Thyroglossal Cyst in Adolescent: Managed with Modified Sistrunk Operation
One kind of congenital entity that results from inadequate closure of the thyroglossal duct is the thyroglossal duct cyst (TDC). It has clinical symptoms at any age and frequently needs to be surgically removed in addition to being a dormant embryological remnant. The infrahyoid area is home to the majority of them. Adult thyroglossal duct cysts (TDCs) are an uncommon disorder. In this case, we were reporting on a thirty-two-year-old female patient who had a thyroglossal cyst that was surgically excised using a modified version of the Sistrunk technique. Fifteen months was the median follow-up period, with no problems. Adult patients with this clinical condition require a high degree of skepticism from surgeons.
Introduction
The most prevalent congenital neck mass, a thyroglossal duct cyst (TDC), often manifests in the first ten years of life [1, 2, 3]. A neck swelling that is painless, cystic, mobile, fluctuant, and midline in nature that does not cause any symptoms unless it is infected is the traditional presentation. Comprehending the embryological source of TDC is essential to its effective management. As the thyroid primordium descends from the root of the tongue down the midline to a final position in the anterior area of the neck, it passes anterior, posterior, and through the hyoid bone. The thyroglossal duct usually closes completely, but if remains persist, cysts or fistulas can develop [4]. The literature analysis indicates that around 7% of the population experiences this developmental defect [5].
A correlation between malignancy and TDC is observed in around 1% of individuals [5, 6].Due to its congenital nature, adults seldom have occurrences of this condition; children are the ones who experience it most frequently. For this reason, the majority of the data on the topic concentrate on treating the illness in kids [7, 8].
Around the world, the standard procedure for managing TDC is acknowledged as being the Sistrunk operation [4]. The cyst, the middle section of the hyoid bone (the body), and the tract up to the foramen cecum are excised during the surgery. The majority of current case studies regarding the treatment of thyroglossal cysts in children demonstrate excellent results after the Sistrunk surgery. There aren’t many studies on the treatment of TDC in adults as this ailment is uncommon in this age group. TDC is confirmed by use of modern imaging modalities including computerized tomography (CT) of the neck and ultrasonography (USG).
Surgery has been around for a while; Sistrunk originally described it . It is used to treat cysts that cause problems, such as recurring infection or irritation [9]. As is typical nowadays, he described removing the cyst together with the middle section of the hyoid bone. But he also talked about how crucial it is to remove the whole duct tissue that connects the hyoid to the foramen caecum. According to him, “better results are obtained when the duct above the hyoid bone is not isolated [9].”This is accomplished by “coring out, in a sense, the tissues between the foramen caecum and the hyoid bone”[9]. Marshall and Becker used this method to report a recurrence rate of just 1.3% in their 310-case series [10].
However, the most recent evidence available indicates a return rate above 4% [11]. This, in our opinion, is an example of how the Sistrunk process has been modified and is being used. This entails the conventional excision of the core hyoid bone, as opposed to Sistrunk’s description of the coring out of the suprahyoid tissues [9].
Case report
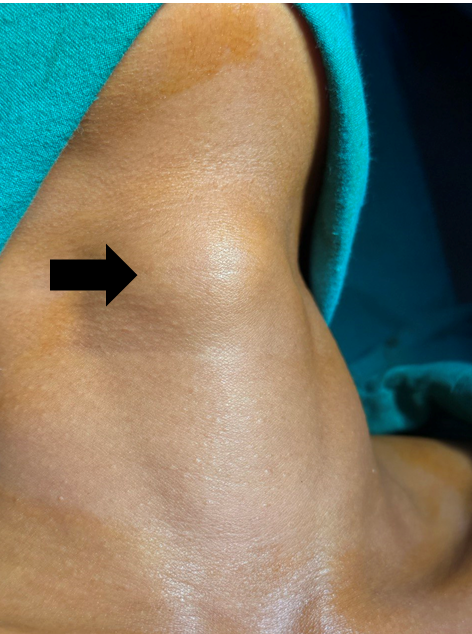
A 32-year-old female patient arrived to our hospital complaining of midline neck swelling that had been bothering her for four to five years (Figure 1). It was progressively growing in size. There was no history of trauma or a significant rise in swelling size. There was no evidence of upper respiratory tract infection or dysphagia. There was no evidence of either hyperthyroidism or hypothyroidism. On inspection, there was a 2x2 cm swelling at the infrahyoid area. It moved in response to deglutition and tongue protrusion. There were no sinuses or dilated veins around the swelling, and there were no symptoms of inflammation (Figure 2). Palpation revealed a 2x2cm swelling in the infrahyoid area and slightly above the thyroid notch. It was soft, cystic, non-tender, and non- fluctuant. The swelling of the skin was normal. The patient was recommended to undergo ultrasonography to determine the size of the lesion and its relationship to the normal thyroid gland.

Figure1: Clinical picture of midline neck swelling which moves with protrusion of tongue.
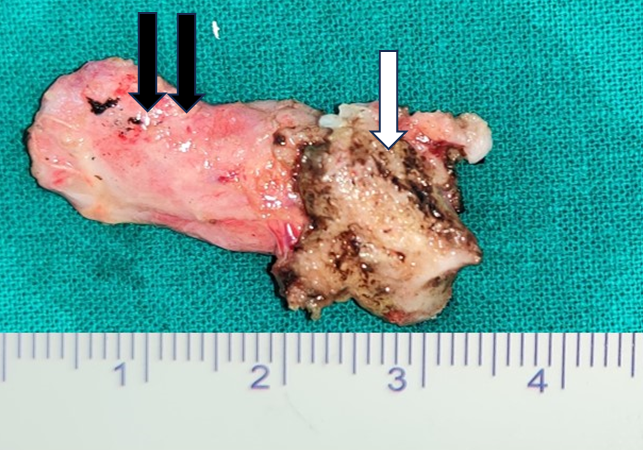
Her thyroid profile test and full blood counts were also normal. Fine needle aspiration cytology (FNAC) revealed a benign cystic lesion. The patient had been advised to have surgical intervention for management purposes. After obtaining adequate permission, the patient was admitted for surgical removal of a thyroglossal duct cyst under general anaesthesia. A midline neck crease incision was made, and a subplatysmal flap was raised. The cyst was discovered immediately above the thyroid notch (Figure 3). The dissection was carried out throughout the thyroglossal tract until the hyoid bone was discovered (Figure 4). The hyoid’s body was skeletonized and divided. The hypoglossal nerve was not damaged. The tract was completed at the hyoid body. To avoid recurrence, Sistrunk’s technique was modified and the surrounding tissue at the base of the tongue was removed. The surgical specimen was sent to histology for examination.


Figure 5 Haemostasis was established, and the surgical incision was closed in layers. The patient had been transferred to the recovery area after successful extubation. Patient was discharged after two days of intravenous antibiotics. The biopsy is based on her histology result, which indicates a cyst surrounded by columnar epithelium. Inflammatory cells and dilated arteries are abundantly invading the underlying fibro collagenous wall. There was no thyroid tissue to be discovered. Overall histomorphology implies a benign cyst (Figure 6). There was no evidence of granuloma or malignancy. In her frequent check-ups till fifteen months, the patient was doing well, with no recurrences.
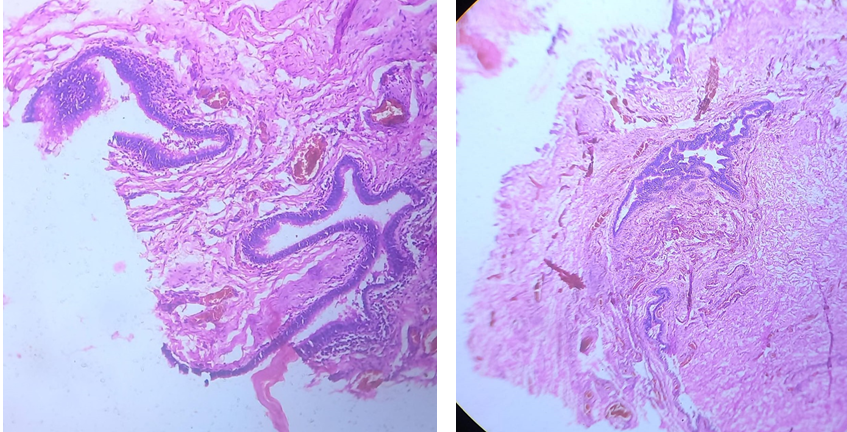
A B Figure 6: (A and B) Histopathological slides.
Discussion
The development of TDC is the result of the non- obliteration of the thyroglossal duct. It becomes the thyroid’s pyramidal lobe if just the lowest portion of the duct survives. Located in the middle of the tongue, halfway between the anterior two thirds and the posterior one third, is the foramen cecum, a little blind hole that represents the ductal aperture.
Although the likelihood of this ductal cyst developing in the hyoid bone, tongue, or floor of the mouth is remote, it can develop anywhere along the thyroglossal duct’s route.
