Hook Wire Localization Failure of Peripheral Pulmonary Nodules during Perioperative Video-Assisted Thoracoscopic Surgery Period
Abstract Introduction: Computed tomography (CT) guided Hook wire localization is often used to identify peripheral small nodules prior to video-assisted thoracoscopic surgery (VATS). Pneumothorax, intrapulmonary hemorrhage, systemic air embolism, and wire dislodgement are well-known complications associated with the former procedure. Still, in this report, the situation of the Hook wire detached from the anchor point during perioperative operation is an infrequent and potentially fatal complication. We encountered four cases of Hook wire dislocation. The abnormal position needle of three cases was successfully removed during the operation, while the other one was successfully removed through reoperation, and all patients recovered smoothly after the operation and were discharged from the hospital.
Introduction
Common techniques for locating lung nodules include the following:Computed tomography (CT) guided percutaneous puncture assisted positioning technique including Percutaneous positioning by Hook wire and spring coil, Percutaneous liquid material injection positioning method, Electromagnetic-guided bronchoscopic puncture positioning technique, Virtual bronchoscope navigation and positioning technology, and CT virtual 3D assisted positioning technology. There are some advantages and disadvantages to the technique of preoperative auxiliary positioning in the lung node, and the surgeon should be able to use the right positioning technology and even the stereo anatomical location method and the hyper acoustic positioning of the technique are also very good [1]. In our hospital, Hook wire was also used to locate peripheral pulmonary nodules before thoracoscopic surgery. The introduction and usage of Hook wire are described in the literature [1].
Case 1 Presentation
A 58-year-old female was admitted to the hospital on February 22, 2022, due to “a small nodule was found in the upper lobe of the right lung “. After obtaining consent of the patient and his or her immediate family, CT-guided hook wire localization was conducted 1 hour prior to S2 segmentectomy under the video-assisted thoracoscopic surgery (VATS) on February 25, 2022. The entire Hook-wire positioning needle shrank into the chest wall muscle layer during the operation and was removed under X-ray fluoroscopy. Then, the operation was completed and the nodule was diagnosed as adenocarcinoma in situ. The operation took 155 minutes and Blood loss was 30 milliliters. The patient recovered successfully and was discharged from the hospital on March 4, 2022 (Figures 1).
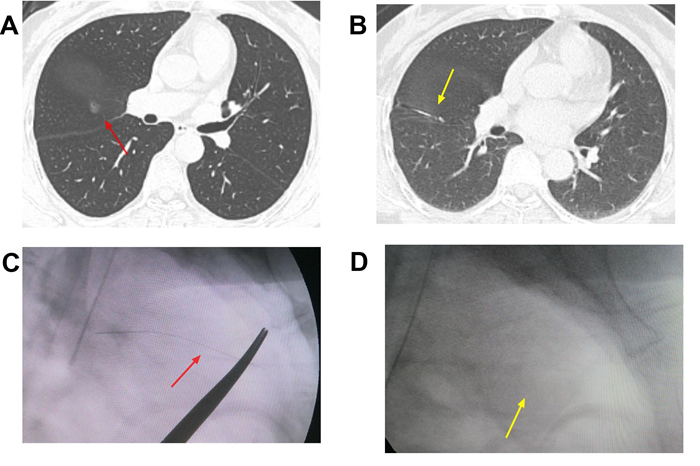
Figure 1: In case 1, A Red arrow points to a pulmonary nodule in the right upper lobe before surgery. B Yellow arrow points to a pulmonary nodule located by Hook wire before operation. C The red arrow points to the Intraoperative C-shaped X-ray localization of the Hook wire in the muscular layer of the chest wall. D The yellow arrow points to an X-ray picture of the right chest wall after removing the Hook wire.
Case 2 Presentation
A female, 58 years old, was admitted to our hospital due to a “The nodules of the right middle lobe were found about 2 years ago” on February 15, 2023. After obtaining consent of the patient and his or her immediate family, CT-guided hook wire localization was conducted 1 hour prior to wedge resection under the VATS on February 17, 2023. The hook wire was not found in the chest cavity during the operation. The positioning pin hole was slightly enlarged outside the chest wall and the positioning pin was removed in sequence. Then, wedge resection under the VATS was completed. Intraoperative rapid frozen section pathology revealed two lesions in the right middle lobe lung, one was adenocarcinoma in situ and the other was highly differentiated mucinous adenocarcinoma. Finally, the right middle lobe lung was removed and Groups 2, 4 and 7 lymph nodes were dissected intraoperatively. The operation took 275 minutes and Blood loss was 50 milliliters. The patient recovered successfully and was discharged from the hospital on February 26, 2023.
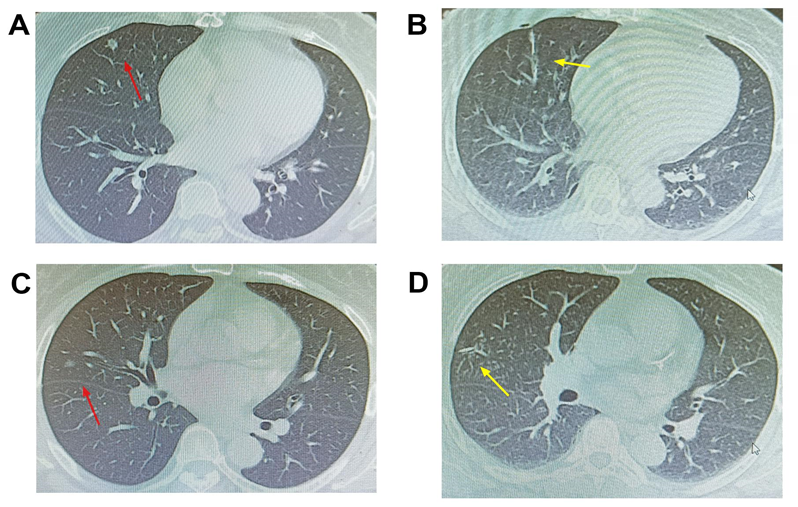
Figure 2: In case 2, A Red arrow points to a pulmonary nodule in the right middle lobe before surgery. B yellow arrow points to another pulmonary nodule in the right middle lobe before the operation. C The red arrow points to a pulmonary nodule located by Hook wire before operation. D The yellow arrow points to another pulmonary nodule located by the Hook wire before the operation, which fell out during the operation.
Case 3 Presentation
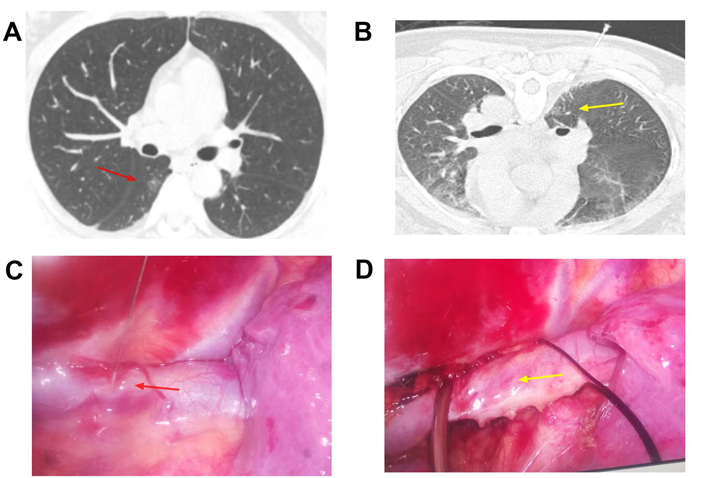
A female, 41 years old, was admitted to our hospital due to “Nodules of the right lower lung were found more than 1 year ago” on May 04, 2022. After obtaining consent of the patient and his or her immediate family, CT-guided hook wire localization was conducted 1 hour prior to wedge resection under the VATS on May 06, 2022. Hook wire was found to penetrate the Azygos vein arch during the operation and was removed under the thoracoscope. The method of dissociating the Azygos venous arch and wrapping the azygos vein on both sides of the puncture needle was adopted to prevent bleeding. The Hook wire was cut to remove the needle, and the azygos vein arch did not bleed. Then, wedge resection under the VATS was completed. The total operation time was 265 minutes. Intraoperative rapid frozen section pathology revealed invasive adenocarcinoma of the lower lobe of the right lung. Finally, the right lower lobe lung was removed and Groups 2, 4 and 7 lymph nodes were dissected intraoperatively. The operation took 265 minutes and Blood loss was 50 milliliters. The patient recovered successfully and was discharged from the hospital on May 16, 2022.
Case 4 Presentation
A female, 53 years old, was admitted to our hospital due to a “physical examination chest CT showed nodules in the right lower lung more than 4 months” on January 02, 2020. After obtaining consent of the patient and his or her immediate family, CT-guided hook wire localization was conducted prior to wedge resection under the VATS on January 05, 2020. The operation lasted 110 minutes. It was found that the Hook wire was not in the chest cavity during the operation, and the needle was forgotten and not removed during the operation. The nodule was diagnosed as adenocarcinoma in situ. After the examination of the chest X-ray postoperatively, it was found that there were needles in the chest wall. After fully communicating with the patient and his family, and obtaining their consent again, a reoperation was performed and the Hook wire was removed on January 12, 2020. Reoperation time is 10 minutes. The patient recovered successfully and was discharged from the hospital on January 15, 2020.
Discussion
CT guided Hook wire localization is often used to identify small nodules prior to video-assisted thoracoscopic surgery (VATS), and Professor Chen Haiquan’s team in the Affiliated Cancer Hospital of Fudan University in China developed this positioning technology earlier [2]. Hook wire localization has a high localization accuracy, short operation time, and few postoperative complications, and is therefore well suited to detect small pulmonary nodules in thoracic centers. However, it may also lead to complications or significant risks (e.g., pneumothorax, pulmonary hemorrhage, substantial pain, wire dislodgement, and systemic air embolism) [3, 4, 5].
