A Case Report of the Warshaw Procedure Used In Blunt Pancreatic Trauma
Spleen preserving surgery in not commonplace in acute trauma due to haemodynamic instability. In the case below we describe a delayed presentation (3 days) of blunt pancreatic injury in which we were able to successfully perform a spleen persevering distal pancreatectomy. Thereby negating the post splenectomy side effects in this young patient. The Warshaw procedure was used due to her haemodynamic stability on presentation. Thus, given certain patient circumstances (haemodynamic stability), spleen preserving surgery can be successfully performed for traumatic injury
Introduction
Spleen preserving distal pancreatectomies is not a common procedure in traumatic injury mainly due to patients’ haemodynamic instability. The procedure is commonly described for benign and malignant disease of the distal pancreas [1]. This shift toward splenic preservation surgery in non-traumatic patients, negates the risks associated with splenectomies. Namely overwhelming post- splenectomy infections (OPSI), the need for vaccinations, hypercoagulability and haematological malignancies [1].
Splenic preservation can be achieved by either ligation or preservation of the splenic vessels. The first described spleen preserving distal pancreatectomy was by Mallet- Guy and Vachon in 1943, in which the splenic vessels were preserved [1].
The Warshaw procedure relies on ligation of the splenic vessels and maintenance of the blood flow to the spleen via the short gastric arteries. This procedure was initially described by Warshaw AL [2], it was successfully completed in 22 of 25 patients, of which their pathologies included acute and chronic pancreatitis, pancreatic necrosis, cystic neoplasms and ductal adenocarcinoma, but no trauma cases [2]. From the above description of the two types of splenic preservation surgery, once can postulate that the dissection would be time consuming, and in trauma, time is not always an option and thus the paucity of literature in trauma cases.
Below we will describe a case of blunt pancreatic trauma in which the Warshaw technique was successfully used at a level 1 Trauma centre as well as review the pertinent trauma studies. The report is according to the SCARE checklist [3]. Written consent from the patient for photographs and the case report as well as ethics approval by the University of the Witwatersrand Human Research Ethics Committee (Medical) No: M 220795 was issued.
Case Summary
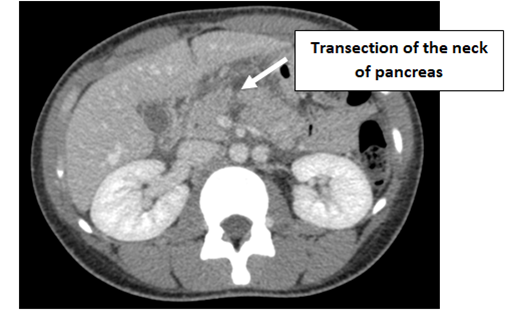
A 22-year female was transferred via ambulance from a peripheral hospital to Chris Hani Baragwanath Academic Hospital Level 1 Trauma Unit. She sustained blunt abdominal trauma by falling onto a crowbar 3 days prior. She had progressive worsening of abdominal pain and emesis, a CT abdomen at the referral hospital was done, which showed complete transection of the neck of the pancreas (Figure 1). Serum amylase was 355 U/L at the time of presentation at the referral hospital (3 days post injury). She was haemodynamically stable with a tender but not peritonitic abdomen. She had no significant past medical, surgical, family or drug history.
At laparotomy, a 75% transection of the neck was found at the level of the superior mesenteric vein. The Warshaw procedure was done which resulted in minimal blood loss with an operative time of about 1.5 hours, the splenic vessels were ligated, and the short gastric arteries preserved.
The pancreas was transected sharply and sutured with pencil drains placed (Figure 2). Post operatively she was transferred to ICU for one day and initiated on nasojejunal feeds. On day 3 her drain fluid amylase was 221 U/L and therefore a concern for a pancreatic fistula, however the right pencil drain stopped draining on day 5 and was removed, the left pencil drain was removed on day 10, and she was started on oral diet on day 3.
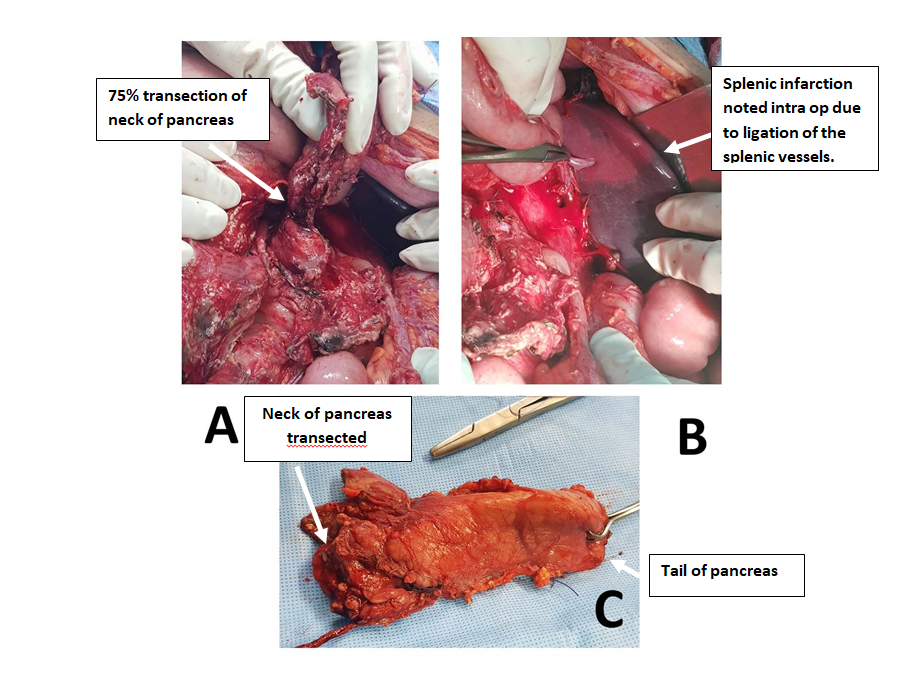
A: pancreatic transection (white arrow) B: macroscopic view of splenic infarction post splenic vein and artery ligation (white arrow) C: resected specimen – distal pancreas Figure 2: intra-operative findings.
