Nerve-Preserving Superomedial Pedicle Breast Reduction Approach for Chest Wall Masculinization: A Case Report
Introduction: Gender affirming chest surgeries are a treatment for transgender and gender diverse individuals who suffer from gender dysphoria. Double incision mastectomy with free nipple grafts is the most common technique used for masculinization of the chest for Fischer grade 2B to 4 patients. However, this technique sacrifices the nerves to the nipple-areolar complex (NAC). While multiple nipple pedicles have been described in cisgender reduction mammoplasty, only an inferior pedicled mammaplasty approach has been described for chest wall masculinization for Fischer grade 2B to 4 patients. Case Presentation: We describe the surgical technique of a superomedial pedicle chest masculinization surgery for an individual with Fischer grade 2B breasts. Sensation was preserved at 2-weeks post-surgery. At 4-months, using a 0 to 10 numeric rating scale, patient satisfaction was 9 for the overall cosmetic outcome and a 9 for the masculinization. Using inferior sternum sensation as a reference (10), areola sensation on the superior side adjacent the nipple was a 6.5 on the right and an 8 on the left. Chest sensation was a 10 in the superolateral, inferolateral, and superomedial quadrants bilaterally, and was an 8 in bilateral inferomedial quadrants. 2-point discrimination of the areola was assessed on the inferior side adjacent the nipple and was 13mm on the left and 14mm on the right. Semmes-Weinstein monofilament testing of the areola was performed adjacent to the nipple superiorly (R: 4.31, L: 4.56), inferiorly (R: 4.31, L: 6.65), medially (R: 4.31, L: 6.65), and laterally (R: 4.31, L: 6.65). Conclusion: A mastectomy technique using a superomedial pedicle can preserve the nerve to the nipple-areolar complex to retain sensation while providing sufficient cosmetic outcome.
Introduction
In recent years, gender affirmation surgeries (GAS) have been increasingly performed as a treatment for transgender and gender diverse individuals who suffer from gender dysphoria [1]. These surgeries present a wide array of chest, genital, and facial feminizing and masculinizing procedures [1].
Gender affirming chest surgeries have similarities to breast augmentation and mastectomy surgeries common to plastic surgeons, but differ in the contour, nipple-areolar position, presence or absence of an inframammary fold, and quality of the breast skin if affected by breast binding [2, 3, 4]. Double incision mastectomy with free nipple grafting is the most common chest masculinization technique and is frequently utilized for Fischer grade 2B to 4 patients [3, 4, 5, 6].
However, this technique sacrifices the nerves to the nipple-areolar complex (NAC). While multiple nipple pedicles have been described in cisgender reduction mammoplasty, only an inferior pedicled mammaplasty approach has been described for chest wall masculinization for Fischer grade 2B to 4 patients [3, 7, 8].
We describe a superomedial pedicled NAC technique of chest masculinization for transgender patients with larger breasts that preserves the anterior branch of the intercostal nerves to leave NAC sensation intact.
Case Presentation
All institutional and governmental regulations for ethical human subject research were followed. Written consent was obtained from the patient for publication of this case report and any accompanying images.
Case Report
A 25-year old (body weight of 120 pounds) individual was assessed for a female-to-male chest surgery. Medical history included gender dysphoria, antiphospholipid syndrome, Henoch-Schönlein Purpura, Addison’s disease, thoracic compression fracture, May-Thurner syndrome, deep vein thrombosis, and long-term anticoagulant use. Medications were corticosteroids and warfarin. Preoperative physical examination showed Fischer grade 2B breasts with good symmetry. The patient was adamant about preserving his nipple sensation irrespective of the surgical technique.
Surgical options discussed included a double-incision mastectomy with free nipple grafts (FNG) with a staged nerve graft to restore nipple sensation, or a breast reduction with a superomedial flap to maximize chances of preserving nipple sensation. Patient’s preference was for a superomedial flap breast reduction. Risks discussed included a less flat, more androgynous chest compared with the double-incision mastectomy approach.
