Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
Postoperative pelvic collections of lymphatic origin are uncommon complications following acetabular fracture fixation. We report a 71-year-old man who developed a large anterior extraperitoneal pelvic collection after open reduction and internal fixation of a right both-column acetabular fracture using the modified Stoppa approach. Comprehensive biochemical analysis and lymphoscintigraphy confirmed a lymphatic origin as the underlying cause of the pelvic collection and excluded alternative etiologies including urinoma, chylous leak, pancreatic leak, bile leak, infection, and malignancy. Persistent high-output drainage ranging between 200-600 mL per/day continued despite two sessions of intranodal lymphangiography with glue embolization. Chemical sclerotherapy using tigecycline diluted in normal saline was subsequently attempted but did not reduce drainage output. The patient later developed secondary infection, which was successfully treated with targeted antibiotic therapy. With prolonged controlled drainage and multidisciplinary management, the lymphatic fistula eventually resolved during outpatient follow-up. At one-year follow-up, radiographs demonstrated complete fracture union, and the patient returned to his preinjury functional status without recurrence. This case highlights a rare complication of the modified Stoppa approach and demonstrates that delayed spontaneous resolution may occur even after failure of interventional therapies. Clinical Message: Persistent postoperative pelvic collections should prompt evaluation for lymphatic injury. Even when interventional treatments fail, prolonged controlled drainage may result in spontaneous resolution, avoiding unnecessary repeated procedures.
Hakeem N¹*, Almuashi I¹, Alghamdi A¹, Almonaye H¹, Elsayed A¹ and Alassiri I²
¹Department of Orthopedic Surgery, King Fahad Armed Forces Hospital, Ministry of Defense Health Services, Saudi Arabia ²Department of Interventional Radiology, King Fahad Armed Forces Hospital, Ministry of Defense Health Services, Saudi Arabia repeated procedures.
Introduction
The modified Stoppa intrapelvic approach has gained widespread acceptance for the fixation of anterior column and both-column acetabular fractures because it provides improved visualization of the quadrilateral surface and pelvic brim while limiting extensive soft-tissue dissection [1, 2]. However, this approach involves dissection in proximity to lymphatic-rich regions adjacent to the external iliac vessels and the obturator neurovascular bundle, creating the potential for lymphatic injury.
Postoperative pelvic collections, including lymphocele, are recognized complications in vascular, urological, and gynecological procedures but are rarely reported following acetabular fracture fixation [3]. Clinically significant lymphatic collections may result in pelvic compression symptoms, persistent drainage, secondary infection, prolonged hospitalization, and delayed recovery. To our knowledge, reports describing lymphatic pelvic collections following acetabular fracture fixation via the modified Stoppa approach remain extremely limited in the orthopedic trauma literature. We present a case of a large refractory pelvic collection that developed after fixation of a both- column acetabular fracture and ultimately resolved following prolonged drainage and multidisciplinary management.
Case Presentation
A 71-year-old man with a history of diabetes mellitus and hypertension sustained an isolated right both-column acetabular fracture after a fall from height (Figure 1A-C).
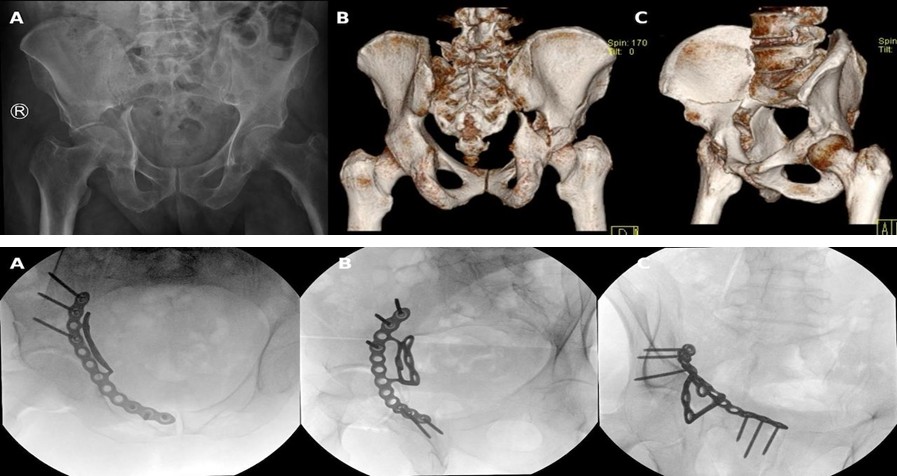
Figure 1A-C: Preoperative imaging. (A) Pelvic radiograph showing acetabular fracture. (B,C) Computed tomography scans demonstrating fracture configuration.
Open reduction and internal fixation were performed three days after injury via the modified Stoppa approach using a suprapectineal plate (Figure 2A-C).
Figure 2A-C: Postoperative radiograph showing internal fixation with satisfactory alignment.
No drain was placed at the index procedure. The immediate postoperative course was uneventful, and the patient was discharged on postoperative day three. Two weeks later, the patient presented with progressive suprapubic swelling and abdominal discomfort without systemic symptoms. Computed tomography imaging demonstrated a large multiloculated anterior extraperitoneal pelvic collection measuring approximately 1492 mL, with compression of the urinary bladder (Figure 3).

Surgical evacuation yielded clear yellow fluid. Comprehensive biochemical analysis of the drained fluid was performed (Table 1). Persistent sterile drainage ranging between 200-600 mL per/day continued for one month (Figure 4).
| Parameter | Results | Interpretation |
|---|---|---|
| Appearance | Clear yellow fluid | Consistent with lymphatic-type fluid |
| Triglycerides | <50 mg/dl | Excludes chylous leak |
| Creatinine | Equal to serum level | Excludes urinoma |
| Amylase | Within normal range | Excludes pancreatic leak |
| Bilirubin | Within normal range | Excludes biliary leak |
| Culture | Initially sterile | No early evidence of infection |
| Cytology | Negative | No evidence of malignancy |
Table 1: Biochemical Analysis of Drained Pelvic Fluid and Diagnostic Interpretation.
Lymphoscintigraphy confirmed that the pelvic collection was a lymphocele (Figure 5).
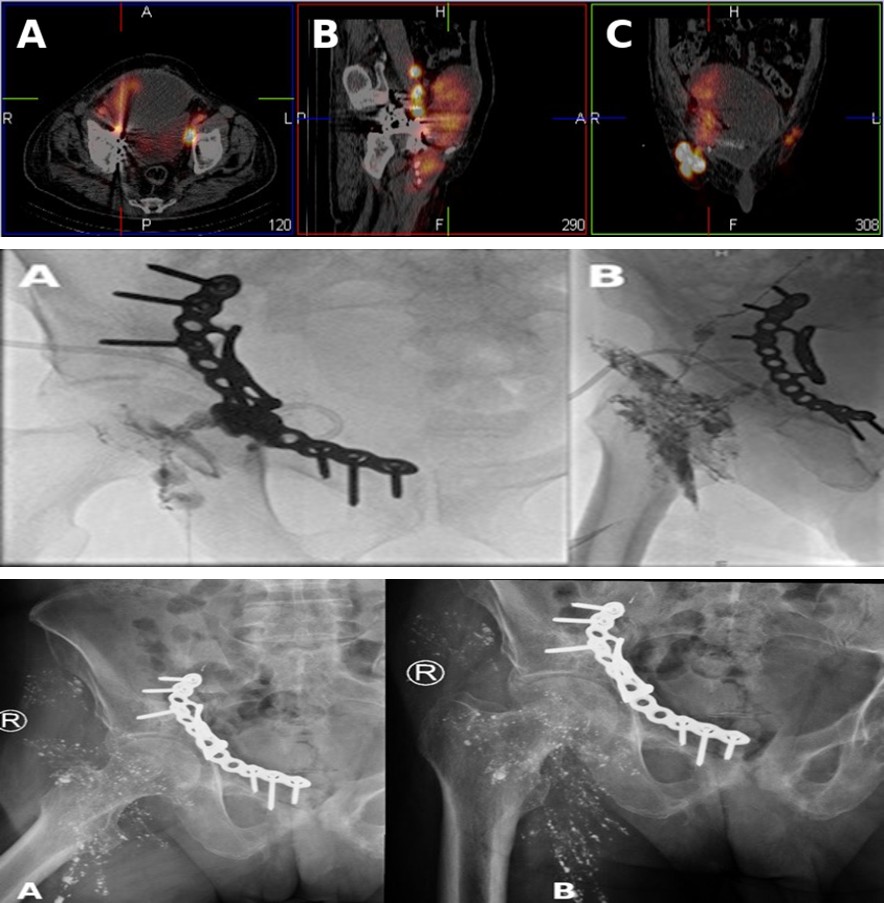
Figure 5A-C: Lymphoscintigraphy demonstrating radiotracer accumulation within the pelvic region consistent with lymphatic leakage in axial (A), sagittal (B), and coronal (C) views.
Two sessions of intranodal lymphangiography demonstrated contrast extravasation at the acetabular level, and N-butyl cyanoacrylate glue embolization was performed (Figure 6A & B).
Figure 6A-B: Glue embolization procedure. (A) First session. (B) Second session.
