Symptomatic Adnexal Cyst with Pregnancy – Laparoscopic Management with a Surprise Revelation
Large cystic masses are rare in pregnancy and are usually ovarian cysts [1]. Surgical removal of the cyst can be performed electively in the 2nd trimester or at any time if acute symptoms are present. In this case report, we present the case of a pregnant women who presented with a symptomatic cyst which was reported as an adnexal cyst on imaging. Preoperatively it was found to be arising from the mesentery of the transverse colon. Histopathological examination was consistent with benign mesenteric cyst.
Introduction
Large cystic masses are infrequent in pregnancy and are more commonly ovarian cysts. Rarely it can be a mesenteric cyst. Mesenteric cysts are benign abdominal lesions that possess the risk of malignant transformation in 3% of reported cases [2, 3, 4, 5]. They most commonly present with variable and nonspecific symptoms; 40% of cases are incidental findings during physical examinations or imaging procedures [3, 4]. They present in the first decade of life and possess a 1:1 male: female ratio.
Case Report
In this report we present a case of a 30-year-old patient G4P3L3 at 12 weeks period of gestation who presented to our emergency department with complaint of pain abdomen for 2 days.
Pain was acute, gradual in onset, progressive in nature, sharp aching, non-radiating, aggravated on doing some physical activity and relieved after taking rest. Pain was associated with vomiting, which was non projectile and non- bilious. Bowel and bladder habits were normal.
She had history of previous 3 full term normal vaginal deliveries. No significant past/personal/family history. On examination, her vitals were stable. Per abdominal examination revealed a soft, 12x12cm tender cystic mass in right iliac fossa extending to right lumbar region. The lower limit of the cyst could be reached, and the overlying skin was normal. On per speculum examination, cervix and vagina were healthy. Per vaginal examination revealed uterus enlarged to 10–12-week gravid uterus size and bilateral fornices were free. Same mass was felt high up tipped through the right fornix without any tenderness.
Ultrasound revealed a single live intrauterine fetus of 11week 2 days. Right adnexa showed a multiloculated cystic lesion measuring 9.4x8.4x8.7 cm with no solid component or septal vascularity. Pedicle vascularity was maintained and right ovary wasn’t visualized separately. A provisional diagnosis of right ovarian serous cystadenoma was made based on the findings.
After counseling and honoring the wishes of the patient, surgical termination of pregnancy and Copper T 380 A (Intra uterine contraceptive device) insertion with diagnostic laparoscopy was done.
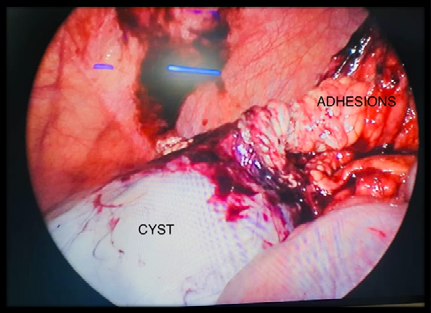
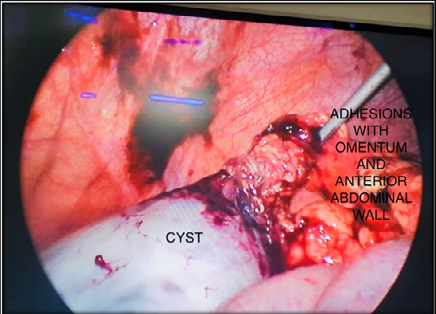
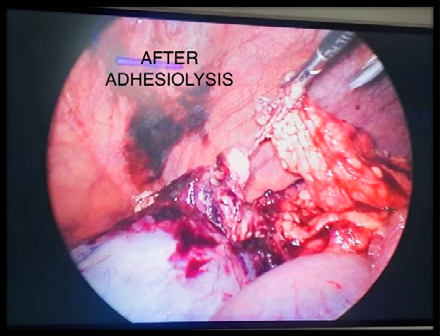
Per-operatively, a large cyst was found partially adherent to the anterior abdominal wall covered with omentum. After adhesiolysis, the tubes and ovaries were found to be normal with no attachment to the cyst. The cyst was arising from the mesentery of the transverse colon with 2 twists at the base. Complete excision of the cyst was done after dividing the pedicle and cyst wall removed after aspiration of cyst fluid.
