A Prospective Study of Total Extra Peritoneal Inguinal Hernia Repair Fixation versus no Fixation of Mesh
Background: The necessity of mesh fixation in laparoscopic totally extra peritoneal (TEP) inguinal hernia repair remains controversial. We performed a single-center prospective study to compare the effectiveness of mesh fixation versus nonfixation in laparoscopic TEP repair. Materials and Methods: This study was conducted in the Department of Surgery, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, India, from August 2021 to July 2023. All patients admitted to the General surgical unit with uncomplicated inguinal hernias were included. A total of 96 patients were included in the study, of which 44 patients underwent TEP repair with fixation of mesh using tacks (GROUP A) and the remaining 52 patients whose mesh was not fixed (GROUP B). Results: Ninety-six patients were randomized to fixation or non-fixation group in TEP. The pain scores at 24 hours, 72 hours, 7 days, 1 month, and 3 months were comparable, but not statistically significant (Day 1 Fixation, 2.7 ± 0.79; Non-fixation 2.48 ± 0.78, P = 0.104, 1 week (Fixation, 0.02 ± 0.15; Non-fixation, 0.08 ± 0.27, P = 0.236). The length of hospital stay (Fixation, 2.07 ± 0.59 days; Non-fixation, 2.1 ± 0.41 days, P = 0.785) and days taken to resume normal activities (Fixation, 3.7 ± 1.02 days; Non-fixation, 3.54 ± 0.94 days, P = 0.41) were also similar for both groups. There was no recurrence in either group at a minimum follow-up of 12 months. The cost of surgery was significantly different between the fixation group and the nonfixation group with a p-value <0.0001. Conclusion: There was no statistical significance between the fixation and non-fixation groups in terms of postoperative pain, requirement and dosage of analgesics, duration of in-hospital stay, time to return to normal activity, complications, recurrence of hernia, except the cost of surgery which was higher in the fixation group.
Abbreviations
TAPP: Trans Abdominal Preperitoneal; TEP: Total Extra Peritoneal.
Introduction
Inguinal hernia repair is a common surgery, performed annually by over 20 million patients worldwide. The treatment of choice is surgical repair with mesh using an open or laparoscopic approach [1].
Laparoscopic repair techniques are associated with significantly less postoperative pain and an earlier return to work compared to open surgery [2]. One advantage of laparoscopic inguinal repair is the inspection of the contralateral side for hernia presence, which is found in 8-51% of patients with unilateral inguinal hernias [3]. Laparoscopic
techniques include Trans abdominal preperitoneal (TAPP), Total extraperitoneal (TEP), and Extended view TEP (e-TEP). The extraperitoneal laparoscopic repair, although initially technically demanding with a long learning curve has evolved into the most popular technique. The peritoneal space is not violated, thus avoiding complications. Laparoscopic total extraperitoneal repair relies on placing a prosthetic mesh in the preperitoneal plane to strengthen the posterior wall of the inguinal canal and prevent recurrence. However, the use of staples or tacks can cause postoperative pain and nerve injury, occurring in 2%-4% of laparoscopic inguinal hernioplasties [4]. Unstapled laparoscopic hernia repair has emerged as a preferable alternative, avoiding complications associated with stapling and offering attractive economic logistics.
Aims and Objectives
The current study aimed to analyse the outcome in laparoscopic Total Extraperitoneal repair (TEP) of fixation vs. non-fixation of mesh in inguinal hernia patients for post- operative pain, time of the surgical procedure, intra and postoperative complications, dosage of analgesics consumed, days of hospital stay after surgery, cost-effectiveness, and the recurrence.
Material and Methods
This study was conducted as a randomized, prospective study following approval by the Institutional Review Board and with the written informed consent of all participants. All patients admitted in the General surgical unit of Jawaharlal Nehru Medical College and Hospital, Aligarh Muslim University, India. Study Population All patients presenting with uncomplicated inguinal hernias above 18 years were included. Those patients were excluded who did not meet the criteria for general anesthesia, had a history of previous lower abdominal surgery, or patients with obstructed and strangulated inguinal hernias. Ninety-six patients were enrolled in the study between August 2021 and July 2023. 44 patients underwent TEP repair with fixation of the mesh (Group A) and the remaining 52 without mesh fixation (Group B) (Figures 1 & 2).
