Excellent Short-term Results of Articular Surface Replacement XL Total Hip Arthroplasty
Symptoms of pain, loosening and squeaking were historically reported as the main revision reasons for articular surface replacement XL (ASR XL) total hip arthroplasty. A total of 42 cementless primary total hip arthroplasties using ultra large-diameter femoral head and mono block acetabular component were performed in our institution. These consecutive 42 arthroplasties were retrospectively reviewed and the results were recorded and analysed. After an average 3-year follow-up period (range, 2.5-3.6 years), 42 primary replacements in 39 patients could be reviewed fully. Mean age at surgery was 51.9 years (range, 20-92 years). Pain was noted in 4 hips and squeaking was noted in 1 hip. According to Harris rating system, clinical results were graded excellent and good in 93% of hips and fair in 7%. Radiologically, the cup abduction angle of the acetabular components for all symptomatic hips was in acceptable realm. There has been no osteolysis or asceptic loosening on both sides of the hip. The failure rate of ASR XL total hip arthroplasty was 2% at early follow-up. The controversial ASR XL acetabular component could yield excellent clinical results in some circumstances.
Introduction
After going through the clinical practice of first- generation and second-generation metal-on-metal articulations in total hip arthroplasty, people began to observe the advantages of large diameter metal-on-metal bearing surface. Large diameter metal-on-metal articulations could offer improved stability and increased range of motion compared with smaller diameter bearings [1, 2]. Meanwhile, with improved metallurgy and new manufacturing quality control, metal-on-metal implants were thought to be able to reduce bearing wear and to achieve better long-term results than conventional implants. These proposed advantages together have prompted the use and development of large diameter metal-on-metal articulations worldwide.
The ASR XL (DePuy Orthopaedics, Warsaw, Indiana) hip prosthesis was released in worldwide for use in conventional total hip arthroplasty in 2003. This total hip system made it possible to have a mono block metal-on- metal ace tabular component paired with a large diameter femoral head, allowing for greater range of motion and bone conservation. However, as a result of many complaints and higher revision rate than other bearing surfaces after use of ASR XL hip prostheses, the ASR XL Acetabular System as well as the ASR Hip Re- surfacing System were voluntarily recalled worldwide by the manufacturer in August 2010.One of the reasons responsible for the recall was the higher short-term to mid-term failure rate reported in some literature [3, 4, 5]. Out of concerns about the total hip arthroplasties using ASR XL Ace tabular System performed during early time in our institution, a retrospective survey has been devised to determine the clinical and radio graphical outcomes for the ASR XL total hip arthroplasty.
Materials and Methods
Between April 2009 and June 2010, 42 cases (39 hips) of primary total hip arthroplasties with the DePuy ASR XL implant were performed at a tertiary care medical center by the senior author (Sun). Porous-coated cobalt-chrome DePuy ASR acetabular components were used in all hips, paired with the modular ultra large-diameter cobalt- chrome femoral heads. The range of ace tabular cup diameter was 44-56mm and the range of femoral head diameter was 39-49mm. Modular titanium DePuy SROM stems were implanted for all patients. The outcome variable was success or failure. Failure was defined as the need for revision. Table 1 gives the details of the patients enrolled in this study. Their mean age at surgery was 51.9 years (range, 20-92years), and the mean body mass index (BMI) was 23.9(range, 17.3-32.1). All the operations were performed with a modified Harding approach to minimize the incidence of posterior dislocation. When fixing the acetabular cup, under reaming press-fit technique was used.
| Men | Women | P | |
| Patients | 19 | 20 | |
| Unilateral | 17 | 19 | |
| Bilateral | 2 | 1 | |
| Average age(y) | 49.8±15.7 | 54.8±11.3 | 0.313 |
| Average weight(kg) | 70.8±9.5 | 59.2±8.8 | 0 |
| Average body mass index(kg/m2) | 24.6±3.0 | 23.2±2.8 | 0.141 |
| Diagnosis(hips) | |||
| Osteonecrosis | |||
| Hip dysplasia | 10 | 4 | |
| Primary osteoarthritis | 1 | 13 | |
| AS* | 4 | 4 | |
| Post-traumatic OFFN* | 4 | 0 | |
| 1 | 0 | ||
| 1 | 0 |
Table 1: Details of the 39 patients (42hips).