According to Ghaneim A, et al. [12], while TDC is found between the hyoid bone and the thyroid cartilage in around 60% of individuals, it is also present suprahyoid, suprasternal, and intralingual in approximately 24%, 13%, and 2% of patients, respectively.
However, reports of exceedingly unusual locales have also been made. For example, Tas et al. described an intrahyoid TDC site [13], while Soon et al. reported a case of TDC that sank into the mediastinum [14]. Though they can sometimes manifest later in adulthood, thyroglossal duct cysts (TDCs) are most commonly detected in paediatric patients, with at least half of them being discovered in the second decade of life [15]. While 1% of cases may be cancerous, the majority are benign [16]. Data on the issue are few in the adult population since TDCs are uncommon in adults. The TDC that breaks down spontaneously presents as a discharging sinus, sometimes incorrectly referred to as a thyroglossal fistula.
Nonetheless, reports in research continue to differ, with some claiming an equal distribution [4, 17, 18] and others suggesting a plurality of either men or women [15, 19, 20, 21]. Due to its connection to the foramen cecum and hyoid bone, the cyst usually travels cranially during tongue protrusion and swallowing. In adult patients, the most common manifestation of TDC is a painless anterior neck lump.
Complications like abscess development are frequently indicated by the presence of additional symptoms including pain, odynophagia, dysphagia, and dyspnoea [4, 15, 18, 19, 21].
The USG neck, which displays a cystic lesion, is one investigation used to find TDC [21]. A benign TGD cyst on a CT scan presents as a midline, smooth-walled, fluid- attenuated mass close to the hyoid bone level [21, 22]. Differential diagnosis includes dermoid cyst, branchial cyst, haemangioma, and lymph node enlargement. According to Sistrunk’s description, thyroglossal cyst excision should always involve removal of the suprahyoid thyroglossal duct to avoid recurrence [9].
This operation has changed over the years, and many surgeons no longer carry out the surgery exactly as Sistrunk initially described. The tissue above the hyoid is usually not excised completely, even if the cyst and a part of the hyoid bone are typically removed together [23]. It is customary to just keep following the tract above the hyoid until it breaks off or vanishes. This is completely at odds with the process that Sistrunk outlined, claiming that this was the precise cause of the prior high recurrence rates [9]. Thyroglossal duct cysts have a variety of epithelial lining types. The cysts may be lined by pseudostratified ciliated epithelium or squamous epithelium. On rare occasions, the cysts may lose their epithelium [24].
The use of robot assistance in endoscopic procedures via transoral and retro auricular channels in adults is one of the more recent methods [25]. Beyond cosmesis, there is disagreement over the benefits of these techniques over the conventional Sistrunk surgery. Recurrence in as much as 3–5% of cases after a typical Sistrunk procedure is the most commonly reported complication [17, 18, 26, 27].
The hypoglossal nerve may sustain harm as a result of its immediate relationship to the hyoid bone, among other infrequent consequences.
With cautious dissection and preservation of the hyoid bone’s superior horn, the nerve is spared [26, 27]. After lingual thyroid, TDCs are the second most frequent location for ectopic thyroid tissue [28]. The majority of ectopic thyroid tissue found in TDCs manifests in combination with a thyroid gland that is normally positioned and develops [29]. About one-third of individuals may be hypothyroid upon presentation, although the bulks are frequently euthyroid [30]. This supports the need for regular thyroid function testing and ultrasonography as part of the assessment procedure.
Research suggests that the following variables may increase the chance of recurrence of TDC: age at surgery, preoperative infection, abscess with or without drainage, and multi-cystic histology [31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41]. A number of studies have assessed the risk variables for recurrence following TDC resection. Perkins et al. reported a 23-year recurrence rate of 15% overall in 231 patients, and discovered that 20% of recurrences happened when the foramen cecum was left unresected [42].
Other groups have reported that failure to perform hyoidectomy and pre-operative infections are the most prevalent risk factors for recurrence. While Marianowski R, et al. [35], discovered greater recurrence rates following two or more infections, Ducic et al. and Flagoele et al. observed considerably higher recurrence rates following a single pre- operative infection [23, 33, 35]. In contrast, Burgues et al. did not identify any influence of pre-operative infection on recurrence [43]. No recurrence was discovered throughout the median follow-up period of 15 months for our patients.
Conclusion
Adult patients with this medical condition require a high degree of skepticism from surgeons. Immediately referring a patient to a specialist is essential for conventional procedure instead of incision and drainage, which has a high incidence of recurrence. The Sistrunk procedure has had positive results. in addition to highlighting the infrequency of TDC in adults, this research offers information on the condition's pattern of occurrence and treatment. Thyroglossal duct cysts are quite frequent, although they should be considered a differential diagnosis in older individuals if they develop in an age range other than normal. This might create a diagnostic issue. It is mentioned that in order to stop TDC from recurring, understanding embryology is crucial, as is careful dissection along anatomical planes and excision of the hyoid bone's core.
Compliance with Ethical Standards
The procedure performed in this case report was in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.”
Funding
This study is not funded by any resources.
Conflict of Interest
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this paper.
Ethical Approval
The study was published with written consent of the patient.
References
-
Plante JKL, Pierson NS, Hedlund GL (2015) Common pediatric head, and neck congenital/developmental anomalies. Radiol Clin North Am 53(1): 181-196.
-
Torsiglieri AJ Jr, Tom LW, Ross AJ, Wetmore RF3rd, Handler SD, et al. (1988) Pediatric neck masses: guidelines for evaluation. Int J Pediatr Otorhinolaryngol 16(3): 199-210.
-
Goins MR, Beasley MS (2012) Pediatric neck masses. Oral Maxillofac Surg Clin North Am 24(3): 457-468.
-
Allard RH (1982) The thyroglossal cyst. Head Neck Surg 5(2): 134-146.
-
Hassan Ne, See Gb, Dayang, Aziz Da (2014) Thyroglossal duct cysts – a ten years retrospective review. East J Med 19(2): 112-118.
-
Dedivitis RA, Guimarães AV (2000) Papillary thyroid carcinoma in thyroglossal duct cyst. Int Surg 85(3): 198- 201.
-
Al‑Thani H, El‑Menyar A, Sulaiti MA, El-Mabrok J, Hajaji K, et al. (2016) Presentation, management, and outcome of thyroglossal duct cysts in adult and pediatric populations: A 14‑year single center experience. Oman Med J 31(4): 276-283.
-
Dedivitis RA, Camargo DL, Peixoto GL, Weissman L, Guimarães AV (2002) Thyroglossal duct: A review of 55 cases. J AmColl Surg 194(3): 274-277.
-
Sistrunk WE. (1920) The surgical treatment of cysts of the thyroglossal tract. Ann Surg 71(2): 121-122.
-
Marshall SF, Becker WF (1949) Thyroglossal cysts and sinuses. Ann Surg 129(5): 642-651.
-
Kim MK, Pawel BR, Isaacson G (1999) Central neck dissection for the treatment ofrecurrent thyroglossal duct cysts in childhood. Otolaryngol Head Neck Surg 121(5): 543-547.
-
Ghaneim A, Atkins P (1997) The management of thyroglossal duct cysts. Int J Clin Pract 51(8): 512-513.
-
Tas A, Karasalihoglu AR, Yagiz R, Doğanay L, Guven S (2003) Thyroglossal duct cyst in hyoid bone: unusual location. J Laryngol Otol 117(8): 656-657.
-
Chon SH, Shinn SH, Lee CB, Tae K, Lee YS, et al. (2007) Thyroglossal duct cyst within themediastinum: an extremely unusual location. J Thorac Cardiovasc Surg 133(6): 1671-1672.
-
Turkyilmaz Z, Sonmez K, Karabulut R, Demirgoullari B Sezer C, et al. (2004) Management of thyroglossal ductcysts in children. Pediatr Int 46(1): 77-80.
-
Miccoli P, Minuto MN, Galleri D, Berti P, Puccini M (2004) Extend of surgery in TGDC carcinoma reflections on a series of 18 cases. Thyroid 14(2): 121-123.
-
Lin ST, Tseng FY, Hsu CJ, Yeh TH, Chen YS (2008) Thyroglossal duct cyst: A comparison between children and adults. Am J Otolaryngol 29(2): 83-87.
-
Brousseau VJ, Solares CA, Xu M, Krakovitz P, Koltai PJ (2003) Thyroglossal duct cysts: Presentation and management in children versus adults. Int J Pediatr Otorhinolaryngol 67(12): 1285-1290.
-
Hsieh YY, Hsueh S, Hsueh C, Lin JN, Luo CC, et al. (2003) Pathological analysis of congenital cervical cysts in children: 20 years of experience at Chang Gung Memorial Hospital. Chang Gung Med J 26(2): 107-113.
-
Zaman SU, Ikram M, Awan MS, Hassan NH (2017) A decade of experience of management of thyroglossal duct cyst in a tertiary care hospital: Differentiation between children and adults. Indian J Otolaryngol Head Neck Surg 69(1): 97-101.