Procedure
The procedure involved a skin incision at the umbilicus, opening the anterior rectus sheath, and retracting the muscle laterally followed by a blunt dissection to create an extra peritoneal tunnel. Two 5 mm trocars were inserted through the midline to prevent damage to the bladder, peritoneum, or bowels.
The dissection began along the midline, below the rectus muscle, and towards the pubic arch. Cooper’s ligament was identified, and the fatty tissue in the preperitoneal region was kept in contact with the inguinal floor. The lateral dissection was made in a surgical plane below the inferior epigastric vessels and above the peritoneum. All hernia defects were identified and repaired, with the final stage involving a macropore synthetic prosthesis covering the myopectineal orifice.
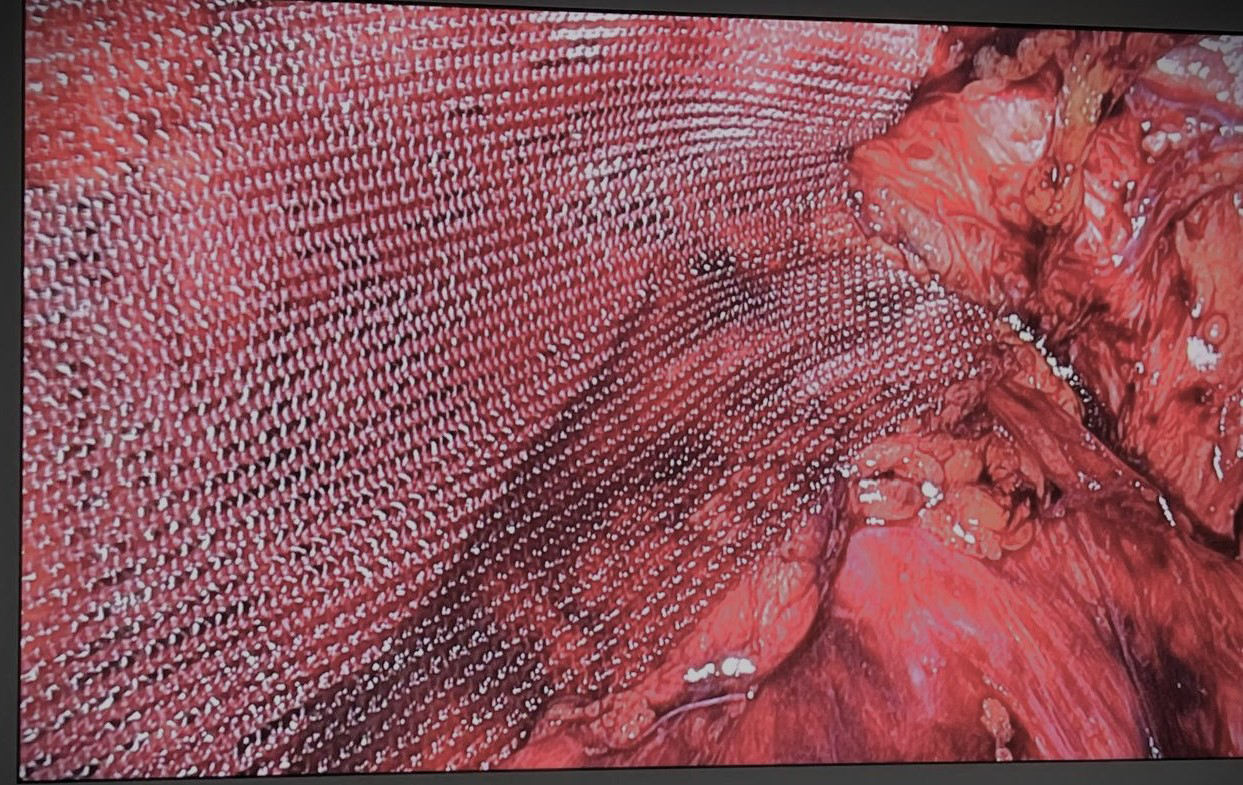
The mesh was inserted through a 10 mm trocar, avoiding skin contact (Figures 1 & 2). In the mesh fixation group fixations were made at Cooper’s ligament by an absorbable tacker (ETHICON Securestrap Absorbable strap fixation device) (Figures 3-5) medial to the inferior epigastric vessels and lateral to the inferior epigastric vessels to prevent nerve injuries and postoperative chronic pain.