Owing to the complex medical history, endocrinology and hematology were consulted and subsequent surgical clearance and risk stratification were obtained with recommendations for changing anticoagulants and increasing hydrocortisone perioperatively.
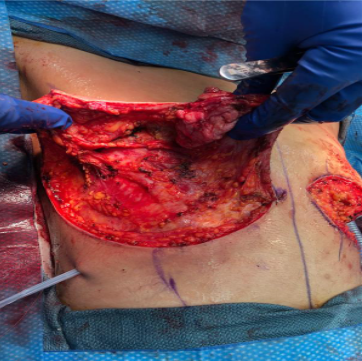
Surgical Technique
A superomedial pedicle was de-epithelialized, and breast tissue was removed in a vertical resection pattern, and a wise skin excision (Figure 1). To achieve a masculine-appearing chest, the superomedial pedicle and the lateral breast flap were both thinned to a 2-cm thickness; the superomedial pedicle was meticulously thinned with blunt dissection used to prevent transecting nerve branches as breast parenchyma and fat lobules were excised. The nipple was rotated to its new position, inset, and excess inframammary skin was removed to create a 3-cm nipple to inframammary fold distance. Jackson-Pruitt (JP) drains were placed bilaterally.
Post-Operative Outcomes
At 2-weeks follow-up, chest and nipple sensation were intact. At 4-months follow-up, using a 0 to 10 numeric rating scale, patient satisfaction with the overall cosmetic outcome, was rated as a 9, with the achieved masculinization was a 9. Using inferior sternum sensation as a 10, areola sensation on the superior side adjacent the nipple was a 6.5 on the right and an 8 on the left. Chest sensation was a 10 in the superolateral, inferolateral, and superomedial quadrants bilaterally, and was an 8 in bilateral inferomedial quadrants. 2-point discrimination of the areola was assessed on the inferior side adjacent the nipple and was 13mm on the left and 14mm on the right. Semmes-Weinstein monofilament testing of the areola was performed adjacent to the nipple superiorly (R: 4.31, L: 4.56), inferiorly (R: 4.31, L: 6.65), medially (R: 4.31, L: 6.65), and laterally (R: 4.31, L: 6.65).
Discussion
Masculinizing chest surgery improves gender dysphoria, health related quality of life, self-esteem and body image, and may be lifesaving [9, 10, 11]. The described superomedial pedicle chest wall masculinization technique of larger breasts helps in the preservation of the innervation and sensation of the NAC. This report provides an alternative method to the previously described inferior pedicle mammoplasty [3, 7, 8]. Wright, et al. reported in 2018 that over 70% of patients retained nipple sensation and erectile function [8], specific outcome measures of sensation have not been reported for the chest wall masculinization flap technique [3, 7]. The several subjective and objective measures of clinically meaningful preservation of sensation are therefore a strength of the present report. The described technique may provide superior preservation of sensation when a thin pedicle is needed.
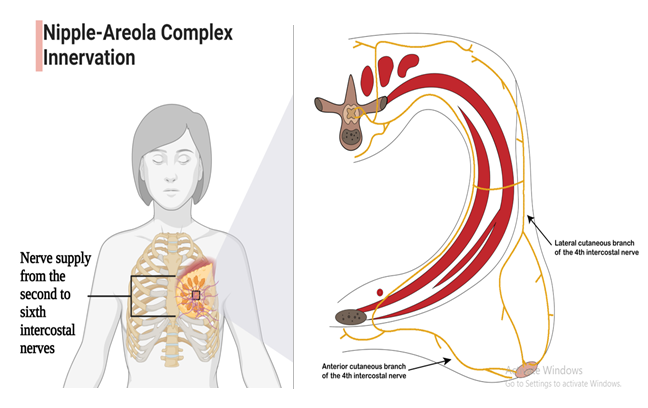
NAC innervation, although variable and incompletely understood, arises via nerve branches of the 3rd, 4th, and 5th intercostal nerves [12]. Intercostal nerves divide into lateral and anterior cutaneous branches (LCB and ACB, respectively) that exit the deep fascia at the midaxillary line and parasternal line, respectively. The ACB sends a lateral branch inferolaterally to the NAC [12]. The LCB divides into posterior and anterior branches, and off of the anterior branch are superficial and deep branches that course to the NAC (Figure 2) [12]. A subdermal plexus that innervates the NAC has been described [13, 14, 15, 16]. Although not always found and debatable whether truly present Farina, et al. [17, 18, 19] is suggested by NAC sensation remaining intact despite simultaneous nerve block of multiple intercostal nerves [20]. Because the nerves to the nipple course from lateral and medial directions, we propose the possibility of increased sensory preservation from more axial-plane oriented flaps, such as the superomedial flap, than craniocaudally oriented flaps.
Despite being erogenous, the areola and the nipple are physiologically less sensitive than other chest areas [21] which explains why our measured findings were less in the areola than in the inferior sternum. Our outcomes were assessed at 4-months, a time-frame sufficient for any iatrogenically disrupted myelin to recover [22]. Suggesting
normal physiologic asymmetry contributing to the slight difference in sensation between the left and right areolas or considerations related to flap dimensions. This case report is limited by a lack of preoperative assessments, so additional larger studies with outcome assessments are needed.
Conclusion
For patients requesting NAC sensation preservation, a thin, superomedial pedicled NAC with rigorous dissection to preserve intercostal nerve branches to the NAC may be considered.
Established Facts
Masculinizing mastectomy for female-to-male transitioning individuals is a potentially life-saving and quality-of-life improving surgical procedure.
Fischer grade 2B-4 individuals undergoing masculinizing mastectomy are most often offered free-nipple-grafts that leave the nipple-areolar complex insensate, or an inferior pedicle approach which may preserve some sensation to the nipple-areolar complex.
Novel Insights
A superomedial pedicle allows preservation of a nerve innervating the nipple-areolar complex and may be the preferred technique for Fischer grade 2B-4 individuals desiring a masculinizing mastectomy.
At 4-months post-surgery, subjective sensation, 2-point discrimination, and Semmes-Weinstein monofilament testing were preserved to the areola.
Statement of Ethics
All institutional and governmental regulations for ethical human subject research were followed. This report describes a single case outcome and does not quality for human subjects research requirements for ethical board approval.
Written Informed Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Ethical Review Board
This report describes a single case outcome and does not quality for human subjects research requirements for ethical board approval.
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Funding Statement
No funding was involved in this report.
Author Contributions Statement
Clinical and operative tasks were performed by Salam Al Kassis and Patrick E. Assi; Data collection was by Adam G. Evans and Benjamin C. Park; Primary manuscript writing was by Adam G. Evans, Benjamin C. Park and Mariam Saad; with revisions and critical concept development by Patrick E. Assi and Salam Al Kassis; Figure drawing was by Benjamin C. Park with revisions by Patrick E. Assi and Adam G. Evans.
Data Statement
All data generated or analysed during this study are included in this article. Further inquiries may be directed to the corresponding author.
References
-
American Society of Plastic Surgeons ( 2020) Plastic Surgery Statistics Report.
-
Lewin R, Amorosa M, Plate N, Trogen C, Selvaggi G (2020) The Aesthetically Ideal Position of the Nipple-Areola Complex on the Breast. Aesthetic Plast Surg 44(4): 1130- 1138.
-
Claes KEY, Arpa SD, Monstrey SJ (2018) Chest Surgery for Transgender and Gender Nonconforming Individuals. Clin Plast Surg 45(3): 369-380.
-
Monstrey S, Selvaggi G, Ceulemans P, Landuyt KV, Bowman C, et al. (2008) Chest-wall contouring surgery in female-to-male transsexuals: a new algorithm. Plast Reconstr Surg 121(3): 849-859.
-
Avarez IMP, Zolper EG, Schwitzer J, Fan LK, Corral GAE (2021) Incidence of Complications in Chest Wall Masculinization for the Obese Female-to-Male Transgender Population: A Case Series. World journal of plastic surgery 10(2): 14-24.
-
Langner BR, U Berli J, Sabino J, Chopra K, Singh D, et al. (2017) Top Surgery in Transgender Men: How Far Can You Push the Envelope? Plast Reconstr Surg 139(4): 873e-882e.
-
Kuhn S, Keval S, Sader R, Kuenzlen L, Kiehlmann M, et al., (2019) Mastectomy in female-to-male transgender patients: A single-center 24-year retrospective analysis. Arch Plast Surg 46(5): 433-440.
-
Wright C, Williams K, Dabritz G (2018) The inferior dermal flap technique for trans male chest contouring. Annals of the Royal College of Surgeons of England 100(2): 157-158.
-
Coleman E, Bockting W, Botzer M, Kettenis PC, Decuypere G, et al. (2012) Standards of Care for the Health of Transsexual, Transgender, and Gender- Nonconforming People, Version 7. International Journal of Transgenderism 13(4): 165-232.
-
Newfield E, Hart S, Dibble S, Kohler L (2006) Female- to-male transgender quality of life. Qual Life Res 15(9): 1447-1457.
-
Agarwal C, Scheefer MF, Wright LN, Walzer NK, Rivera A (2018) Quality of life improvement after chest wall masculinization in female-to-male transgender patients: A prospective study using the BREAST-Q and Body Uneasiness Test. J Plast Reconstr Aesthet Surg 71(5): 651-657.
-
Schlenz I, Kuzbari R, Gruhber H, Holle J (2000) The Sensitivity of the Nipple-Areola Complex: An Anatomic Study. Plastic and Reconstructive Surgery 105(3): 905- 909.
-
Michelle le Roux C, kill BJ, Pan WR, Rozen WM, Ashton MW (2010) Preserving the neurovascular supply in the Hall-Findlay superomedial pedicle breast reduction: an anatomical study. J Plast Reconstr Aesthet Surg 63(4): 655-662.
-
Cooper AP (1840) Anatomy of the Breast. Johns Hopkins Medicine.
-
Pandya S, Moore RG (2011)Breast development and anatomy. Clin Obstet Gynecol 54(1): 91-95.
-
Sarhadi NS, Dunn JS, Lee FD, Soutar DS (1996) An anatomical study of the nerve supply of the breast, including the nipple and areola. Br J Plast Surg 49(3): 156-164.
-
Farina MA, Newby BG, Alani HM, (1980) Innervation of the nipple-areola complex. Plast Reconstr Surg 66(4): 497-501.
-
Craig RD, Sykes PA (1970) Nipple sensitivity following reduction mammaplasty. Br J Plast Surg 23(2): 165-172.
-
Jaspars JJ, Posma AN, Immersesl AAV, Groot ACG (1997) The cutaneous innervation of the female breast and nipple-areola complex: implications for surgery. Br J Plast Surg 50(4): 249-59.
-
Bijkerk E, Cornelissen AJM, Sommer M, Hulst RRWJ, Lataster A, et al. (2020) Intercostal nerve block of the anterior cutaneous branches and the sensibility of the female breast. Clin Anat 33(7): 1025-1032.
-
Tairych GV, Kuzbari R, Rigel S, Todoroff BP, Schneider B, et al. (1998) Normal cutaneous sensibility of the breast. Plast Reconstr Surg 102(3): 701-704.
-
Dy CJ, Mackinnon SE (2016) Ulnar neuropathy: evaluation and management. Current reviews in musculoskeletal medicine 9(2): 178-184.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication