Assessing the Management of Varicose Vein Using Individualized Medicine: An Empirical Study
Varicose vein is one of the most common clinical condition presented by abnormal blood flow in the lower extremities and it remains an open question as to which inciting factor is responsible for their development, if any one particular factor is in fact solely responsible. It is unclear whether local dysfunction in the vein wall leads to valvular incompetence or whether the reverse is true. The abnormal vessel of the varicosity is invariably dilated, and luminal diameter is larger than in normal vein. Importantly, varicose vein disease is characterized by skip lesions, areas of normal vein between varicosities. Homoeopathy is a complementary system of medicine that follows a holistic approach. Homeopathy follows a personalized approach in treatment of chronic disease such as varicose veins Here 30 cases of varicose vein was used for the study and in each case complete case taking was done and after evaluated using Revised Venous Clinical Severity Score an and medicine was selected according to the totality. Potency and dose was determined based on the susceptibility of the patient. Follow up was done. Since p value <0.05, it indicates that the test is statistically significant and hence the null hypothesis is rejected.
Introduction
Varicose veins significantly reduce quality of life, whereas their operative treatment demonstrably improves quality of life [1]. About half of women and a third of men were found to have varicose veins in the northern Indian population. 47.3% of women and 27.8% of men is found to be suffering from varicose vein, while venous symptoms were present in 49.3% of women and 18.9% of men. In 18.9% of females and 5.2% of males, skin trophic alterations were seen [2]. Its high prevalence and associated consequences, such chronic venous ulcers, place a significant burden on social systems and healthcare systems [3]. Alteration of the vessel wall along with valve has been found as one of the major pathology in most of the cases of varicose vein. Obesity, blood pressure, lifestyle, and nutritional factors are all modifiable factors that have been demonstrated to affect vascular health and to be linked to vascular-related disorders. Age, sex (more common in women), obesity, pregnancy, and prior deep vein thrombosis have all been linked in epidemiological studies to an increased incidence of varicose veins [3].
Varicose veins are frequently referred to as a “Western” ailment as it is one of the emerging diseases found mainly in developing countries. Varicose vein occurrence varies greatly between different parts of the world, according to epidemiological studies [4]. Adults might have varicose veins at varying rates, ranging from 10% to 60% [5]. Although venous varicosities are frequently thought of as a cosmetic issue, the majority of instances are accompanied by varied degrees of discomfort, including heaviness, soreness, swelling, cramps, and increased tiredness. In a bigger Scale, varicose veins are actually just one aspect of a spectrum of alterations brought on by chronic venous insufficiency, which can include anything from simple telangiectasia (spider veins) to venous ulcers [6]. Varicose veins’ etiology is still poorly understood. The first theories, which were simply mechanical in nature, have given way in the last ten years to concepts that center on intricate molecular and histopathologic changes in the extracellular matrix (ECM) and vessel wall. The histopathologic changes are uniformly present, while pathologic mechanical variables such valve incompetence and venous hypertension are not always present. However, because valve dysfunction and venous hypertension are typically present, these mechanical aspects are likely to affect the disease’s severity [6]. Varicose veins appear differently clinically depending onthepatient.
Common lower limb symptoms usually include heaviness, swelling, soreness, cramping or itching are much more frequently reported by women than by men [7]. Skin changes, corona phlebectatica, a higher BMI, and popliteal vein discomfort, restless legs, cramping, or itching are significant risk factors for the evolution of varicose vein towards varicose leg ulcer [8]. Some people show no symptoms. If symptoms are present, they are typically restricted to the varicose vein-affected area, though they may become more widespread to affect the entire lower extremity. There may be discomfort, burning, or itching in a specific area. Leg aches, weariness, or swelling are examples of general symptoms. The symptoms normally get better at night, especially after lengthy hours of standing, and go away when the patient sits and elevates their legs.
Homoeopathy is a complementary system of medicine that follows a holistic approach. Homeopathy follows a personalized approach in treatment of chronic disease such as varicose veins. It is highly precise and has proved to be effective in alleviating the symptomatology. The potency to be administered in each case is selected based on the susceptibility of the individual. In acute case, if the prescriber has studied the case very carefully at the beginning, not only the presenting symptoms but also the past history of the patient, a single antipsoric might have sufficed the case. But in chronic disease may be incurable except by an anti-psoric, anti-syphilitic or anti- Sycotic [9].
Materials and Methods
A sample size of 30cases having the symptomatology of varicose vein was randomly selected from the OPD and IPD of Sarada Krishna Homoeopathic medical college and hospital. The details of the case already recorded from the patient in standardized pre-structured case format of Sarada Krishna Homoeopathic Medical College & Hospital. Patients between the age group of 20 and 85 years old and those who expressed the symptomatology that is pain and edema of the lower extremities was selected for the study. Those patients having serious comorbidities was excluded from the study. The case was analyzed and totality erected. Evaluation of the symptoms was done followed by repertorisation and a suitable similimum is selected. Patients who are pregnant and those having serious comorbidities was excluded from the study. Outcome was evaluated using Revised Venous Clinical Severity Score.
Inclusion Criteria
Age group of 20 - 85 years, Patients diagnosed with varicose vein of lower extremities and from both sexes.
Exclusion Criteria
Patients with age less than 20 years and more than 85 years, Patient with other serious co-morbidities, Patients who are pregnant.
Statistical Methods and Analysis of Data
The Revised Venous Clinical Severity Score was used to test the hypothesis. Observed data was represented by tabular and graphical representation. Hypothesis was tested using paired ‘t’ test.
Results
Cases were examined, totalities constructed in accordance with homoeopathic principles, symptoms were assessed, and clinical evaluations was done using the Revised Venous Clinical Severity Score. The significance was examined using the paired T test. Since the p-value < α, H0 is rejected. The After population’s average is considered to be not equal to the Before population’s average. In other words, the sample difference between the averages of After and Before is big enough to be statistically significant thus showing the effectiveness of homoeopathy in the management of varicose vein (Table 1).
- MEAN
- STANDARD DEVIATION
- MEAN DIFFERENCE (95% CI) t- statistic (df)
- P Value
- PRE
- POST
- PRE
- POST
- 16.8
- 13.8
- 2.4
- 2.7
- 1.34
- 11.2604
- 2.774
Table 1: Comparison of Pre- and post- treatment value.
Discussion
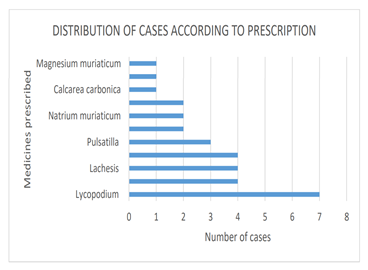
Many study have shown the different socioeconomic factors influencing the occurrence of varicose vein. Previous studies have shown that varicose vein tend to occur more commonly in males than females [10]. In this study also 83% of the affected individuals were male. Another finding is that the most commonly affected individuals belong to the age group of 40- 51 years. Other studies also support this evidence [10]. The most commonly prescribed medicine was Lycopodium clavatum [11, 12] ( in 23 % cases ) followed by Sulphur, Lachesis and Rhus toxicodendron in 13%, Pulsatilla nigricans in 10 % cases, Arsenicum album, Natrium muriaticum and Vipera in 6% of cases, Calcarea carbonica, Apis mellifica and Magnesium muriaticum in 3.33 % of cases [13] (Figure 1).
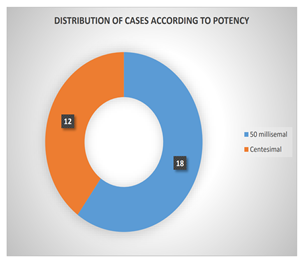
Out of 30 cases, 60% was given medicine in LM potency and 40% in Centesimal potency [14] (Figure 2). Hence LM potency is considered to be more better in alleviating pain than Centesimal potency [15].
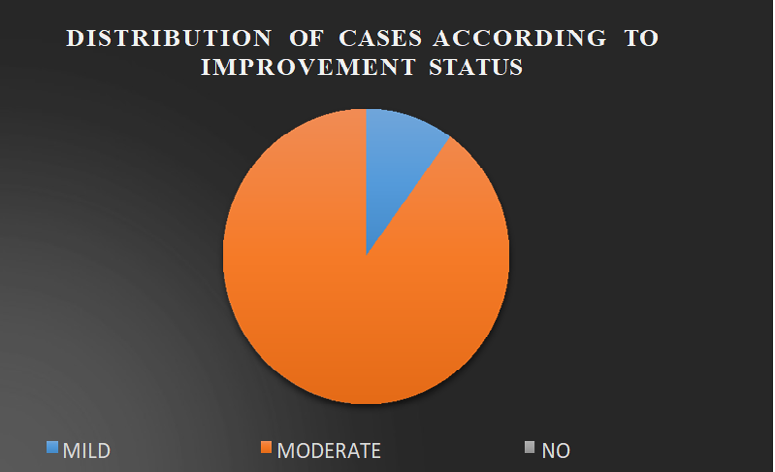
In this study, 90 % of cases showed moderate improvement in their symptomatology and 10% showed mild improvement in their symptomatology after intervention using individualized medicine (Figure 3).
Conclusion
Varicose vein is said to be one of the most chronic diseases that affects the quality of life of the patients. With this study we may conclude that homoeopathy was found to be efficient in the management of symptoms of varicose vein. Homoeopathy is one of the most available systems of medicine which will not impose a financial liability upon the patient or the society. Moreover, the patient will not have to face any adverse side effects to the treatment provided.
References
-
Brar R, Nordon IM, Hinchliffe RJ, Loftus IM, Thompson MM (2010) Surgical management of varicose veins: meta-analysis Vascular 18(4): 205-220.
-
Agarwal V, Agarwal S, Singh A, Nathwani P, Goyal P, et al. (2016) Prevalence and risk factors of varicose veins, skin trophic changes, and venous symptoms among northern Indian population. Int J Res Med Sci 4(5): 1678-1682.
-
Yuan S, Bruzelius M, Damrauer SM, Larsson SC (2021) Cardiometabolic, lifestyle, and nutritional factors in relation to varicose veins: a Mendelian randomization study. Journal of the American Heart Association10(21): e022286.
-
Darwood RJ, Theivacumar N, Dellagrammaticas D, Mavor AI, Gough MJ (2008) Randomized clinical trial comparing endovenous laser ablation with surgery for the treatment of primary great saphenous varicose veins. Journal of British Surgery 95(3): 294-301.
-
Dalboh A, Alshehri NA, Alrafie AA, Bakri KA (2020) Prevalence and awareness of varicose veins among teachers in Abha, Saudi Arabia. Journal of Family Medicine and Primary Care 9(9): 4784-4787.
-
Oklu R, Habito R, Mayr M, Deipolyi AR, Albadawi H, et al. (2012) Pathogenesis of Varicose Veins. Journal of Vascular Interventional Radiololgy 23(1): 33-39.
-
Jones RH, Carek PJ (2008) Management of varicose veins. American family physician 78(11): 1289-1294.
-
Pannier FA, Rabe E (2015) Progression in venous pathology. Phlebology 30(1suppl): 95-7.
-
Dunham C (2007) The Science of Theurapeutics. In: 1st (Edn.), Alteration and succession, pp: 157- 226**.**
-
Bahk JW, Kim H, Jung-Choi K, Jung MC, Lee I (2012) Relationship between prolonged standing and symptoms of varicose veins and nocturnal leg cramps among women and men. Ergonomics 55(2): 133-139.
-
Banerjee J, Biswas S, Madhu NR, Karmakar SR, Biswas SJ (2014) A better understanding of pharmacological activities and uses of phytochemicals of Lycopodium clavatum: A review. Journal of pharmacognosy and phytochemistry 3(1): 207-210.
-
Lorenzetti E, Treib EL, Heling AL, Coltro-Roncato S, Carvalho JC, et al. (2016) Antimicrobial action against of Macrophomina phaseolina and control of the grey stem in soybean by homeopathic remedies Nosode and Sulphur. African Journal of Agricultural Research 11(36): 3412-3417.
-
Boericke W (2010) Boericke’s New Manual of Homeopathic Materia Medica with Repertory. 3rd edition. New Delhi, Large Print, India.
-
Hahnemann S (2021) Organon of medicine: Sixth edition. New Delhi, India.
-
Nayak C, Singh V, Gupta J, Ali M, Pal R, et al. (2012) Homoeopathic individualized LM-potencies versus Centesimal potencies for pain management of cervical spondylosis: A multicenter prospective randomized exploratory clinical study. Central Council for Research in Homoeopathy 6(4): 16-23.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review