-
Ahuja AT, Wong KT, King AD, Yuen EHY (2005) Imaging for thyroglossal duct cyst: the bare essentials. Clin Radiol 60(2): 141-148.
-
Beede DL, Bergeron RT, Som PM (1985) CT of thyroglossal duct cysts. Radiology 157(1): 121-125.
-
Howard DJ, Lund VJ (1986) Thyroglossal ducts, cysts and sinuses: a recurrent problem. Ann R Coll Surg Engl 68(3): 137-138.
-
Gregory M, Organ CH (2000) Thyroid gland and surgery of the thyroglossal duct: exercise in applied embryology. World J Surg 24(8): 886-890.
-
Kim CH, Byeon HK, Shin YS, Koh YW, Choi EC (2014) Robot-assisted Sistrunk operation via a retro auricular approach for thyroglossal duct cyst. Head Neck 36(3): 456-458.
-
Ogunkeyede SA, Ogundoyin OO (2019) Management outcome of thyroglossal cyst in a tertiary health center in Southwest Nigeria. Pan Afr Med J 34: 154.
-
Ndegbu CU, Olasehinde O, Adeyemo A, Alatise OI, Amusa YB (2021) Management of thyroglossal cyst in adults: a single-institution experience. Niger J Surg 27(1): 38-41.
-
Lilley JS, Lomenick JP (2013) Delayed diagnosis of hypothyroidism following excision of a thyroglossal duct cyst. J Pediatr 162(2): 427-428.
-
Massine RE, Durning SJ, Koroscil TM (2001) Lingual thyroid carcinoma: A case report and review of the literature. Thyroid 11(12): 1191-1196.
-
Radkowski D, Arnold J, Healy GB, McGill T, Treves ST, et al. (1991) Thyroglossal duct remnants. Preoperativeevaluation and management. Arch Otolaryngol Head Neck Surg 117(12):1378-1381.
-
Mickel RA, Calcaterra TC (1983) Management of recurrent thyroglossal duct cysts. Arch Otolaryngol 109(1): 34-36.
-
Ein SH, Shandling B, Stephens CA, Mancer K (1984) The problem of recurrent thyroglossal duct remnants. J Pediatr Surg 19(4): 437-439.
-
Ducic Y, Chou S, Drkulec J, Ouellette H, Lamothe A (1998) Recurrent thyroglossal duct cysts: a clinical and pathologic analysis. Int J Pediatr Otorhinolaryngol 44(1): 47-50.
-
Shah R, Gow K, Sobol SE (2007) Outcome of thyroglossal duct cyst excision is independent of presenting age or symptomatology. Int J Pediatr Otorhinolaryngol 71(11): 1731-1735.
-
Marianowski R, Ait Amer JL, Morisseau Durand MP, Rassi S, Manach Y (2003) Risk factors for thyroglossal duct remnants after Sistrunk procedure in a pedi- atric population. Int J Pediatr Otorhinolaryngol 67(1): 19-23.
-
Ostlie DJ, Burjonrappa SC, Snyder CL, Murphy JP, Watts J, et al. (2004) Thyroglossal duct infections and surgical outcomes. J Pediatr Surg 39(3): 396-399.
-
Hirshoren N, Neuman T, Udassin R, Elidan J, Weinberger JM (2009) The imperative of the Sistrunk operation: review of 160 thyroglossal tract remnant operations. Otolaryngol Head Neck Surg 140(3): 338-342.
-
Bennett KG, Organ CH Jr, Williams GR (1986) Is the treatment for thyroglossal duct cysts too extensive? Am J Surg 152(6): 602-605.
-
Athow AC, Fagg NL, Drake DP (1989) Management of thyroglossal cysts in children. Br J Surg 76(8): 811-814.
-
Hoffman MA, Schuster SR (1988) Thyroglossal duct remnants in infants and children: reevaluation of histopathology and methods for resection. Ann Otol Rhinol Laryngol 97 (5Pt1): 483-486.
-
Pelausa ME, Forte V (1989) Sistrunk revisited: a 10- year review of revision thy- roglossal duct surgery at Toronto’s hospital for sick children. J Otolaryngol 18(7): 325-333.
-
Ryu YJ, Kim DW, Jeon HW, Chang H, Sung MW, et al. (2015) Modified Sistrunk op- eration: new concept for management of thyroglossal duct cyst. Int J Pediatr Otorhinolaryngol 79(6): 812-816.
-
Flageole H, Laberge JM, Nguyen LT, Adolph VR, Guttman FM (1995) Reoperation for cysts of thyroglossal duct. Can J Surg 38(3): 255-259.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review