Diagnostic and Surgical Challenges of a Lumbar Extradural Hydatid Cyst: A Case Report and Review of Literatures
Spinal hydatid cysts, though uncommon, are a serious condition. An 14-year-old boy experienced back pain, increasing weakness, and numbness in his legs. Lumbar region MRI revealed a cystic lesion with a regular outline in the extradural space, exhibiting T1-weighted images showed a lesion that was hypointense, while T2-weighting images displayed hyperintense. The lesion severely compressed the dural sac and caudal roots, extending into the L3 and L4 neural foramina. The condition was addressed through an L3 laminectomy and completely removing the hydatid cyst. This report discusses the clinical symptoms, diagnostic process, and surgical treatment of this rare spinal hydatid disease case, along with a review of all documented primary extradural hydatid cyst cases in the literature.
Abbreviations
MRI: Magnetic Resonance Imaging; H&E: Hematoxylin and Eosine; ELISA: Enzyme-Linked Immunosorbent Assay.
Introduction
Human echinococcosis is a major health issue and an endemic condition in Iran. The tapeworm Echinococcus multilocularis causes most hydatid disease cases [1]. Though it rarely impacts bone tissue, affecting only 0.5% to 2% of cases, the vertebral column is involved in 45% of these instances. Spinal hydatid cysts are located most commonly at the thoracic (52%), followed by the lumbar (37%) and then the cervical and sacral levels [2]. These lesions can break through the bony wall, entering the spinal canal and pressing on the spinal cord and intraspinal roots, while usually leaving the dura intact. Intrathecal cysts are extremely uncommon [3].
Despite advancements in spinal surgery and drug treatments, the infiltrative nature of spinal involvement in this disease complicates achieving a cure and heightens the risk of recurrence [4]. Braithwaite and Lees have classified the spinal involvement by hydatid disease in Five groups: (a) primary intramedullary hydatid cyst; (b) intradural extramedullary hydatid cyst; (c) extradural intraspinal hydatid cyst; (d) hydatid disease of the vertebrae; (e) paravertebral hydatid disease [5]. In this paper, we report one case of primary extradural intraspinal hydatid cyst.
Although this condition is uncommon, it is severe and can have devastating consequences. Reviewing case series and reports is essential for developing effective treatment strategies for this infectious disease.
Case Present
A 14- year-old country boy is presented to Qa’em Hopspital in June 2024. He was admitted to our clinic because of persistent pain and paresthesia of the lower extremities and progressive difficulty with walking which had intensified over the past month.
The neurological examination showed reduced sensation around the perianal area and paraparesis, more pronounced on the right side and in the distal muscle groups. The patient exhibited normal patellar and Achilles relaxes, without any urinary and fecal incontinence. The patient complains of severe pain, paresthesia in the anterior thigh both lower limbs, especially the right lower limb, and inability to walk.
On neurological examination, there was no weakness in the lower limbs and no sensory impairment. He also didn’t have sphincter disturbances.
Patient doesn’t mention fever or weight loss in recent months. The patient lives in a rural environment and has various animals, including dogs and sheeps. A general physical examination revealed nothing. All the patient’s lab tests, including WBC, erythrocyte sedimentation rate and C-reactive protein levels were within normal ranges.
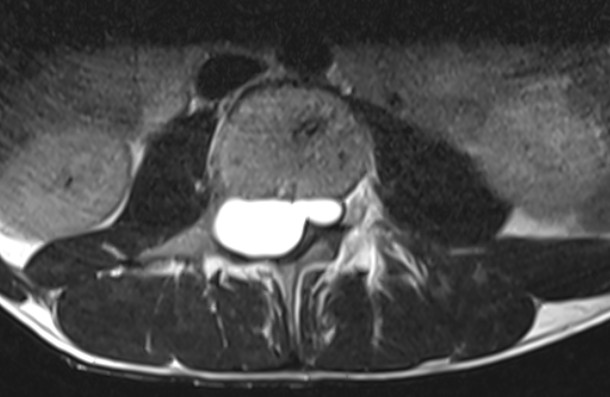
Abdominal ultrasonography and Brain magnetic resonance imaging (MRI) were normal. However, an MRI of the lumbar area depicated a cystic lesion within the lumbar spinal canal, measuring 3.2 cm vertically and 1.5 cm horizontally, with an extradural location, which caused compression of the thecal sac. T1-weighted images showed a lesion that was hypointense, while T2-weighting images displayed hyperintense (Figure 1). Lesion leads to significantly compressed the dural sac and caudal roots and extended into the L3 and L4 neural foramina without involving the bone (Figure 1).