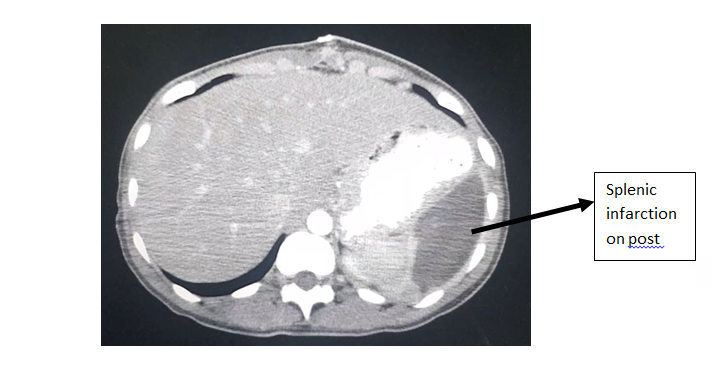
On day 10 she had a follow up CT abdomen which showed the splenic infarction involving two-thirds of the spleen as expected and no pancreatic collections seen see Figure 3.
The patient’s hospital stay was uneventful, and she was discharged home. At her follow up visit a month later the patient was well. Subsequent telephonic follow up at 4 years revealed no complications.
Discussion
In our young patient we successfully managed to preserve her spleen thereby negating the post splenectomy complications, such as overwhelming post-splenectomy infections (OPSI) which has a mortality rate of 50%, hypercoagulability and haematological malignancies [1, 4]. Long term risks associated with the Warshaw procedure is local portal hypertension, gastric fundus varicose veins, variceal bleeding, and splenic infarction [4]. Splenic infarction is relatively common 23% as is the case in our patient, however only 1.9% require re operation for abscess formation. The splenic blood supply from the short gastric arteries post a Warshaw procedure quickly develop collaterals and even a 20% infarcted spleen is still functional [5]. Generally, this complication is noted on post-operative imaging on patients symptomatic for left upper quadrant pain, however we noticed it intra operatively and thus far our patient is asymptomatic [5].
A meta- analysis comparing spleen preserving distal pancreatectomy and distal pancreatectomy with splenectomy, showed a shorter hospital stay and lower incidence of intra- abdominal abscesses in the spleen preserving cases. No statistical significant differences were seen in operative times, blood loss and pancreatic fistula rates [1]. Again, all studies were done on benign disease of the pancreas. The Warshaw procedure had a higher incidence of splenic infarcts. The above literature is on non- traumatic pancreatic pathology, however these non-statistically significant complications has been the argument for not using splenic preserving surgery in trauma [1].
Although multiple successful case reports of spleen preserving distal pancreatectomies with or without splenic vessel ligation in a trauma setting have been reported. The most recent case report was described in 2021, where the authors experienced significant technical challenges during surgery due to the concomitant pancreatitis obscuring the planes between the pancreas, splenic vessels (which were preserved) and the post wall of the stomach [5]. Lin et al reviewed a 25- year period, which included 51 trauma patients. They found that a distal pancreatectomy with splenectomy has a greater mortality rate, abdominal morbidity and their associated pancreatic fistula rate required more interventions [6].
The largest review to date includes 834 trauma patients over an 8-year period. Patients sustained penetrating and blunt abdominal trauma. Patients that had splenic preserving surgery had a shorter hospital stay, but no statistically significant differences were found in complication rate, mortality rate and ICU length of stay [7]. Essentially spleen preserving surgery is associated with less morbidity and is safe in the haemodynamic ally stable patient, regardless of splenic vessel preservation.
In conclusion, the Warshaw procedure is a safe and effective method for splenic preservation in the trauma setting on a stable patient.
References
-
He Z, Qian D, Hua J, Gong J, Lin S, et al. (2014) Clinical comparison of distal pancreatectomy with or without splenectomy: a meta-analysis. PLoS One 9(3): e91593-e91593.
-
Warshaw AL (1988) Conservation of the spleen with distal pancreatectomy. Arch Surg 123(5): 550–553.
-
Agha RA, Franchi T, Sohrabi C, Mathew G, Kerwan A, et al. (2020) The SCARE 2020 Guideline: Updating Consensus Surgical Case Report (SCARE) Guidelines. Int J Surg 84: 226-230.
-
Ferrone CR, Konstantinidis IT, Sahani DV, Wargo JA, Warshaw AL, et al. (2011) Twenty-three years of the warshaw operation for distal pancreatectomy with preservation of the spleen. Ann Surg 253(6): 1136-1139.
-
Mulpuri VB, Bhuria DK, Rana S, Gupta R (2021) Spleen- preserving distal pancreatectomy following grade III pancreatic injury in a delayed presentation: A technical challenge. BMJ Case Rep 14(6): e242721.
-
Lin BC, Chen RJ, Hwang TL (2018) Spleen-preserving versus spleen-sacrificing distal pancreatectomy in adults with blunt major pancreatic injury. BJS Open 2(6): 426-432.
-
Schellenberg M, Inaba K, Cheng V, Bardes JM, Lam L, et al. (2018) Spleen-preserving distal pancreatectomy in trauma. J Trauma Acute Care Surg 84(1): 118-22.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review