In our four cases, the situations of the Hook wire detached from the anchor point during the perioperative period is an infrequent and potentially fatal complication.
Although there has been no unified standard for CT- guided Hook wire localization so far, some clinicians proposed the indications for using CT-guided Hook wire localization as described in the literature [6]. The focus of this report is that the situation of the failure of the positioning hook is relatively special. The reasons are as follows: If the pulmonary nodule is located in the outer third of the lung, especially near the subpleura, because of the insufficient depth or not entering the parenchyma vertically of the positioning needle, it will easily fall off, which is a technical problem. Such as the case of case 1, case 2, and case 4. The Hook wire needle was left in the chest wall due to carelessness and the lack of carefully check system enforcement at the end of the surgery, resulting in iatrogenic reoperation to remove the needle for case 4.
The complications above are related to the inexperience and maybe there’s a process where the surgeon has a learning curve [7]. In the early period of pulmonary nodule operation, the tail of the Hook wire is left outside the chest wall too little usually 1cm. When the Hook wire falls off from the lung, the needle is prone to be pulled back to the chest wall during the posture, such as in the case of case 1. Therefore, later, after positioning the patient, we firstly straightened the tail of the Hook wire outside the chest wall and left at least 3cm outside the chest wall to prevent the needle from sliding into the chest wall, so as not to find the hook wire inside and outside the chest wall during subsequent surgery. It is possible to mistakenly puncture the surrounding large blood vessels, which has the potential to cause major bleeding, such as case 3. After Hook-wire shedding, all lesions were successfully found and resected according to longitude and latitude positioning [8], and no lesions remained and the scope of lung surgery was unexpanded due to Hook-wire shedding.
Conclusion
Thoracoscopic pulmonary nodule surgery is a complicated process, and there is a learning curve in Hook wire positioning during perioperative video-assisted thoracoscopic surgery period in the early stage. Only by carefully designing the surgical plan and program before surgery, carefully following the surgical plan during surgery, in particular, check carefully at the end of the procedure to see if there are any unresolved details, and having foresight and countermeasures for possible risks during surgery can the operation be smooth and the patients be safe and satisfied.
Acknowledgments
Not applicable.
Authors’ Contributions
Shouqiang Yu collected the data of the patient, consulted literature, and wrote the manuscript; Yayun Sheng edited the manuscript and dealt with the Figures. Yonghui Quan also gave useful suggestions on writing and improved the manuscript. Zhiliang Zhou was the consultant in charge of the case, established the diagnosis, and approved the submitted version. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Institutional Review Board Statement
Because it is a retrospective study, the publication of this article exempted patients from signing a written informed consent.
Funding
None. The author(s) received no financial support for the research, authorship, and/or publication of this article
Data Availability Statement
The datasets used and analysed in the current study are available from the corresponding author on demand.
References
-
Liu B, Gu C (2019) Expert Consensus on Preoperative Assisted Positioning of Pulmonary Nodules. Chinese Clinical Journal of Thoracic and Cardiovascular Surgery 26(02): 109-113.
-
Chen S, Zhou J, Zhang J, Hu H, Luo X, et al. (2011) Video- assisted thoracoscopic solitary pulmonary nodule resection after CT-guided hook wire localization: 43 cases report and literature review. Surg Endosc 25(6): 1723-1729.
-
Qin W, Ge J, Gong Z, Zhang Y, DiBardino DM, et al. (2022) The incidence and risk factors of acute pain after preoperative needle localization of pulmonary nodules: a cross-sectional study. Translational lung cancer research 11(8): 1667-1677.
-
Yi JH, Choi PJ, Bang JH, Jeong SS, Cho JH (2018) Systemic air embolism after computed tomography-guided hook wire localization: two case reports and literature review. J Thorac Dis 10(1): E59-E64.
-
Yu A, Jiao Z, Wang T (2021) Air embolism after CT-guided localization of pulmonary nodule: one case report]. Chinese Journal of Thoracic and Cardiovascular Surgery 37(11): 686-687.
-
Chen D, Dai C, Kadeer X, Mao R, Chen Y, et al. (2018) New horizons in surgical treatment of ground-glass nodules of the lung: experience and controversies. Therapeutics and clinical risk management. 31(14): 203-211.
-
Ma S, Yan T, Liu D, Wang K, Wang J, et al. (2018) Minimally invasive esophagectomy in the lateral-prone position: Experience of 124 cases in a single center. Thorac Cancer 9(1): 37-43.
-
Zhou N, Shan H, Zhang A (2020) Cross-sectional CT guidance for positioning small pulmonary nodules under direct vision: oblique line-dial positioning. Journal of Clinical Pulmonary Medicine 25(09): 1301-1320.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review