Postoperative follow-up of all the 39 patients was undertaken at two, six and twelve months and then annually. During the follow-up, we have managed to obtain the information of all the patients in any possible approach and 8 patients (8 hips) were contacted by phone or mail. Clinical results were graded according to the Harris scoring system. In light of the complications mentioned in former literature [4, 5], incidence of groin pain, grinding, squeaking, dislocation and revision was particularly observed at each visit. A complete radiograph file was set for each patient and a single surgeon independent of the operation was assigned to make all radiographic measurements and assessments. According to the method by Callaghan [6], cup abduction was measured on a standard AP pelvis radiograph. Fixation and osteolysis were assessed using the method by DeLee and Charnley [7]. Descriptive statistics were performed using the SPSS Software (Version 19). Independent t tests were used to assess differences in normally distributed continuous variables, and statistical significance was set at P < .05.
Results
There were no revisions performed until the final follow-up. The average Harris score improved from preoperative 47.8 (range, 28.0-69.5) to 91.6 (range, 73.0 - 98.0) (P<0.05). In addition, the mean Harris score for the male patients and female patients was 93.0 and 90.2 respectively, which did not have statistical difference (P=0.101). There were zero cases of osteolysis and zero cases of dislocation. Under the witness of surgeon independent of the operation, the mean abduction angle of all the acetabular cups was 38.7° (range, 32.0°-44.0°) and no differences were noted between the initial and the final measurement. Statistics of the results was shown (Table 2).
| Men(19 patients,21 hips) | Women(20 patients,21 hips) | P | |
|---|---|---|---|
| Mean abduction | 40.0±2.5 | 39.7±3.9 | 0.834 |
| Mean Harris Score | 93.0±5.3 | 90.2±5.4 | 0.101 |
| Complications | 3 pain | 1 pain,1 squeaking | - |
Table 2: Statistics of the results.
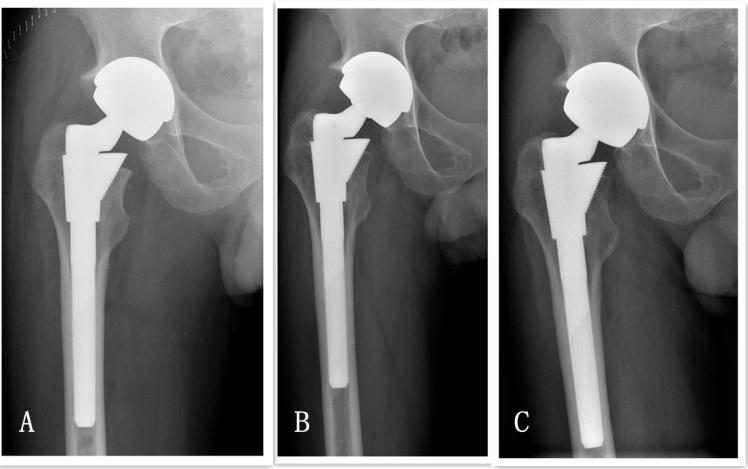
Table 2: Statistics of the results. P values are in 2-tailed t test comparison between the men group and women group. In total, there were 5 cases demonstrating hip dysfunction. Mean abduction and Harris score for this symptomatic subgroup were 36.8° and 84.2. Hip pain occurred in 4 patients (4 hips). One male patient had persistent pain after operation and needed NSAIDs to relieve the pain which greatly affected his daily life. However, there were no signs of loosening on the radiograph and no symptoms of infection (Figure 1). The cup abduction of this hip measured 36°.Though reoperation being vigorously advised, the patient finally refused the revision. The other three patients, one male and two female, noted light pain intermittently 1 year after operation. However, the pain had little influence on their daily life and they were satisfied with the current hip function. The abduction of these three hips measured 36°, 40°and 40° respectively. There was one additional female patient (1 hip) noting the squeaking and the abduction measured 32°. The Harris score for this patient was 91 at final visit and she felt no need to be given any treatment. Thus, we concluded the early failure rate in this cohort was 2% (1/42).
No statistical difference in cup abduction and BMI was found between the symptomatic hips and the asymptomatic hips. In addition, we compared the data in this study with the data available in former literature about ASR XL total hip arthroplasty [5] by using 2-tailed Student t test. Table shows the details of the comparison.
| Men(21 hips) | Men(39 hips)* | p | Women(21 hips) | Women(31 hips)* | P | |
|---|---|---|---|---|---|---|
| Age | 49.8±15.7 | 55.8±12.2 | 0.1062 | 54.8±11.3 | 63.7±12.5 | 0.0117 |
| BMI | 24.6±3.0 | 28.2±5.1 | 0.0044 | 23.2±2.8 | 27.0±6.1 | 0.0041 |
Table 3: The details of the comparison.
Discussion
Since the introduction of first generation of metal-on- metal bearings made of stainless steel by Wiles [8], the complications caused by metal debris such as metal ion release, osteolysis, pseudo tumor formation and hypersensitivity have always been the persistent concerns. Several times of evolution of metal-on-metal bearing surface made it clear that improved metallurgy and manufacturing control were the primary ways to reduce wear debris. Based on this concept, some studies about metal-on-metal hip replacement have yielded excellent results after long term follow-up [9, 10]. Meantime, the importance of implant design was also noted. In vivo and in vitro studies [11, 12] both have demonstrated that large diameter metal-on-metal bearing surface could effectively reduce wearing rate. In addition, large femoral heads had fewer incidence s of dislocation than small femoral heads [1, 2]. In high expectation to increase the range of motion of the hip joint and to reduce the wearing rate and dislocation, ASR XL system was introduced. However, in contrary to the advantages initially expected, adverse effects began to be reported [3, 4, 5] after years of clinical use in hip replacement. The reasons leading to high failure rate were mostly attributed by the authors to the primordial design flaws of the ASR XL system. We began to use the ASR XL system in total hip arthroplasty from April 2009.After an average 3-year follow-up, the failure rate in this cohort was estimated 2%, better than the results reported in other corresponding literature [4, 5, 13]. To validate the result, some defects obviously existing in our study were listed as follows. First, one of the main reasons leading to ASR hip revision was the metal debris correlated with asceptic loosening [13] and per prosthetic osteolysis in some cases could not be detected simply by radio graphical assessment [14]. Nevertheless, we didn’t take serum Cr and Co level test at each visit. Thus, the final result that no osteolysis or asceptic loosening occurred in this cohort through radio graphical assessment may have some error in it. Second, 8 patients could not be reviewed fully by clinic route; phone and mail became the only ways to obtain the complete information of these patients. Based on this consideration, the mean Harris score 91.6 at the final follow-up may deviate from the real level slightly. Third, in comparison with the data from the large artificial joint replacement registry centers [3, 13], the scale of samples enrolled in this study was smaller. However, it is of great significance to record the early term results of a group of Asian patients after using ASR XL hip system. Aiming to clarify the reasons leading to the excellent result in this study, several factors influencing the treatment effect, such as abduction of the metal cup, body mass index of the patients and the sex difference, were analyzed. In terms of cup angle, simulator studies have indicated an increase wear and metal ion levels with steeper cup angle (>50°) [15, 16]. De Haan [17] proposed that, to optimize the wear characteristics of a metal-on-metal implant, a function articular surface of 10mm at least was necessary. Owing to the sub hemispheric design employed by ASR XL cup, a 48-mm ASR XL implant inserted at 45° of abduction functions like an implant placed at 59° of abduction, subsequently leading to edge loading, diminished lubrication and metallosis. In our series, the mean abduction measured 38.7° (range, 32.0°- 44.0°),which was smaller than Steele’41°(range,31°-57°) [4] and Langton’ 48.8° (range,36° - 76°) [13]. Lower position of metal cups by the surgeon effectively prevented edge loading, decreasing the incidence of metalloids. In one-leg standing position, the pressure the hip joint has to bear is three times bigger than the body weight. In running and jumping, the ratio could reach up to 10 or more. Thus, it is undoubted that overweight will accelerate the wear rate of the bearing surface. In this study, body weight and BMI were recorded and calculated for each patient. The mean BMI of these patients was 23.9 (range, 17.3-32.1), which was statistically smaller (p<0.05) than that of corresponding literature [5]. Relatively lighter weight of Asian patients is helpful in avoiding acute abrasion and extending the duration of the metal-on-metal articulation. A large number of literatures [18, 19, 20] have emphasized the effect of sex factor on the clinical result and cautioned that prudence should be taken before the application of metal-on-metal implant to female patients. In this study, all the patients were also divided into male group and female group. However, there was no definite difference in function results between these two groups. The only patient who we thought needed revision appeared in the male group. In terms of this sharp contrast, we didn’t make conclusion that there would never be differences between them. It is thought that long term follow-up is needed and the plan is in progress. In summary, total hip arthroplasty using ASR XL system yield excellent clinical result than we initially expected after short term follow-up. The complications caused by this kind of cup design did not occur in our series in great number. However, we report this experience without explaining it fully. We hope that others will be able to confirm or refute the outcome we report and, if the former, explain it.
References
-
Cuckler JM, Moore KD, Lombardi Jr AV, McPherson E, Emerson R (2004) Large versus small femoral heads in metal-on-metal total hip arthroplasty. J Arthroplasty 19(8): 41-44.