(“ETHICON SECURESTRAP Absorbable Strap Fixation Device | Ethicon,” n.d.) Figure 3: Ethicon Securestrap Absorbable strap fixation device.

Post-operative Care and Follow-up
Following the surgery, patients were shifted to the ward on IV fluids and were allowed oral feeds when adequate bowel sounds were heard. Pain was measured on the Visual Analogue Scale on the 1st, 2nd, and 7th days. On the 3rd day, check-dressing was done, and the stitch line was evaluated for any seroma formation or wound infection. Patients were viewed after 1 week, at which time skin sutures were removed, and follow-up data was recorded. Further follow- up was done during the patient’s visit or by phone call.
Statistical Analysis
The study presented categorical variables in numbers and percentages, while quantitative data was presented as mean ± SD and median with 25th and 75th percentiles. Data normality was checked using the Shapiro-Wilk test, and nonparametric tests were used for non-normal data. Statistical tests were applied to compare quantitative and not normally distributed variables, and quantitative and normally distributed variables using the independent t-test. Qualitative variables were compared using Fisher’s exact test. Data entry was done in a Microsoft EXCEL spreadsheet, and the final analysis was done using SPSS software version 25.0. A p-value of less than 0.05 was considered statistically significant.
Observations and Result
Patients were randomly assigned into two groups 44 in the mesh fixation group and 52 in the non-fixation group. Our study compared the patients who underwent a mesh fixation procedure versus a non-fixation mesh procedure. The mean age was 41.98 ± 13.52 years in the fixation group and 42.81 ± 12.96 in non-fixation group, while the mean ± SD operation time was 85.84 ± 21.85 minutes in the mesh fixation group and
81.02 ± 21.99 minutes in the non-fixation group. The mean VAS score on day 1 was 2.7 ± 0.79 in the fixation group and 2.48 ± 0.78 in the non-fixation group. No significant difference was found between the groups concerning postoperative pain on days 1, 3, and 7, 1 month, 3 months. The mean dosage of injectable analgesic was 2.48 ± 0.63 in the fixation group and 2.54 ± 0.7 in the non-fixation group.
Complications such as port site infection and seroma were observed in 1 (2.27%) of patients in the fixation group and 1 (1.92%) in the non-fixation group. Delayed urinary retention and scrotal oedema were observed in 2(4.55%) of patients in the fixation group and 1(1.92%) in the non-fixation group. None of the patient (0/96) reported recurrence in both groups.
The cost of surgery was significantly different between the fixation and non-fixation groups. The mean duration of hospital stay was 2.07 ± 0.59 days in the fixation group and 2.1 ± 0.41 days in the non-fixation group. The mean duration for return to work was 3.62 ± 1.00 days in the fixation group and 3.54 ± 0.94 days in the non-fixation group showed no statistical significance.
