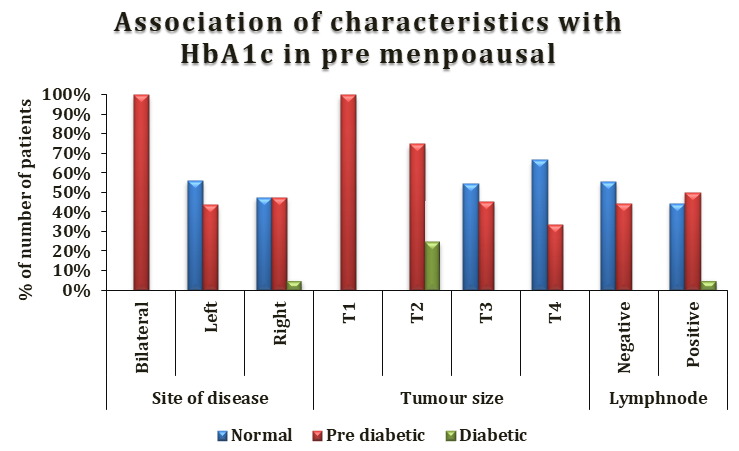
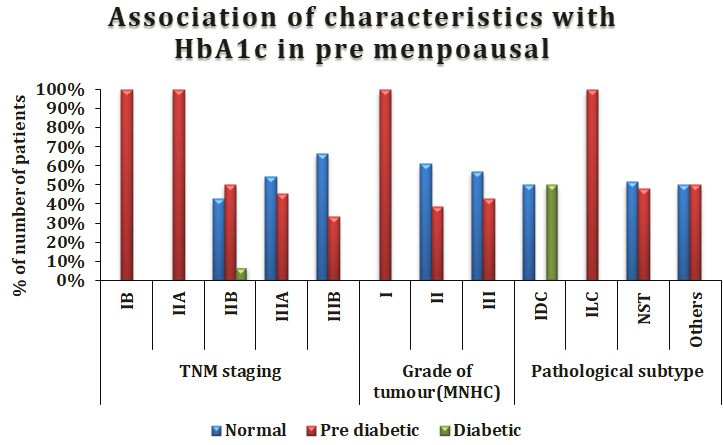
| Stage | ||||||||
| IB | 0 (0%) | 1 (100%) | 0 (0%) | 0.761* | 0.266* | |||
| IIA | 0 (0%) | 1 (100%) | 0 (0%) | 3 (25%) | 8 (66.67%) | 1 (8.33%) | ||
| IIB | 6 (42.86%) | 7 (50%) | 1 (7.14%) | 5 (31.25%) | 9 (56.25%) | 2 (12.50%) | ||
| IIIA | 6 (54.55%) | 5 (45.45%) | 0 (0%) | 1 (5.26%) | 13 (68.42%) | 5 (26.32%) | ||
| IIIB | 6 (66.67%) | 3 (33.33%) | 0 (0%) | 1 (5.88%) | 11 (64.71%) | 5 (29.41%) | ||
| Grade | ||||||||
| I | 0 (0%) | 3 (100%) | 0(0%) | 0.202* | 2 (20%) | 6 (60%) | 2 (20%) | 0.908* |
| II | 11 (61.11%) | 7 (38.89%) | 0(0%) | 6 (15.38%) | 24 (61.54%) | 9 (23.08%) | ||
| III | 4 (57.14%) | 3 (42.86%) | 0(0%) | 2 (18.18%) | 8 (72.73%) | 1 (9.09%) | ||
| ER status | ||||||||
| Negative | 9 (50%) | 9 (50%) | 0 (0%) | 0.608* | 5 (13.51%) | 26 (70.27%) | 6 (16.22%) | 0.383* |
| Positive | 6 (40%) | 8 (53.33%) | 1 (6.67%) | 4 (19.05%) | 11 (52.38%) | 6 (28.57%) | ||
| PR status | ||||||||
| Negative | 13 (41.94%) | 17 (54.84%) | 1 (3.23%) | 0.259* | 9 (15.79%) | 36 (63.16%) | 12 (21.05%) | 1* |
| Positive | 2 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (100%) | 0 (0%) | ||
| Her2 neu status | ||||||||
| Negative | 11 (50%) | 10 (45.45%) | 1 (4.55%) | 0.648* | 3 (13.64%) | 15 (68.18%) | 4 (18.18%) | 0.928* |
| Positive | 4 (36.36%) | 7 (63.64%) | 0 (0%) | 6 (16.67%) | 22 (61.11%) | 8 (22.22%) | ||
| LVI | ||||||||
| Not Identified | 6 (50%) | 5 (41.67%) | 1 (8.33%) | 0.675* | 7 (22.58%) | 18 (58.06%) | 6 (19.35%) | 0.285* |
| Identified | 9 (52.94%) | 8 (47.06%) | 0 (0%) | 2 (7.14%) | 20 (71.43%) | 6 (21.43%) |
Table 6: Association Between HbA1c with Clinicopathologic Characteristics in Breast Cancer Patients Based on Menopausal Status (n
* Fisher’s exact test
Discussion
Glycosylated haemoglobin A1c (HbA1c) tests were adopted as a diagnostic tool for diabetes by the American Diabetes Association (ADA) [8]. The chronic glycemic exposure marker HbA1c shows the average blood glucose levels over a period of two to three months [8, 9]. Overall breast carcinoma is the 2nd most common malignancy seen worldwide and the most common malignancy in females. Over hundred years the associations of breast carcinoma with other co-morbidities were being studied to identify various etiologies and associated morbidity and mortality. This study was undertaken with the aim to study the association of glycosylated haemoglobin A1c with anthropometric measurements & tumour characteristics in carcinoma breast. Results from our study showed that prediabetic patients with no history of diabetes made up the majority of the breast cancer patients in this series. This is especially interesting because prior research suggested that many diabetes cases would go untreated until a breast cancer diagnosis was obtained. In our study the mean age was 47.75±11.77 SD years. The youngest was 18 years old and eldest was 80 years all of whom were females. In our study maximum patients 62% belonged to 40-59 years age group (p value 0.069) which not statistically significant. 84 (84%) patients were married and 13 (13%) patients were widow and only 3 (3%) were single. Our study is in agreement with study of Nehad M Ayoub, et al. [10] average age of the patients was 49.9±10.3 SD years (range 27 to 80 years). In their study maximum patients 62.3% belonged to 40-59 years age group. 74% patients were married 16.6% were widow and 8.5% were single. In our study 36 (36%) patients were pre-menopausal and 64 (64%) patients were post-menopausal. In pre-diabetic group 70% patients were postmenopausal and in diabetic group 93% patients were postmenopausal. In the study by Nehad M Ayoub, et al. [10] 32% patients were pre-menopausal and 67.7% were post-menopausal. Study indicated a significant association between HbA1c and menopausal status. Postmenopausal women presented with higher mean levels of HbA1c
compared to premenopausal patients. The results were similar and comparable to our study. In our study HbA1c levels were positively and significantly correlated with waist circumference, hip circumference and BMI but were not significantly correlated with waist to hip ratio. In agreement to our findings Million Women Study [11] which followed 1.2 million UK women aged 50 to 64 years for a mean of 5.4 years, including 45,037 with breast cancer, and identified a nearly 30% higher risk of developing postmenopausal breast cancer with obesity. An increased risk of breast cancer in postmenopausal women with diabetes was reported in study by Talamini, et al. [12]. Our findings revealed that on the basis of HbA1c % levels, most patients were classified as prediabetics (58%). In agreement with study of Nehad M Ayoub, et al. [10] HbA1c % levels revealed that most patients classified as prediabetics (44.4%). 6% patients in our study were known cases of diabetes. Our study is in agreement with the study of Juhua Luo, et al. [13] of women with invasive breast cancer, in which 9.0 % had pre-existing treated diabetes before breast cancer diagnosis. In our study 52 (52%) patients had right sided disease, 47 (47%) had left sided disease and 1 (1%) patient had bilateral disease (p value 0.434) which was not statistically significant. Our study is in agreement with study of Shao-Ang Cheng, et al. [14] in the case of invasive carcinoma of breast. The right breast was more commonly affected than the left in young (<40 years old) patients whereas the opposite trend was found in old (≥40 years old) patients. In our study 2 (2%) patient had T1 tumour; 23 (23%) patients had T2 tumour; 51 (51%) had T3 tumour; and rest 24 (24%) had T4 tumour. 56% patients had clinically palpable lymph nodes while 44% did not. In this study 1% had stage I carcinoma of breast; 43% had stage II and 56% had stage III carcinoma of breast. Most of the pre-diabetic and diabetic patients had stage III breast cancer (55.1% and 56% respectively) with p value 0.879 which was not statistically significant. In this study pathological grading of disease was done by Nottingham histological grading system. 13% patients had grade I; 57% had grade II and 18% had grade III disease. Maximum patients were seen as grade II in pre-diabetic and diabetic HbA1c patients (53.4% and 64.3% respectively; p value 0.858) which was not statistically significant. In pre- diabetic and diabetic patients lymphovascular invasion was identified in 48.3% and 42.9%, respectively; (p value 0.888) which was not statistically significant. 77 (77%) patients had invasive ductal carcinoma – no special type (NST) as breast carcinoma subtype which failed to exhibit sufficient morphological features to be classified as specific histological types. Our study is in agreement with study of Barbara, et al. [15] grading which showed that most tumours were moderately differentiated, i.e., grade II in 67 patients (73%) and were followed by low-differentiated, i.e., grade III in 19 patients (21%); (p value 0.0698). Our study is in agreement with study of the Bronsveld, et al. [16] in which they did not find an association between any of the clinicopathological breast cancer subtypes and diabetes in postmenopausal breast cancer patients compared to the non-diabetic. Our study is in agreement with study of Yancik, et al. [17] in which there was no association seen between diabetes and breast cancer stage in menopausal women. Our study deviates from the study of Fleming, et al. [18] which evaluated women older than 67 years with breast cancer using Surveillance, Epidemiology, and End Results-Medicare data and found an increased risk of late-stage disease in women with diabetes. Our study differs from the study of Srokowski, et al. [19] which demonstrated that a higher percentage of women with diabetes presented with a more advanced stage than their nondiabetic counterparts. In our study 36 (36%) patients had positive ER status; while 55 (55%) had negative ER status. In pre-diabetic and diabetic patients; 60.3% and 42.9% had negative ER status respectively (p value 0.567). In our study 88 (88%) patients had negative PR status. In our study 47 (47%) patients had positive Her2 neu receptor status and 44 (44%) had negative Her2 neu. In pre-diabetic and diabetic 50% and 57.1% had positive Her2 neu status respectively; (p value 0.585). In agreement to our study Karlin, et al. [20] also reported no significant differences in breast cancer grade, stage, and receptor positivity between diabetic and non-diabetic patients. In contrast to our study Julie R. Palmer, et al. [21] demonstrated positive association with diabetes for ER negative breast cancer but not for ER positive cancer. The impact of HbA1c on breast clinicopathologic characteristics was inconsistent. HbA1c status in this study did not significantly correlate with tumour clinicopathologic features.
Conclusion
Our study demonstrated that a considerable proportion of breast cancer patients in this study were prediabetic. Glycaemic status and HbA1c was clearly associated with measures of visceral obesity in carcinoma of breast patients. Postmenopausal patients in this study had higher levels of HbA1c compared to premenopausal cases. However; clinicopathological and tumour characteristics in our study didn’t demonstrate any significant correlation with glycaemic status and need more research and randomized controlled trials. Collectively, findings from our study call for appropriate assessment for glycaemic status in breast cancer patients on presentation, particularly emphasizing the need to control hyperglycemia and identify vulnerable groups of breast cancer patients who might benefit from interventions to improve glycaemic control.
Ethical Approval
The study was approved by the Jawaharlal Nehru Medical College and Hospital Institutional Ethics Committee.
References
-
Lei S, Zheng R, Zhang S, Wang S, Chen R, et al. (2021) Global patterns of breast cancer incidence and mortality: A population‐based cancer registry data analysis from 2000 to 2020. Cancer Communications 41(11): 1183- 1194.
-
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, et al. (2021)Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians 71(3): 209-249.
-
Soerjomataram I, Bray F (2021) Planning for tomorrow: Global cancer incidence and the role of prevention 2020–2070. Nature reviews Clinical oncology 18(10): 663-672.
-
Britt KL, Cuzick J, Phillips KA (2020) Key steps for effective breast cancer prevention. Nature Reviews Cancer.20(8): 417-436.
-
Gaudet MM, Gierach GL, Carter BD, Luo J, Milne RL, et al. (2018)Pooled Analysis of Nine Cohorts Reveals Breast Cancer Risk Factors by Tumor Molecular Subtype Breast Cancer Risk Factors by Tumor Molecular Subtypes. Cancer research.78(20): 6011- 6021.
-
Nishida C, Ko GT, Kumanyika S (2010) Body fat distribution and noncommunicable diseases in populations: overview of the 2008 WHO Expert Consultation on Waist Circumference and Waist-Hip Ratio. Eur J Clin Nutr 64(1): 2-5.
-
(2000) Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser 894: 1-253.
-
American Diabetes Association (2023) Diagnosis. Diabetes overview.
-
Nathan DM (2009) International expert committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 32(7): 1327-1334.
-
Ayoub NM, Jaradat SK, Alhusban A, Tahaineh L (2020) Glycosylated Hemoglobin A1c Is Associated with Anthropometric Measurements and Tumor Characteristics in Breast Cancer Patients. Int J Womens Health 12: 139-149.
-
Million Women Study Collaborative Group (1999) The Million Women Study: design and characteristics of the study population. Breast Cancer Res 1(1): 73-80.
-
Talamini R, Franceschi S, Favero A, Negri E, Parazzini F, et al. (1997) Selected medical conditions and risk of breast cancer. Br J Cancer 75(11): 1699-1703.
-
Luo J, Virnig B, Hendryx M, Wen S, Chelebowski R, et al. (2014) Diabetes, diabetes treatment and breast cancer prognosis. Breast Cancer Res Treat 148(1): 153-162.
-
Cheng SA, Liang LZ, Liang QL, Huang ZY, Peng XX, et al. (2018) Breast cancer laterality and molecular subtype likely share a common risk factor. Cancer Manag Res 10: 6549-6554.
-
Barbara RC, Piotr R, Kornel B ,Elżbieta Z, Danuta R, et al. (2020) Divergent Impact of Breast Cancer Laterality on Clinicopathological, Angiogenic, and Hemostatic Profiles: A Potential Role of Tumor Localization in Future Outcomes. J Clin Med 9(6): 1708.
-
Bronsveld HK, Jensen V, Vahl P, De Bruin ML ,Cornelissen S, et al. (2017) Diabetes and Breast Cancer Subtypes. PLoS One 12(1):e0170084.
-
Yancik R, Wesley MN, Ries LA , Havlik RJ, Edwards BK, et al. (2001) Effect of age and comorbidity in postmenopausal breast cancer patients aged 55 years and older. Jama 285(7): 885-892.
-
Fleming ST, Pursley HG, Newman B , Pavlov D, Chen K (2005) Comorbidity as a predictor of stage of illness for patients with breast cancer. Med Care 43(2): 132-140.
-
Srokowski TP, Fang S, Hortobagy GN , Sharon HG (2009) Impact of diabetes mellitus on complications and outcomes of adjuvant chemotherapy in older patients with breast cancer. J Clin Oncol 27(13): 2170-2176.
-
Karlin NJ, Dueck AC, Reddy SK, Verona PM , CCook CB (2014) Implications of breast cancer with diabetes mellitus on patient outcomes and care. Diabetes Management 4(5): 411.
-
Palmer JR, Castro-Webb N, Bertrand K, Bethea TN , Denis GV (2017) Type II Diabetes and Incidence of Estrogen Receptor Negative Breast Cancer in African American Women. Cancer Res 77(22): 6462-6469.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review