-
Smith TM, Berend KR, Lombardi Jr AV, Emerson RH Jr, Mallory TH (2005) Metal-on-metal total hip arthroplasty with large heads may prevent early dislocation. Clin Orthop Relat Res 441: 137-142.
-
de Steiger RN, Hang JR, Miller LN, Graves SE, Davidson DC (2011) Five-year results of the ASR XL Acetabular System and the ASR Hip Resurfacing System: an analysis from the Australian Orthopaedic Association National Joint Replacement Registry J Bone Joint Surg Am 93(24): 2287-2293.
-
Steele GD, Fehring TK, Odum SM, Dennos AC, Nadaud MC (2011) Early failure of articular surface replacement XL total hip arthroplasty. J Arthroplasty 26(6): 14-18.
-
Bernthal NM, Celestre PC, Stavrakis AI, Ludington JC, Oakes DA (2012) Disappointing Short-Term Results With the DePuy ASR XL Metal-on-Metal Total Hip Arthroplasty. J Arthroplasty 27(4): 539-544.
-
Callaghan JJ, Salvati EA, Pellicci PM, Wilson PD, Ranawat CS (1985) Results of revision for mechanical failure after cemented total hip replacement, 1979 to 1982. A two to five-year follow-up. J Bone Joint Surg Am 67(7): 1074-1085.
-
DeLee JG, Charnley J (1976) Radiological demarcation of cemented sockets in total hip replacements. Clin Orthop Relat Res 121: 20-32.
-
Wiles P (1958) The surgery of the osteoarthritic hip. Br J Surg 45(193): 488-497.
-
Randelli F, Banci L, D'Anna A, Visentin O, Randelli G (2012) Cementless Metasul metal-on-metal total hip arthroplasties at 13 Years. J Arthroplasty 27(2): 186- 192.
-
Dastane M, Wan Z, Deshmane P, Long W, Dorr L (2011) Primary hip arthroplasty with 28-mm Metasul articulation. J Arthroplasty 26(4): 662-664.
-
Affatato S, Leardini W, Jedenmalm A, Ruggeri O, Toni A (2007) Larger diameter bearings reduce wear in metal-on-metal hip implants. Clin Orthop Relat Res 456: 153-158.
-
McKellop H, Park SH, Chisea R, Doorn P, Lu B, et al. (1996) In vivo wear of 3 types of metal on metal hip prostheses during 2 decades of use. Clin Orthop Relat Res 329S: S128-S140.
-
Langton DJ, Jameson SS, Joyce TJ, Hallab NJ, Natu S, et al. (2010) Early failure of metal-on-metal bearings in hip resurfacing and large-diameter total hip replacement. J Bone Joint Surg Br 92(1): 38-46.
-
Randelli F, Banci L, Favilla S, Daniela Maglione, Alberto Aliprandi, et al. (2013) Radiographically Undetectable Periprosthetic Osteolysis With ASR Implants: The Implication of Blood Metal Ions. J Arthroplasty 28(8): 1259-1264.
-
Brondner W, Grubl A, Jankovsky R, Meisinger V, Lehr S, et al. (2004) Cup inclination and serum concentration of cobalt and chromium after metal-on- metal total hip arthroplasty. J Arthroplasty 19(8): 66- 70.
-
Angadji A, Royle M, Collins SN (2008) A hip simulator study on the effect of cup inclination on the wear of ‘‘as cast’’ and ‘‘double heat-treated’’ metal-on-metal hip replacements, 54th Ann Meet of Orthop Res Soc p.1912.
-
De Haan R, Campbell PA, Su EP, De Smet KA (2008) Revision of metal- on-metal resurfacing arthroplasty of the hip: the influence of malpositioning of the components. J Bone Joint Surg Br 90(9): 1158-1163.
-
Latteier MJ, Berend KR, Lombardi AV, Ajluni AF, Seng BE, et al. (2011) Gender is a Significant Factor for Failure of Metal-on-Metal Total Hip Arthroplasty. J Arthroplasty 26(6): 19-23.
-
Jameson SS, Baker PN, Mason J, Porter ML, Deehan DJ, et al. (2012) Independent predictors of revision following metal-on-metal hip resurfacing. J Bone Joint Surg Br 94(6): 764-754.
-
Murray DW, Grammatopoulos G, Pandit H, Gundle R, Gill HS, et al. (2012) The ten-year survival of the Birmingham hip resurfacing: an independent series. J Bone Joint Surg Br 94(9): 1180-1186.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results