Late Onset of Lower Limb Infection Caused by Gluteal Augmentation with Polyalkylimide Gel (PAIG), A Case Report
Background: Soft tissue augmentations with liquid injectibles is a common method for the treatment of lipodystrophy in HIV positive patients. Especially PAIG injections in small volumes have been used for this purpose and have been an established treatment. We report an unusual case of a complication 15 years after bilateral gluteoplasty by PAIG injection. PAIG as a volume replacement for aesthetic procedures as well as for the treatment of facial lipodystrophy has been used for a long time. A broad experience has been gained and few complications have been reported so far therefore it is an established and reliable procedure. Today’s plastic surgeon has a wide range of liquid injectibles and alternate procedures to choose from. Volume augmentation by hyaluronic acid, collagen and especially autologous fat grafting are more common in Europe and North America. Material and methods: We present a case report of a patient treated in our department for lower limb infection due to a long term complication after bilateral gluteoplasty by polyalkylimde injection. Verbal consent was obtained from the patient. Results: We report an unusual case of a complication 15 years after bilateral gluteoplasty by PAIG injection. Our case reports a descending abscess on the left inferior member in a male patient of Asian descent. Typical silicone associated granulomas were absent. Histopathology revealed foreign body tissue reaction untypical for silicone. A second survey of the patient’s history indicated previous PAIG injections for gluteoplasty. A radical surgical approach was crucial for the cure. Conclusion: Our case shows that plastic surgeons have to be aware of alternate augmentation methods and procedures in patients of foreign descent especially Asia and its associated potential complications. Those might include unusual materials like PAIG or silicone and respective different injection areas, as well. Treating those patients means to consider material migration with unusual clinical presentation of the complication. Consideration of cultural particularities and thoroughly empathetic and perceptive history taking is a crucial condition for the correct diagnosis and consecutive therapy.
Introduction
Liquid injectibles (“fillers”) for soft tissue augmentation especially have been used for over 5 decades therefore broad experience has been gained [1].
Volume replacement by Polyalkylimide (PAIG) injections is an established treatment for HIV patients suffering from lipodystrophy. This had significant impact on quality of life of those patients [2]. Polyalkylimide is an hydrogel polymer of non-biodegradable properties consisting of 4 % alkylimide groups and mostly (96 %) pyrogen-free water [3]. It has been used widely as a treatment for HAART therapy related facial lipodystrophy (or- atrophy) syndrome (FLA) and relatively few complications have been reported so far [3, 4]. Even fewer cases have been described on complications after gluteal injections with PAIG for gluteal lipodystrophy treatment in HIV positive patients [5] (Figure 1).
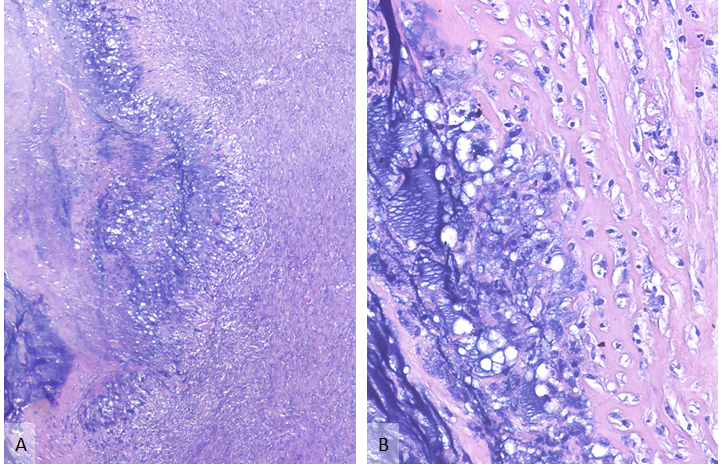
Figure1A: Necrotic fascia (left) was aligned with blue acellular material (center) next to inflamed and scared viable fibrous tissue (right). Figure 1B: On high power, at the border of foreign material, histiocytes, lymphocytes and neutrophils were present without formation of typical foreign body granulomas. (embedding in paraffin wax, stain: hematoxylin and eosin, original magnification: A. 40x, B. 200x).
We describe a long-term complication after PAIG injections for gluteal augmentation in an HIV negative individual.
Case Presentation
A 44-year old male Asian patient and member of the LGBTQ community presented to our emergency department with pain and local inflammatory signs of the left thigh. According to the patient’s history he suffered a mosquito bite a few days ago that led to scratching and supposedly progressed to the presentation of a super infected wound that produced a slight putrid secretion.
The patient had a history of previous breast augmentation with saline implants around 10 years ago. No proper medication at admission, no allergies known.
On clinical examination we found a perforated abscess located above the left medial knee with regional erythema and swelling of the distal inner and ventral thigh. ROM of the left hip and knee joint didn’t show any restrictions, there were no signs indicating any intraarticular effusion. The patient didn’t report any limitations at walking.
Laboratory findings presented normal WBC with 9.8 G/ ml, C-reactive protein was elevated with 96 mg/l, fever was absent. A screening for HIV, Hepatitis B and C were negative.
Echography was performed revealing an abscess formation in the subcutaneous tissue of the ventral and medial thigh with dimensions of 20 cm x 3 cm and a depth of 1,5 cm. Its expansion reached from the groin to the perforation area right above the left ventromedial knee.
Emergency surgery was performed on the day of admission. The abscess was incised, excess pus was drained. There were no granulomas detectable as expected in a foreign body reaction due to silicone. Specimen for microbiological and histopathological examination were preserved, a drain was installed and we decided to close the wounds primarily. On the ward the patient was treated with an antibiotic regimen consisting ampicillin and clavulanic acid. Drains could be removed on the 3rd day, local inflammation signs receded and pain was significantly reduced.
Histopathological findings indicated a foreign body reaction with typical lymphatic cell and plasma cell infiltration with multinucleated giant cells and vast vascular proliferation around foreign bodies in the subcutaneous tissue. Granuloma like lesions could not be seen. Lymphadenopathy was absent. Microbiology testing was negative.
An MRT scan of the thighs was performed to detect any foreign body. Remaining fluid formations in the groin area and subcutaneous foreign body like formations of the ventromedial thigh could be seen (Figure 2).
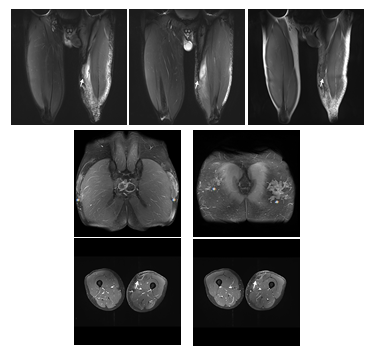
Figure 2: Magnetic resonance imaging indicates contrast enhanced liquid formations of the left groin area descending to the medial and ventromedial thigh. An Abscess formation of the proximal ventral thigh can be seen (↑). Enlarges lymphatic nodules of both sides are present. Extended bilateral foreign body inclusions in the subcutaneous tissue in the pelvic area and gluteal region are detectable (*).
The patient indicated another aesthetic procedure about 15 years ago. He had undergone a bilateral gluteoplasty by injection of an unknown quantity of polyalkylimide gel (PAIG) of unknown purity.
We performed a pelvic X-ray that showed no opaque calcified formations in the gluteal area or any gas formation within the subcutaneous tissues. Echography of the groin revealed enlarged lymphatic nodes that were slightly painful on palpation and a band-like hypoechoic lesion in the subcutaneous tissue was seen from the pelvic region through the groin reaching ventromedially down to the medial knee.
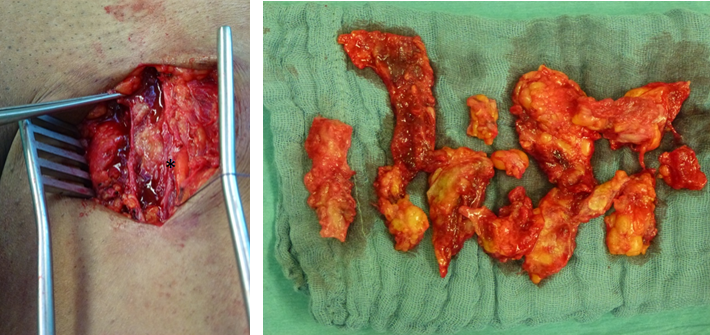
We performed a second operation on the 5th postoperative day for thorough debridement of involved subcutaneous tissue and abscess in the groin.
We found remaining turbid secretion enclosed in the subcutaneous tissue reaching from the groin area down to the medial knee (Figure 3).
Histopathological findings showed typical PAIG inclusions in an inflammatory subcutaneous pannus. Histology of the involved lymphatic nodes revealed multinucleated giant cells surrounding a basophile non polarizing foreign material.
The subsequent antibiotic treatment was continued, the drains could be removed and the patient could be discharged on the 4th postoperative day with bland wounds and missing signs of local inflammation. The patient was advised to continue antibiotic treatment by orally administered amoxicillin and clavulanic acid for 10 days. Stitches were removed 14 days after the last surgical intervention.
Follow-up showed excellent outcome with no pain and favorable scar formation.
Discussion
We describe an uncommon long-term complication following bilateral gluteoplasty by subcutaneous injection of PAIG in an HIV negative patient of Asian descent.
The first description of PAIG as a volume replacement has been published in 2002 [6]. PAIG characteristics are the formation of a thin capsule of 0,02 mm consisting of collagen about 6 weeks after application. The commonly used Injection volumes vary between 5 to 13 ml [7, 8, 9]. PAIG has been considered an endoprosthesis due to its capsule formation and therefore isolation from the tissues surrounding the injection site. To this day only few reports concerning long term complications after PAIG injections have been published. One early publication describing a long-term abscess formation 3 years after facial PAIG injection in a healthy individual was published in 2007. Goldan, et al. described the isolation of Mycobacterium simiae in that case, an oral cavity resident, suggesting an oral infection route [10]. Campana, et al. [5] described a case of gluteal abscess formation 7 years after PAIG injection in an HIV positive individual being E. coli the infecting germ. A certain tissue susceptibility after tissue augmentation with PAIG has been suspected by other groups [3, 8, 10]. Although we were not able to find any pathogen responsible for the infection of the lower limb we highly suspect a human skin germ causing the infection. Interestingly we observed a long- term complication after 15 years in an area far away from the original PAIG injection site indicating an unusual and distant migration of the injected volume augmentation agent. It took more than a decade of free migration from the gluteal region to the left thigh of our patient. We deducted, after careful anamnesis, the migration was most likely due to the patient’s habit of receiving massages of the back and gluteal region on a regular basis indicating that PAIG might not be stable and inert enough.
Soft tissue augmentation and volume replacement are common procedures performed by plastic surgeons, oral and maxillofacial surgeons, dermatologists and others. PAIG has had a more restricted indication, i.e. the treatment of facial lipodystrophy especially in HIV positive patients. A more common treatment option for volume replacement in aesthetic augmentation is the use of injectible collagen, hyaluronic acid and especially the autologous fat transfer [11, 12, 13, 14]. Huge experience has been made over the past decades in the field of volume replacement by those injectible materials mentioned before with quite low complication rates. Therefore collagen and HA injections are a safe and practicable method in the hands of the experienced practitioner with precise predictable results, PAIG injections on the other hand can present complication rates as high as 4,8 % [15, 16].
Today’s societies are characterized by high migratory movements resulting in a different and heterogenic composition of individuals with different national and cultural backgrounds, therefore uncommon treatment techniques and methods concerning volume replacement therapies have to be considered. Especially in Asian countries different and uncommon methods for volume replacement have to be taken into account. There might be no records proving purity, quality and composition of the agents used for soft tissue augmentation. Moreover practitioners have to bear in mind that patients of the LGBTQ community are more prone to aesthetic treatments e.g. gluteal augmentation with silicone or PAIG, as we show in our report [17, 18]. Granuloma formation caused by high volume gluteal injections of silicone as shown by Seeger, et al. in another patient of Asian descent indicates a possible link between gluteal silicone injection and bilateral avascular femoral head necrosis and the formation of silicone granulomas [19]. Especially untrained practitioners will continue to perform volume augmentation with liquid injectibles that will lead to inevitable complications [20].
For the improvement of diagnostic accuracy and subsequent effective treatment it is highly important to consider infectious complications as a result of aesthetic and medical soft tissue augmentation. Correct, thorough and empathetic patient history taking might be required especially in patient with a foreign provenance and practitioners need to be sensitive in the very process of assessment.
Acknowledgment
The authors declare that they have no conflict of interest.
References
-
Narins RS, Beer K (2006) Liquid injectable silicone: a review of its history, immunology, technical considerations, complications, and potential. Plast Reconstr Surg 118(3): 77S-84S.
-
Karim RB, lint ADC, Galen SRV, Rozelaar LV, Askarizadeh PTNE, et al. (2008) Long-Term Effect of Polyalkylimide Gel Injections on Severity of Facial Lipoatrophy and Quality of Life of HIV-Positive Patients. Aesth Plast Surg 32(6): 873-878.
-
Nelson L, Stewart J (2011) Early and late complications of polyalkylimide gel (Bio-Alcamid)®. Journal of Plastic Reconstructive & Aesthetic Surgery 64(3): 401-404.
-
Karim RB, Hage JJ, Rozelaar LV, Lange CAH, Raaijmakers J (2006) Complications of polyalkylimide 4% injections (Bio-AlcamidTM): a report of 18 cases. Journal of Plastic Reconstructive & Aesthetic Surgery 59(12): 1409-1414.
-
Campana M (2010) Late-onset gluteal Escherichia coli abscess formation 7 years after soft tissue augmentation with Bio-AlcamidTM in a HIV-positive patient. Journal of Plastic Reconstructive & Aesthetic Surgery 63(9): e709-e710.
-
Pacini S, Ruggiero M, Morucci G, Cammarota N, Protopapa C, et al. (2002) Bio-alcamid: a novelty for reconstructive and cosmetic surgery. Ital J Anat Embryol 107(3): 209- 214.
-
Ramon Y, Fodor L, Ullmann Y (2007) Preliminary Experiences with Bio-Alcamid in HIV Facial Lipoatrophy. Dermatology 214(2): 151-154.
-
Lahiri A, Waters R (2007) Experience with Bio-Alcamid, a new soft tissue endoprosthesis. Journal of Plastic Reconstructive & Aesthetic Surgery 60(6): 663-667.
-
Protopapa C, Sito G, Caporale D, Cammarota N (2003) Bio‐Alcamid TM in drug‐induced lipodystrophy. Journal of Cosmetic and Laser Therapy 5(3-4): 226-230.
-
Goldan O, Georgiou I, Farber N, Winkler E, Haik J, et al. (2007) Late-onset facial abscess formation after cosmetic soft tissue augmentation with bio-alcamid. Aesthetic Surgery Journal 27(4): 416-418.
-
Jagdeo J, Ho D, Lo A, Carruthers A (2015) A systematic review of filler agents for aesthetic treatment of HIV facial lipoatrophy (FLA). Journal of the American Academy of Dermatology 73(6): 1040-1054.e14.
-
Heden P, Sellman G, Wachenfeldt MV, Olenius M, Fagrell D (2009) Body Shaping and Volume Restoration: The Role of Hyaluronic Acid. Aesth Plast Surg 33(3): 274-282.
-
Mckee D, Remington K, Swift A, Lambros V, Comstock J, et al. (2019) Effective Rejuvenation with Hyaluronic Acid Fillers: Current Advanced Concepts. Plastic and Reconstructive Surgery 143(6): 1277e-1289e.
-
Clauser L, Zavan B, Galie M, Vittorio LD, Gardin C, et al. (2019) Autologous Fat Transfer for Facial Augmentation: Surgery and Regeneration. Journal of Craniofacial Surgery 30(3): 682-685.
-
Beauvais D, Ferneini EM (2020) Complications and Litigation Associated With Injectable Facial Fillers: A Cross-Sectional Study. Journal of Oral and Maxillofacial Surgery 78(1): 133-140.
-
Schelke, Leonie W, Canninga, Marijke, Neumann, et al. (2009) Complications after Treatment with Polyalkylimide. Dermatologic Surgery 35: 1625-1628.
-
(2016) A potential role for the dermatologist in the physical transformation of transgender people: A survey of attitudes and practices within the transgender community. Journal of the American Academy of Dermatology 74(2) : 303-308.
-
Ginsberg BA (2017) Dermatologic care of the transgender patient. International Journal of Women’s Dermatology 3(1): 65-67.
-
Seeger JB, Ahmed GA, Basad E, Rickert M, Ishaque BA(2014) Gluteal silicone injections and total hip arthroplasty: a case report. J Med Case Reports 8(1): 140.
-
Ellis LZ, Cohen JL, High W (2012) Granulomatous reaction to silicone injection. J Clin Aesthet Dermatol 5(7): 44-47.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication