A Case of Cartagenet's Syndrome Presenting as a Solid Pulmonary Lesion
Background: Cartagena syndrome is a very rare disease with typical clinical manifestations of chronic sinusitis, bronchiectasis, and visceral inversion. Although it is not difficult to diagnose, many physicians do not pay enough attention to it, and it is often misdiagnosed or underdiagnosed. Here, we describe a patient with Cartagena syndrome who presented with solid pulmonary lesions on admission to the hospital. Case Details: A 15-year-old young woman with clinical symptoms such as cough, expectoration, nasal congestion, and runny nose came to the hospital this time due to the aggravation of cough and expectoration symptoms and chest pain. At admission, chest CT showed consolidation of the middle lobe of the left lung and inversion of the whole internal organs. After anti infection and expectorant treatment, the symptoms improved. Reexamination of chest CT showed that inflammation was obviously absorbed, the middle lobe bronchiectasis was obvious, and improved sinus CT showed extensive sinusitis, The final clinical diagnosis was Katane syndrome. Conclusion: It is not difficult to diagnose Cartagene syndrome with typical triad, but it is easy to miss or misdiagnose those with atypical imaging manifestations. For patients with lung consolidation and visceral inversion, we should think of the possibility of Cartagene syndrome, and timely review chest CT and improve relevant examinations to avoid missed diagnosis and misdiagnosis.
Case Presentation
Kartagener’s syndrome (KS) is a rare autosomal recessive genetic disease. In 1933, Kartagner first described the syndrome: the clinical triad of chronic sinusitis, bronchiectasis and visceral inversion. In 1975, Campner and others proposed that ciliary movement disorder is the cause of KS [1]. Normal cilia function is essential for the defense of the respiratory host and sperm vitality, and to ensure correct visceral orientation during embryogenesis. In KS, mutations in DNAI1 and DNAH5 genes will cause damage to ciliary movement, leading to recurrent sinus and lung infections, infertility, and the wrong direction of left and right viscera [2, 3]. Here we report a case of Katag sodium syndrome with pulmonary consolidation on admission.
Case Details
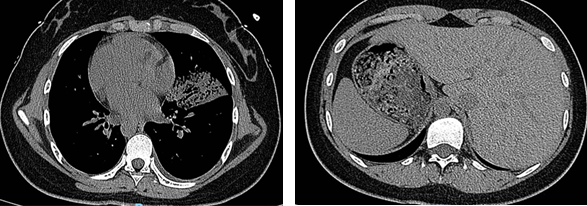
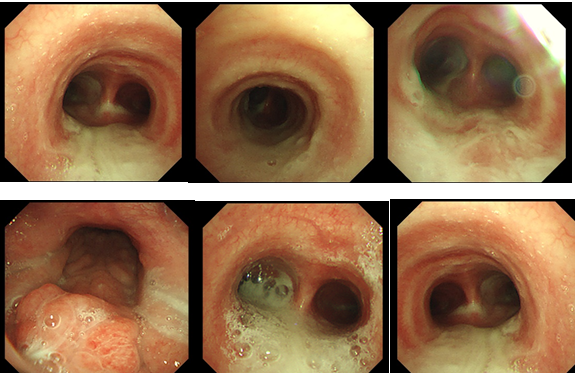
The patient is a 15-year-old young female, whose parents and sister are in good health. She complained of irregular menstrual cycle and repeated cough, expectoration, nasal congestion, runny nose and other clinical symptoms since childhood. This time, she came to the hospital for treatment due to worsening cough and expectoration symptoms with chest pain. Chest CT: total viscera inversion (Figure 1), mirror right middle lobe (left middle lobe) massive pneumonia with consolidation and atelectasis of lung tissue, Mirror right thorax (left thorax) with a small amount of pleural effusion (Figure 2). Considering lung infection, he was admitted to our department. Bronchoscopy: a large amount of yellow and white sticky sputum was trapped in the trachea, left and right main bronchi, and bronchial tubes of each lobe (Figure 3). Haemophilus influenzae was found in the alveolar lavage fluid, and cefoperazone sulbactam sodium was given to fight infection, supplemented by expectorant, physical therapy, and other treatments. After more than 10 days, the patient’s symptoms were significantly relieved. CT reexamination of the chest showed that the whole viscera were transposed, and the mirror right middle lung lobe (left middle lung lobe) was inflamed with bronchiectasis. Compared with the bronchiectasis of CT on admission, the inflammation was obviously absorbed in Figure 4. Perfect CT of nasal sinuses: chronic inflammation of bilateral maxillary sinuses, ethmoid sinuses, and sphenoid sinuses, and the final clinical diagnosis is Kattagne syndrome (KS).


Discussion
KS is a very rare autosomal recessive genetic disease. The typical clinical trial of KS is chronic sinusitis, bronchiectasis and internal inversion, with an incidence of about one in 60000 [4]. It is a special type of primary ciliary dyskinesia (PCD). The pathological manifestations are abnormal ciliary structure, dyskinesia and clearance dysfunction, which lead to the secretion and pathogenic microorganisms cannot be discharged timely and effectively, and eventually develop into bronchiectasis, sinusitis, nasal polyps and otitis media. The lack of ciliary movement also affects the development of the embryo, leading to the disorder of organ differentiation in the human body, which is typically manifested as visceral heterotopia. And because of the cilia dyskinesia, sperm motility can lead to infertility. At present, the diagnostic criteria of KS are:
- Dextrocardium or total visceral transposition
- Bronchiectasis
- Paranasal sinusitis. Complete KS can be diagnosed with the above three items at the same time, and only the first two items are diagnosed as incomplete KS.
Because KS is a congenital disease, there is no specific treatment method at present, mainly to enhance the immunity of the body, pay attention to the prevention and control of infection, and prevent the further development of the disease. Acute infection period: infection should be actively controlled. Sensitive antibiotics can be selected for treatment after the pathogenic bacteria are identified according to the sputum culture results of patients. Surgical treatment is required when conventional conservative treatment is ineffective, especially when bacteria are resistant to drugs or severe nasal polyps. Non acute infection period: strengthen exercise, improve immunity, prevent colds, and prevent acute exacerbation of infection. At present, some studies have introduced viral gene fragments carrying normal DNAl1 gene into cells with ciliary function defects due to mutation of DNAI1 gene, so that cilia can resume normal rhythmic movement [5]. However, at present, gene therapy has not been widely carried out in clinical work, which needs further clinical research.
Although KS is a rare disease, its clinical diagnosis is not difficult. A clear diagnosis can be made by asking about the medical history, physical examination and related imaging data. This patient has triple symptoms of bronchiectasis, visceral transposition and sinusitis, and the diagnosis of complete KS is clear. The patient began to show symptoms of respiratory tract infection and sinusitis repeatedly when he was young, but failed to be diagnosed as KS, which may be related to the clinicians’ failure to fully understand and pay attention to KS. In addition, the imaging manifestations of the patient at the time of admission were pulmonary consolidation signs and bronchiectasis was covered up, which increased the difficulty of diagnosis. With the progress of treatment, consolidation is absorbed, and bronchiectasis is manifested, and the final diagnosis is clear. At present, the bronchiectasis of the patient is only limited to the middle lobe, but the bronchoscope first shows a large number of thick sputum in each lobe segment of both lungs. Considering that the ciliary telecontrol disorder of the patient is mainly in the middle lobe at present, but other lung segments are also getting worse, it is very likely that extensive bronchiectasis of both lungs will occur in the near future.
Conclusion
We reported a case of Cartagene syndrome with lung consolidation at admission. For patients with lung consolidation and organ inversion, we should think about the possibility of KS. After treatment, we should actively review chest imaging, and if necessary, improve CT scanning of nasal sinuses, bronchoscopy, maxillary sinus puncture and other examinations to determine whether there is bronchiectasis and paranasal sinusitis, so as to improve the diagnostic rate of clinical KS, Find and treat as early as possible.
References
-
Tadesse A, Alemu H, Silamsaw M, Gebrewold Y (2018) Kartagener’s syndrome: a case report. J Med Case Rep 12(1): 5.
-
Chilvers MA, Rutman A, Callaghan OC (2003) Ciliary beat pattern is associated with specific ultrastructural defects in primary ciliary dyskinesia. J Allergy Clin Immunol 112(3): 518-524.
-
Lobo LJ, Zariwala MA, Noone PG (2011) Ciliary dyskinesia: primary ciliary dyskinesia in adults. Eur Respir Mon 52: 130-149.
-
Pandit S, Choudhury S, Das A, Basuthakur S, Das SK (2014) A rare case of Kartagener’s syndrome. J Nat Sci Biol Med 5(1): 175-177.
-
Chhin B, Negre D, Merrot O, Pham J, Tourneur Y, et al. (2009) Ciliary beating recovery in deficient human airway epithelial cells after lentivirus ex vivo gene therapy. PLoS Genet 5(3): e1000422.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report