The patient underwent an L3 laminectomy to explore and excise the lesion. The cyst was completely and without rupture removed along with a Fibrous pseudocapsule that was firmly adhered to the dural sac and bone. Cystic epidural lesion was observed below the L3 root. The cyst was resected and the site was washed with hypertonic saline. The surgical specimen measured 3*1.5 cm and was identified as a semitransparent, white, pearl-like, cystic substance which was thought to be parasitic. The cavity was subsequently irrigated with hypertonic saline. Histopathological analysis confirmed the diagnosis of a hydatid cyst. Histopathological analysis revealed that Hematoxylin and Eosine (H&E) stainted the wall of the cyst. The cyst wall contained eosinophilic inflammatory cells that indicated a severe inflammation, while the eosinophilic laminar membranous material located in granular eosinophilic debris, which supported a diagnosis of hydatidosis. Although, serological tests (specific ELISA/ Western blot) returned negative results. Postoperatively, albendazole treatment was initiated early. His neurological condition improved after the operation and he was discharged with instructions to continue receiving anthelmintic treatment with albendazole (400 mg twice a day).
Discussion
We presented a rare manifestation of hydatid cyst in lumbar region. Human beings are accidental intermediate hosts. Spinal hydatid cysts account for 1 % of all cases of hydatid disease [6]. Hydatid cysts are usually located at the thoracic level (52%), followed by the lumbar (37%), and then the cervical and sacral levels [7]. It affects both sexes equally, but is seen more often in the younger population [8].
Due to the lack of specific clinical manifestations of the spinal hydatid disease, clinical suspicion alone may only guide neurosurgeons for the management of these patients [6, 7]. Symptoms related to the spinal cord compression may be observed in a wide spectrum from numbness to motor deficit’s. Although the First symptoms are backache and radicular pain commonly, weakness of the lower extremities is observed towards the terminal stage of the spinal hydatid disease [9].
Radiological studies are generally inconclusive, but they may aid in diagnosing hydatid disease.
Laboratory tests such as ELISA, indirect hemagglutination and complement fixation tests are reported to be 80–100 % sensitive and 88–96 % specific in abdominal disease [3]. However, the sensitivity decreases abruptly to 25–56 % in extrahepatic disease which limits their use in the diagnosis or follow up for primary bone disease [3]. The best preoperative diagnostic procedure is MR [10, 11]. The MRI images of the lesions were reviewed by Berk C, et al. [12] who discripted that they had a distinctive shape: sausage-like shape with two dome- shaped ends, thin and regular walls, but no septation or debris in the lumen.
The lesions are occasionally spherical. The cyst content and CSF signal characteristics are typically similar. The cyst wall may exhibit a high signal in T1-weighted images and has fewer signals than its contents. Additionally, T2-weighting images reveal primarily refracting the same high-signal cyst content with contrasting low intensity. T2-weighted images demonstrate the possibility of survival, with a decrease in high signal and an increase in low signal from collapsed cyst walls being indicative of cured cysts. The contrast on the cyst wall is slightly enhanced. The low-signal rim on T2-weighted images is associated with the histopathological examination and is indicative of reactive Yibrosis and degeneration surrounding the parasitic membrane [12]. The only effective therapeutic option for treating this condition is surgery where the cyst is removed without rupture while maintaining the integrity of the cyst wall [1, 2, 13]. A laminectomy is typically the preferred procedure to alleviate compression caused by cysts [14, 15]. The recurrence of cysts can be prevented by carefully dissecting and irrigation around the cyst [16, 17]. The surgical area should be irrigated with hypertonic saline if cysts rupture during intervention, but this appears to have no impact as it will only cause recurrence once the cyst is embedded in the intradural space [18]. Adjuvant anthelminthic therapy with mebendazole and albendozole is preferred to combine surgical treatment to prevent potential recurrences [13, 19, 20, 21].
Although hydatid cyst is characterized as benign pathologies, the high risk of dissemination and increased likelihood of recurrences make the condition potentially malignant. The high mortality and morbidity rates caused by this benign pathology are a result of the repetitive surgical procedures [22].
Conclusion
Lumbar extradural hydatid cysts are rarely mentioned in the literature. The primary treatment for hydatid cysts involves surgical intervention, requiring complete removal without rupture. Despite negative serological tests, hydatid cysts should be included in the differential diagnosis of cystic spinal lesions, given the distinct clinical and neuroradiological characteristics.
References
-
Moosazadeh M, Abedi G, Mahdavi SA, Shojaee J, Charkame A, et al. (2017) Epidemiological and clinical aspects of patients with hydatid cyst in Iran. Journal of Parasitic Diseases 41(2): 356-360.
-
Caglar YS, Ozgural O, Zaimoglu M, Kilinc C, Eroglu U, et al. (2019) Spinal hydatid cyst disease: challenging surgery-an institutional experience. Journal of Korean Neurosurgical Society 62(2): 209-216.
-
Lotfinia I, Sayyahmelli S, Mahdkhah A, Shoja MM (2013) Intradural extramedullary primary hydatid cyst of the spine: a case report and review of literature. European Spine Journal 22(3): 329-336.
-
Kafaji A, Al-Zain T, Lemcke J, Al-Zain F (2013) Spinal manifestation of hydatid disease: a case series of 36 patients. World neurosurgery 80(5): 620-626.
-
Braithwaite P, Lees RF (1981) Vertebral hydatid disease: radiological assessment. Radiology 140(3): 763-766.
-
Jain A, Prasad G, Rustagi T, Bhojraj SY (2014) Hydatid disease of spine: Multiple meticulous surgeries and a long term followup. Indian journal of orthopaedics 48(5): 529-532.
-
Scarlata F, Giordano S, Saporito L, Marasà L, Li Pani G, et al. (2011) Cystic hydatidosis: a rare case of spine localization. Infez Med 19(1): 39-41.
-
Zali A, Shahmohammadi M, Biazar BH, Masoumi N, Samieefar N, et al. (2023) Spinal hydatid cyst initially diagnosed as spinal tumor: A case report and review of the literature. Clinical Case Reports 11(5): 7244.
-
Padayachy LC, Ozek MM (2023) Hydatid disease of the brain and spine. Child’s Nervous System 39(3): 751-758.
-
Sharma RM, Khalid S, Sarmast AH, Modi M, Rafeeque R (2017) Multiple primary intraspinal extradural hydatid cyst in a young patient. Journal of Spinal Surgery 4(3): 133-135.
-
Gunecs M, Akdemir H, Tugcu B, Gunaldi O, Gumucs E, et al. (2009) Multiple intradural spinal hydatid disease: a case report and review of literature Spine 34(9): E346-E350.
-
Berk C, Erdogan A (1998) MRI in primary intraspinal extradural hydatid disease: case report. Neuroradiology 40(6): 390-392.
-
Baykaner M, Dogulu F, Ozturk G, Edali N, Tali T (2000) A viable residual spinal hydatid cyst cured with albendazole. J Neurosurg Spine 93(S1): 142-144.
-
Pamir MN, Akalan N, Ozgen T, Erbengi A (1984) Spinal hydatid cysts. Surg Neurol 21(1): 53-57.
-
Dauchy FA, Pointillart V, Malvy D (2013) Vertebral echinococcosis leading to spinal cord compression. Eur Spine J 22(3): 667-668.
-
Taghipour M, Zamanizadeh B, Bagheri M, Zare Z (2005) Hydatid cyst of the foramen magnum case report. Neurosurg Q 15: 110-112.
-
Prabhakar M, Acharya A, Modi D, Jadav B (2005) Spinal hydatid disease: A case series. J Spinal Cord Med 28(5): 426-431.
-
Islekel S, Zileli M, Esahin Y (1998) Intradural spinal hydatid cysts. Eur Spine J 7(2): 162-164.
-
Altinors N, Bavbek M, Caner HH, Erdoğan B (2000) Central nervous system hydatidosis in Turkey: a cooperative study and literature survey analysis of 458 cases. J Neurosurg 93(1): 1-8.
-
Pandey M, Chaudhari MP (1997) Primary hydatid cyst of sacral spinal canal: case report. Neurosurgery 40(2): 407-409.
-
Garcia-Vicuna R, Carvajal I, Ortiz-Garcia A, Lopez- Robledillo JC, Laffon A, et al. (2000) Primary solitary echinococcosis in cervical spine. Postsurgical successful outcome after long-term albendazole treatment. Spine 25(4): 520-523.
-
Farajirad E, Farajirad M, Khajavi M, Shojaie SRH (2016) Central Nervous System Hydatid Disease: Clinical Analysis of 99 Cases in Qaem Hospital of Mashad University of Medical Sciences, Iran. Neurosurgery Quarterly 26(1): 1-4.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review