| Variable | Parameter | Fixation (n=44) | Non- fixation (n=52) | P- value |
|---|---|---|---|---|
| Age | Years | 41.98 ± 13.52 | 42.81 ± 12.96 | 0.76 |
| Duration of surgery | Unilateral Hernia | 84.9 ± 19.84 | 79.9 ± 21.57 | 0.299 |
| Bilateral Hernias | 88.08 ± 26.82 | 109 ± 15.56 | 0.311 | |
| Mean ± SD | 85.84 ± 21.85 | 81.02 ± 21.99 | _ | |
| Pain (VAS-Score) | Day1 | 2.7 ± 0.79 | 2.48 ± 0.78 | 0.104 |
| Day3 | 0.84 ± 0.81 | 0.63 ± 0.79 | 0.176 | |
| Day7 | 0.02 ± 0.15 | 0.08 ± 0.27 | 0. 236 | |
| 3rdMonth | 0 | 0 | NA | |
| 6th Month | 0 | 0 | NA | |
| Frequency of Analgesics (Diclofenac 75mg) | Injectable | 2.48 ± 0.63 | 2.54 ± 0.7 | 0.656 |
| Oral | 4.64 ± 1.83 | 4.1 ± 1.76 | 0.145 | |
| Postoperative Complications | Infection | 1 (2.27%) | 1 (1.92%) | 1 |
| Seroma | 1 (2.27%) | 1 (1.92%) | 1 | |
| Urinary retention | 2 (4.55%) | 1 (1.92%) | 0.592 | |
| Scrotal oedema | 2 (4.55%) | 1 (1.92%) | 0.592 | |
| Recurrence | 0 (0%) | 0 (0%) | NA | |
| Hospital Stay | Duration in Days | 2.07 ± 0.59 | 2.1 ± 0.41 | 0.785 |
| Return To Work | Duration in Days | 3.7 ± 1.02 | 3.54 ± 0.94 | 0.41 |
| Cost of surgery | Indian rupees | 14088.41 ± 2752.67 | 11317.5 ± 1139.84 | 0.0001 |
| Readmission | Yes | 1 (2.27%) | 1 (1.92%) | 1 |
Table 1: Comparison of demographic features and perioperative data between the two groups of patients.
Discussion
The European Hernia Society recommends the TEP technique for laparoscopic hernia repair rather than the trans-abdominal preperitoneal technique because of the lower risk of visceral injury, port site hernia, and ileus with TEP [5]. Mesh fixation in the laparoscopic preperitoneal repair of inguinal hernias is a debatable issue. The stability of non-fixation mesh in TEP is primarily due to the sandwich effect and tissue incorporation. The mesh pressure between the peritoneal layer and the abdominal wall leads to the sandwich effect, stabilizing the mesh’s position and preventing movement. The need to fixation the mesh seems greater during the early postoperative period since with time there is significant tissue incorporation into the mesh [6]. Our study described the experience of a single surgeon performing laparoscopic TEP repair of inguinal hernias at our institution.
Our study did not find any difference in pain scores between the groups on day 1, day 3, 1 week, 1 month, or 3 months postoperatively. Some studies did demonstrate that chronic pain is greater in the mesh fixation group [7, 8]. Nerve entrapment by the tacks could be responsible for this [9, 10]. Taylor C, et al. [11] in a study demonstrated that chronic pain increases proportionately with the number of tacks used and was statistically significant. After a 3-month follow-up, there was no statistical difference observed between the two groups in a meta-analysis conducted by Lo CW, et al. [12] in 2019 involving ten trials and 1099 patients with 1467 hernias compared the efficacy and safety of mesh fixation and non-fixation in laparoscopic total extra peritoneal (TEP) hernia repair.
Our study did not show any difference in operative time between the two groups. Several factors must be taken into account when comparing operative time, including the use of mesh fixation, the nature of the hernia (primary vs. recurrent), the site of the hernia (unilateral vs. bilateral), and the complexity of the hernia (simple vs. combined). Among patients with a preoperative diagnosis of unilateral recurrent hernia, the bilateral repair was performed because a contralateral hernia was incidentally discovered intraoperative in 4.1% of patients. Diagnosing a potentially existing but preoperatively undiagnosed hernia is a clear advantage of laparoscopic repair.