Post-operative period was uneventful and the patient was discharged on day 3 in stable condition.
Histopathological findings were consistent with benign mesenteric cyst.
Patient was seen at the follow up clinic and was doing fine.
Discussion
Mesenteric cyst is a rare cause of abdominal pain and can arise from the mesentery of the duodenum to the sigmoid colon. The incidence varies from 1/105,000–250,000 in admitted surgical patients. Mesenteric cyst can be simple or multiple, unilocular or multilocular, and may contain hemorrhagic, serous, chylous, or infected fluid. They range in size from 3cm to 30cm in diameter. The most accepted theory about the aetiology of mesenteric cysts is benign ectopic lymphatic proliferation in the mesentery that are not related to other parts of the mesenteric system [6]. More than half of the cysts are found in the small bowel mesentery, and particularly are seen in the ileum. Diagnosis of mesenteric cyst is made by ultrasonography. MRI is preferred over Ultrasound. Ultrasonography provides information such as the size, location, and the presence of intrinsic septae in these cases. CT scan is done for better identification of the anatomy of the mass, and to determine its association with the surrounding organs.
Losanoff pathological classification is done for mesenteric cysts. It correlates pathological conditions with surgical options and strategies, apart from the nature of cysts. Accordingly, mesenteric cysts are divided into four groups: Type 1: pedicled cysts; type 2: Sessile that are limited to the mesentery and can be excised completely; type 3: Spread to the retroperitoneum, which is often inadequately resected, and type 4: Multicentre cysts requires complex surgery, sclerotherapy, or both. The standard treatment for mesenteric cysts is surgical resection.
There are very few cases reported of mesenteric cyst in pregnancy. Al-Mulhim AA reported a case of mesenteric cyst associated with a crossed ectopic kidney who underwent successful laparoscopic excision of the cyst in the second trimester of pregnancy [7].
Aliyu S et al reported a case of a giant mesenteric cyst measuring kg that coexisted with pregnancy [8]. The patient underwent spontaneous vaginal delivery followed by laparotomy at 6 weeks postpartum.
Manan Murlidhar Boob et al reported a case of 21 year old women who was provisionally diagnosed with a large mesenteric cyst in the antenatal period, however, on repeated imaging and exploration, it was found to be an adnexal mass with torsion [9].
Conclusion
Although mesenteric cysts are rare in adults, they should be considered in the differential diagnosis in cystic abdominal lumps. Once diagnosed they can be dealt with open as well as laparoscopic surgical excision safely.
References
-
Acharya K, Poudel D, Dahal S, Kuikel S, Adhikari A (2022) A case of huge ovarian cyst in second trimester: A rare case report. Annals of Medicine and Surgery 82: 104765.
-
Kurtz RJ, Heimann TM, Holt J, Beck AR (1986) Mesenteric and retroperitoneal cysts. Ann Surg 203(1): 109-112.
-
Hardin WJ, Hardy JD (1970) Mesenteric cysts. Am J Surg 119(6): 640- 645.
-
Mason JE, Soper NJ, Brunt LM (2001) Laparoscopic excision of mesenteric cysts: a report of two cases. Surg Laparosc Endosc Percutan Tech 11(6): 382- 384.
-
Mackenzie DJ, Shapiro SJ, Gordon LA, Ress R (1993) Laparoscopic excision of a mesenteric cyst J Laparoendosc Surg 3(3): 295-299.
-
Belhassen S, Meriem B, Rachida L, Nahla K, Saida H, et al. (2017) Mesenteric cyst in infancy: presentation and management. Pan Afr Med J 26: 191.
-
Al-Mulhim AA (2003) Laparoscopic excision of a mesenteric cyst during pregnancy. JSLS 7(1): 77-81.
-
Aliyu S, Buba AA, Ningi AB (2019) Giant Mesenteric Cyst Co-Existing with Pregnancy at Term. J Clin Trials 9(6): 390.
-
Boob MM, Chavan NN, Kapote D, Sakhalkar A, Kampoowale S, et al. (2023) An Interesting Case of an Adnexal Mass Mimicking a Mesenteric Cyst in Pregnancy. J South Asian Feder Obst Gynae 15(2): 248- 250.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review