Despite technically successful embolization confirmed fluoroscopically, drainage output remained between 300-500 mL per/day without significant reduction over subsequent weeks [4, 5]. Chemical sclerotherapy using 50 mg of tigecycline diluted in 100 mL of normal saline was subsequently attempted but did not decrease daily drainage output.
Following prolonged drainage, the patient developed fever of 38.2 C, leukocytosis, and elevated inflammatory markers. Drain fluid culture grew Pseudomonas aeruginosa. Targeted intravenous antibiotic therapy resulted in resolution of systemic infection. No radiographic evidence of hardware involvement was identified.
After approximately two months of hospitalization, the patient was discharged with the drain in place. During outpatient follow-up, drainage gradually decreased and ultimately ceased over the following two months. Follow-up ultrasound demonstrated complete resolution of the pelvic collection, and the drain was removed without recurrence. At one-year follow-up, radiographs demonstrated complete fracture union (Figure 7A & B).
The patient returned to his pre-injury functional status with full weight bearing. No recurrence was observed. Discussion The pelvic lymphatic system accompanies major vascular structures, including the external iliac and obturator vessels, and is susceptible to injury during intrapelvic surgical dissection. The modified Stoppa approach, although less invasive than traditional extensile approaches, requires exposure of these regions and may inadvertently disrupt small lymphatic channels.
Lymphocele formation following orthopedic procedures is rare but can occur when lymphatic disruption leads to persistent leakage into confined anatomical spaces. In contrast to postoperative seromas or hematomas, lymphatic collections may demonstrate sustained high-output drainage and delayed spontaneous resolution.
Lymphoscintigraphy remains a valuable diagnostic modality for confirming lymphatic origin and identifying leakage pathways. In addition, intranodal lymphangiography not only facilitates visualization of lymphatic anatomy but also allows for targeted therapeutic intervention through embolization techniques.
In the present case, two sessions of intranodal lymphangiography with glue embolization were performed, demonstrating clear contrast extravasation at the acetabular level. Despite technically successful embolization, high- output drainage persisted. This phenomenon can be explained by the extensive collateral pelvic lymphatic network, which may maintain lymphatic flow even after occlusion of the primary leakage site.
Chemical sclerotherapy using tigecycline was also unsuccessful in reducing drainage. Failure of interventional treatment modalities in lymphatic leaks has been reported and may be influenced by factors such as multiple leakage channels, high lymphatic flow rates, and complex lymphatic anatomy. Prolonged drainage increases the risk of secondary infection, particularly in elderly patients with comorbid conditions. In this case, infection with Pseudomonas aeruginosa developed but was successfully managed with targeted antibiotic therapy without involvement of the fixation hardware.
Importantly, despite failure of both embolization and sclerotherapy, gradual spontaneous closure of the lymphatic fistula was achieved with continued controlled drainage and close multidisciplinary follow-up. This highlights a critical clinical consideration: in stable patients without uncontrolled infection, conservative management may ultimately lead to resolution even after unsuccessful interventional procedures.
This case emphasizes that persistent pelvic lymphatic collections following acetabular fracture fixation may follow a prolonged but self-limiting course. Recognition of this possibility can help guide management decisions and avoid unnecessary repeated interventions.
Conclusion
Refractory persistent pelvic collection due to lymphocele is a rare complication following acetabular fracture fixation via the modified Stoppa approach. Comprehensive biochemical evaluation and lymphoscintigraphy are essential for diagnosis. Even after failure of interventional therapies such as lymphangiographic embolization and sclerotherapy, delayed spontaneous resolution may occur with controlled drainage and multidisciplinary care.
Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given consent for clinical information and images to be reported in the journal. The patient understands that names and initials will not be published, and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Conflict of Interest
The authors declare no conflict of interest.
Funding
No funding was received for this study.
References
-
Cole JD, Bolhofner BR (1994) Acetabular fracture fixation via a modified Stoppa limited intrapelvic approach. Clin Orthop Relat Res 305: 112-123.
-
Sagi HC, Afsari A, Dziadosz D (2010) The intrapelvic approach to the acetabulum. J Orthop Trauma 24(5): 263-270.
-
Browse NL, Allen DR, Wilson NM (1997) Management of lymphoceles. Br J Surg 84(9): 1137-1143.
-
Itkin M, Nadolski GJ (2018) Modern techniques of lymphangiography and lymphatic interventions. J Vasc Interv Radiol 29(5): 623-634.
-
Nadolski GJ, Itkin M (2020) Lymphatic embolization for lymphatic leaks. Semin Intervent Radiol 37(1): 53-63.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results
- Management of Complications from Traditional Treatment of Locomotor System Injuries at the National Hospital of Niamey: A Report of 220 Cases