In our study, injectable analgesics were administered on demand by the patient after assessing the VAS at 6, 24, and 72 hours of surgery. Injection of diclofenac 75 milligrams was given as an analgesic. In group A, the dose of injectable required ranged from 2-4 doses with a mean of 2.48 ± 0.63 doses and in group B, the dose of injectable analgesic ranged from 2-4 doses with a mean of 2.54 ± 0.7 (P-value 0.656) which was statistically insignificant. Kochar S, et al. [13] in 2020 a study showed no significant difference in postoperative analgesia required between the study groups.
In our study, 3 patients developed urinary retention two patients in the fixation group and one in the non- fixation group, and were treated by Foley’s catheter. The early complications developed in our work were seroma one in each group. Scrotal oedema was seen in two patients in the fixation group and one in the non-fixation group. Two patients developed port site infection one in each group and were successfully managed conservatively.
There was no statistically significant difference in mean hospital stay between the two groups. Eltair M, et al. [14] in 2019 conducted a study comparing laparoscopic repair of groin hernia with and without mesh fixation and found that the pooled analysis, which included 372 patients, demonstrated that there was no significant difference in length of hospital stay between the two groups. Dong H, et al. [15] in 2023 conducted a meta-analysis of 15 randomized controlled trials (RCTs) comparing non-fixation of mesh and fixation of mesh in laparoscopic total extra peritoneal (TEP) inguinal hernia repair found that there was no significant difference in hospital stay The mean duration for return to work was 3.7±1.02 days and 3.54±0.94 days respectively. The difference in return to work was not statistically significant with a p-value of 0.41. In a meta-analysis study conducted by Eltair M, et al. [14] in 2019, the study found that there was no significant difference in the time taken to return to normal activity between the two groups. Another study by Kumar A, et al. [16] in 2018, involved 122 patients who underwent laparoscopic inguinal hernia repair (IH) the difference in return to work was statistically insignificant with a p-value of 0.89.
Our study did not have any recurrence of hernia over a period of one year. Similarly, Gangopadhyay A, et al. [8] in 2018 conducted a comparison of non-fixation versus mesh fixation in TEP repair and observed no recurrence in either group. Taylor C, et al. [11] in 2008 conducted a multi-centre study involving 360 patients and found no difference in the risk of hernia recurrence at six months. Sahebally SM, et al. [7] in 2020 conducted a systematic review and meta- analysis that compared the effectiveness of mesh fixation versus no fixation in laparoscopic TEP inguinal hernia repair and found similar recurrence rates between the two groups. Lv Y, et al. [17] in 2024 conducted another meta-analysis of 18 randomized controlled trials involving 2617 patients and found no significant differences in recurrence rates for patients with smaller inguinal hernia orifices. Similarly, Dong H, et al. [15] in 2023 conducted a meta-analysis of 15 randomized controlled trials found no significant difference in recurrence rate between the non-fixation mesh and fixation mesh groups in laparoscopic TEP inguinal hernia repair.
In our study comparing the effects of mesh fixation and non-fixation in laparoscopic inguinal hernia repair, the cost of surgery in the non-fixation group was found to be significantly less than the cost of surgery in the fixation group (p-value <0.0001). Kochar S, et al. [13] in 2020, conducted a study showed that the procedure cost was significantly higher in Group A (mesh fixation) than in Group B (no mesh fixation) (p<0.001). Similarly, Taylor C, et al. [11] in 2008, conducted a study between 2004 and found that fixation increased operative costs by approximately 375 Australian dollars.
Conclusion
In TEP repair of inguinal hernias there is no significant difference between postoperative pain, frequency of analgesics administered, duration of in hospital-stay, return to work, complications and the hernia recurrence.
Mesh fixation repair is associated with increased operative costs.
References
-
Gavriilidis P, Davies RJ, Wheeler J, de’Angelis N, Di Saverio S (2019) Total extraperitoneal endoscopic hernioplasty (TEP) versus Lichtenstein hernioplasty: a systematic review by updated traditional and cumulative meta- analysis of randomised-controlled trials. Hernia 23(6): 1093-1103.
-
Tamme C, Scheidbach H, Hampe C, Schneider C, Kockerling F (2003) Totally extraperitoneal endoscopic inguinal hernia repair (TEP). Surg Endosc 17(2): 190- 195.
-
van den Heuvel B, Beudeker N, van den Broek J, Bogte A, Dwars BJ (2013) The incidence and natural course of occult inguinal hernias during TAPP repair. Surg Endosc 27(11): 4142-4146.
-
Tam K, Liang H, Chai C (2010) Outcomes of Staple Fixation of Mesh Versus Nonfixation in Laparoscopic Total Extraperitoneal Inguinal Repair: A Meta‐Analysis of Randomized Controlled Trials. World J Surg. 34(12): 3065-3074.
-
Simons MP, Aufenacker T, Bay-Nielsen M, Bouillot JL, Campanelli G (2009) European Hernia Society guidelines on the treatment of inguinal hernia in adult patients. Hernia 13(4): 343-403.
-
Garg P, Nair S, Shereef M, Thakur JD, Nain N, et al. (2011) Mesh fixation compared to nonfixation in total extraperitoneal inguinal hernia repair: a randomized controlled trial in a rural center in India. Surg Endosc 25(10): 3300-3306.
-
Sahebally SM, Horan J, Rogers AC, Winter D (2020) Fixation versus no fixation in laparoscopic totally extraperitoneal repair of primary inguinal hernia-a systematic review and meta-analysis of randomized controlled trials. Langenbecks Arch Surg 405(4): 435- 443.
-
Gangopadhyay A, Ghosh BC (2018) To compare advantage of non-fixation versus fixation of mesh in Laparoscopic totally Extra Peritoneal (TEP) repair of inguinal hernias. Asian J Med Sci 9(4): 35-40.
-
Stark E, Oestreich K, Wendl K, Rumstadt B, Hagmüller E (1999) Nerve irritation after laparoscopic hernia repair. Surg Endosc 13(9): 878-881.
-
Lantis JC, Schwaitzberg SD (1999) Tack Entrapment of the Ilioinguinal Nerve during Laparoscopic Hernia Repair. J Laparoendosc Adv Surg Tech 9(3): 285-289.
-
Taylor C, Layani L, Liew V, Ghusn M, Crampton N, et al. (2008) Laparoscopic inguinal hernia repair without mesh fixation, early results of a large randomised clinical trial. Surg Endosc 22(3): 757-762.
-
Lo CW, Tsai YC, Yang SSD, Hsieh CH, Chang SJ (2019) Comparison of short- to mid-term efficacy of nonfixation and permanent tack fixation in laparoscopic total extraperitoneal hernia repair: A systematic review and meta-analysis. Tzu Chi Med J 31(4): 244-253.
-
Kochar S, Kakkar D, Singh DP (2020) Evaluation of mesh fixation versus non-fixation in laparoscopic mesh hernioplasty in inguinal hernias. Int Surg J 7(10): 3354- 3359.
-
Eltair M, Hajibandeh S, Hajibandeh S, Balakrishnan S, Alyamani A, et al. (2019) Meta-analysis of laparoscopic groin hernia repair with or without mesh fixation. Int J Surg 71: 190-199.
-
Dong H, Li L, Feng HH, Wang DC (2023) Safety of unfixed mesh in laparoscopic total extraperitoneal inguinal hernia repair: A meta-analysis of randomized controlled trials. Surg Open Sci 16: 138-147.
-
Kumar A, Kaistha S, Gangavatiker R (2018) Non-fixation versus Fixation of Mesh in Totally Extraperitoneal Repair of Inguinal Hernia: a Comparative Study. Indian J Surg 80(2): 128-133.
-
Lv Y, Yang B, Hao G, Wang Y (2024) Mesh Fixation versus Nonfixation in Laparoscopic Inguinal Hernia Repair: A Systematic Review and Meta-Analysis. Am Surg 90(1): 111-121.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review