Subtalar Dislocation: About a Case Report
External subtalar dislocation is a rare and severe orthopedic injury, accounting for only 1% of all dislocations and 17% of subtalar dislocations. It results from forced eversion trauma and requires early diagnosis and management to prevent complications. We report a rare case of left external subtalar dislocation successfully managed in our department.
Introduction
Pure external subtalar dislocation is defined as a total and permanent loss of contact between the talus and the navicular and between the talus and the calcaneus which moves externally.
It is a rare and serious entity, representing only 1% of all dislocations observed in trauma [1]. The external variant is exceptional, representing 17% of these dislocations.
Subtalar dislocation is most often secondary to a high- energy mechanism [2] , such as road accidents or a fall, but can also occur following a sports accident [3].
In Niger, rare clinical cases or articles have been made on this subject. It is with this in mind that we report the case of a purely traumatic left external subtalar dislocation occurring in a 63-year-old patient following a road traffic accident treated in our department at the Niamey National Hospital.
This was a 63-year-old patient from Tahoua (Niger), retired, who was allegedly the victim of a road traffic accident following a skid of their public transport vehicle with an imprecise mechanism causing him pain in his left foot and absolute functional impotence of the left pelvic limb.
Upon Admission: Patient was conscious with good hemodynamic and ventilatory status.
Examination of the Locomotor System of the Left Pelvic Limb Found: Left foot deformity: His heel was displaced laterally relative to his leg with his foot in eversion and plantar flexion (Figure 1);

The head of the talus was visible and palpable on the dorsomedial aspect of his ankle (Figure 1) ; The skin was stretched at the level of the talar protrusion without visible wound (Figure 1) ; The peripheral pedal and posterior tibial pulses were clearly felt; Sensitivity and motor function of the foot were preserved; Active or passive mobilization of the foot was impossible;
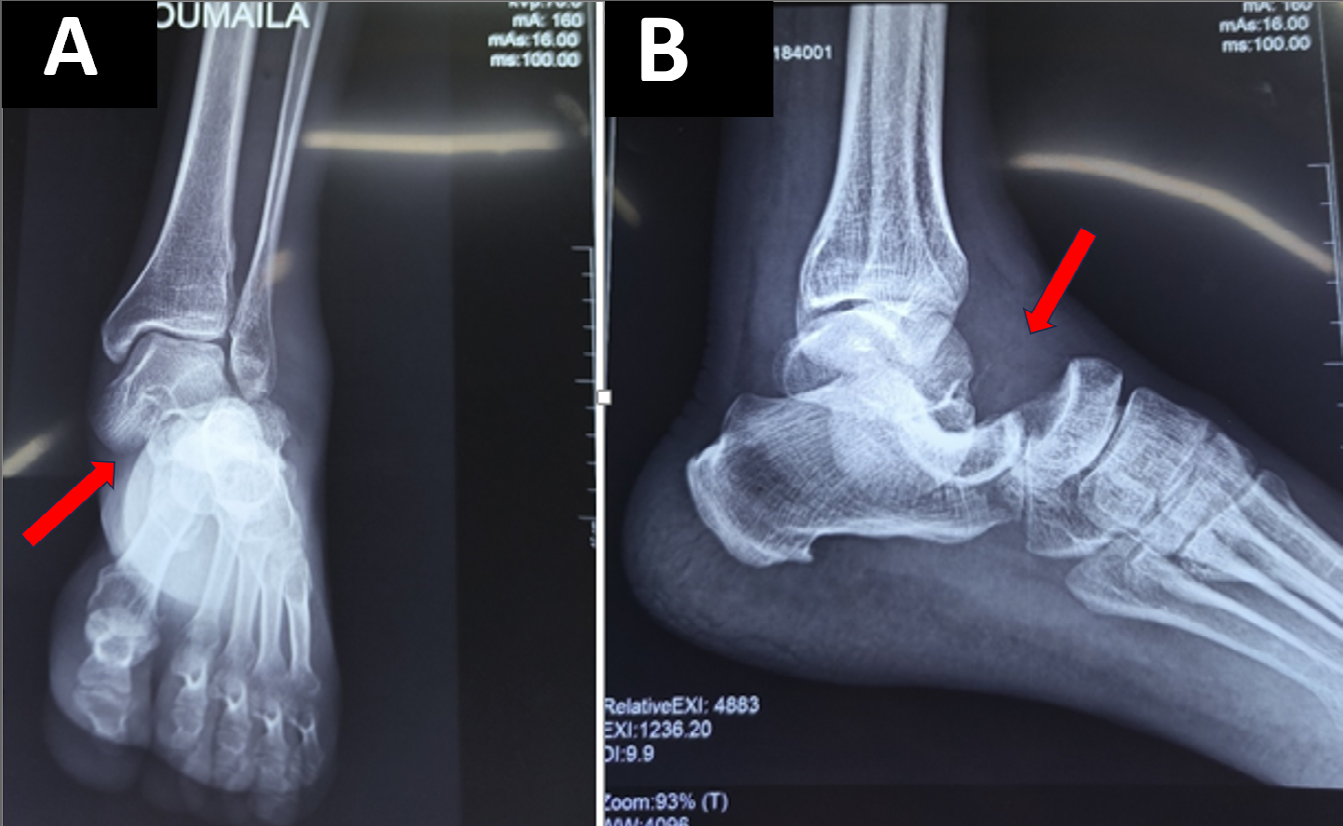
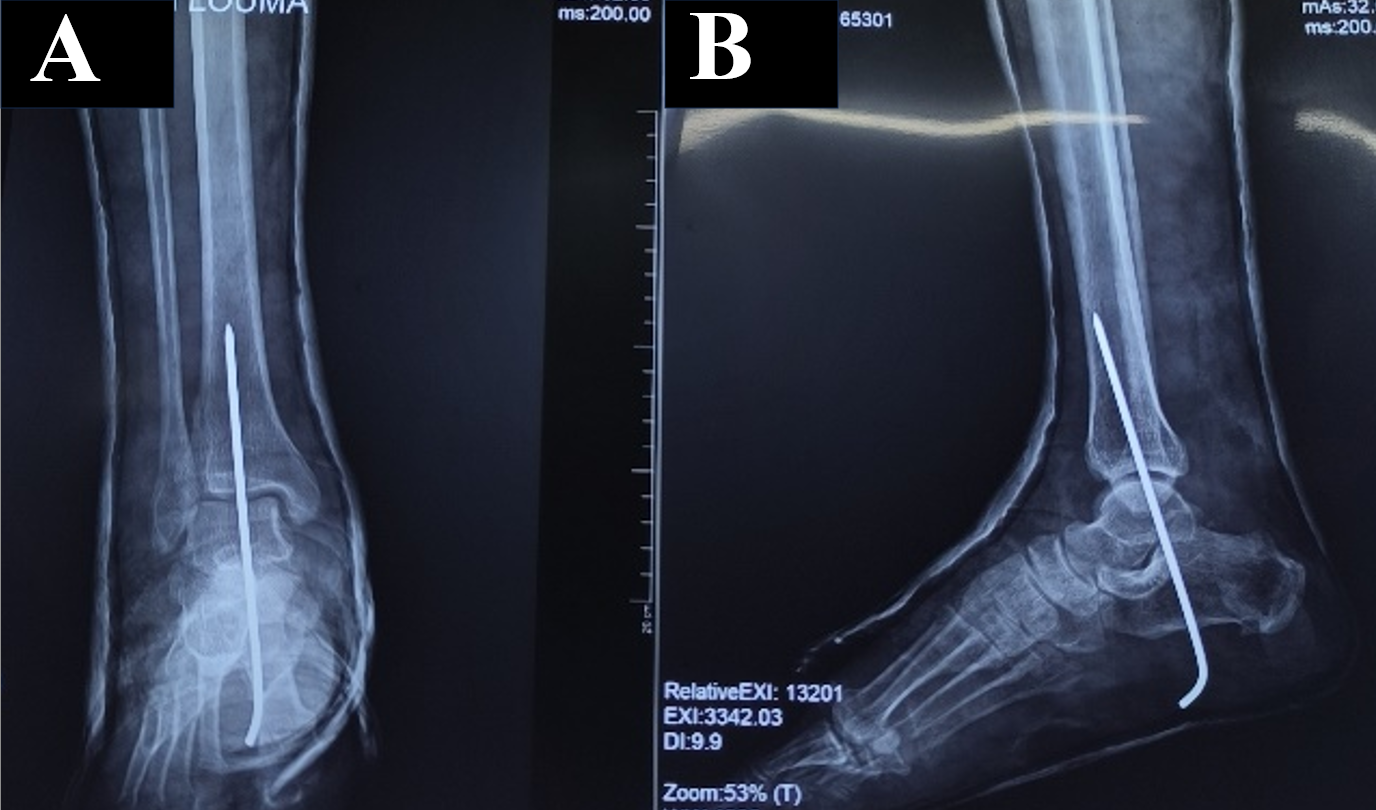
The radiological assessment showed a pure left external talocalcaneal and talo-navicular dislocation without associated fracture (Figure 2). The orthopedic reduction was performed urgently under general anesthesia by the boot puller maneuver followed by left calcaneal-talotibial pinning. Additional contention by plaster boot was performed and maintained for six weeks (Figure 3). The radiological control showed good joint congruity after reduction (Figure 4). The patient was hospitalized for observation with the limb elevated for postural drainage for four days. Rehabilitation was undertaken six weeks after the reduction. During follow- up consultations, the patient’s progress was favorable with improved joint mobility and an absence of pain. A return to sports activities was authorized from the third month post- trauma with a follow-up of seven months.

Discussion
Subtalar dislocation, simultaneous dislocation of the talocalcaneal and talo-scaphoid joints, represents approximately 1% of dislocations. The literature is full of numerous clinical cases but lacks recent studies on its management and its long-term evolution in Niger. Allieu [4], in 1967, introduced the term talar-scaphocalcaneal dislocation, specifying that this dislocation can be internal, external, posterior or anterior.
According to the literature data, this dislocation is mainly due to three types of trauma: road traffic accident, fall from a high place, sports accident. Candau [5], as well as Patel, et al. [6], emphasize that a trauma of high intensity is necessary to induce a subtalar dislocation, which is confirmed in our study where the patient suffered a dislocation following a road accident involving a skid of his vehicle. Thus, the external variant occurs during an eversion position. It leads to the following chronological events: rupture of the anterior portion of the deltoid ligament at its distal insertion, then rupture of the astragalocalcaneal interosseous ligament and finally rupture of the dorsal taloscaphoid ligament [7].
After clinical examination, a standard X-ray of the ankle from the front and side is necessary to confirm the diagnosis as well as the associated lesions. It is also recommended to perform a CT scan [7, 8] after treatment to objectify osteocartilaginous lesions and joint damage at the talocalcaneal level. Magnetic Resonance Imaging is useful in the diagnosis of avascular necrosis [9].
The treatment consists of an emergency reduction under general anesthesia. This is done by the boot-puller maneuver described by the classic authors Boehler L [10]. Patient in the supine position, Knee flexed at 90° to release the triceps, One hand placed on the antero-superior region of the tibiotarsal ensures the support of the lower limb, the other hand grasps and pulls the foot forward in plantar flexion as if to pull off a boot. Malgaigne JF [11] recommends exerting an impulse on the head of the talus to guide it towards the articular sphere. 15 to 20% of lateral dislocations cannot be reduced by talonavicular or tendon interposition (tibialis posterior, long flexor of the hallux) [12]. Stabilization by pins, associated with a 6-week plaster cast (this was the case for our patient), carried out by some authors, is suspected of stiffening but is a guarantee against instability [13]. Other authors only carry out a 6-week plaster cast to maintain the reduction.
The outcome of these LSTs is Punctuated by four Major Complications: Stiffness is the most frequent complication, osteoarthritis, avascular necrosis of the talus and instability of the subtalar joint [14, 15, 16] .
Conclusion
Pure external taloscaphocalcaneal dislocation is a rare condition most often secondary to high-energy trauma. Emergency management is required after a clinical assessment in order to perform emergency reduction by external maneuvers. In the majority of cases, a closed reduction is sufficient, but if the dislocation is irreducible, open, or unstable, surgical treatment should be considered.
Conflict of Interest: The authors have reported no conflict of interest. Data Availability: All data are included in the article content.
References
-
Leitner B (1954) Recent subtalar dislocation of the foot with tibiotarsal subluxation of the talus. Rev Chir Orthop 40(2): 232-235.
-
Wang HY, Wang BB, Huang M, Wu XT (2020) Treatment of closed subtalar joint dislocation: A case report and literature review. Chin J Trauma 23(6): 367-371.
-
Benabbouha A, Ibou N (2022) Rare case of pure medial subtalar dislocation in a basketball player. Pan Afr Med J 23(106).
-
Allieu Y (1967) Internal talar-scaphocalcaneal dislocation: experimental study of the mechanism based on 10 cases. Thesis, Médecin Montpellier.
-
Candau B, Rogez JM, Letenneur J (1978) Astragalo- scapho-calcaneal dislocation J chir 115: 279-284.
-
Patel J, Vianney Y (1913) On the subtalar dislocation of the foot inwards. Chir Orthop Review 1: 1-14.
-
Rammelt S, Goronzy J (2015) Subtalar dislocations. Foot Ankle Clin 20(2): 253-264.
-
Macey ARM, Grama C (2016) An ankle that just didn’t look right. BMJ 355: i5056.
-
Jarde O, Boulu G, Havet E, Gabrion A, Vives P (2001) Complete transverse fractures of the talus: Value of MRI for the detection of ischemic necrosis. Acta Orthop Belg 67(1): 60-67.
-
Boehler L (1944) Fracture treatment technique. Med de France 9-P-2-5(1443-1449).
-
Malgaigne JF (1855) Treatise on fractures and dislocations, In: JB Baillerie (ed.), Paris, France, pp: 1030-1070.
-
Meyer JM, Hoffmeyer P (1985) subtalar dislocation. Med and Hyg 43: 1520-1522.
-
Tricoire JL, Colombier JA, Chiron P, Duraffour H, Puget J, et al. (1989) Subtalar dislocations: prognostic assessment, therapeutic approach. Strasbourg, 9th Congress of Emergency Surgery.
-
DeLee JC, Curtis R (1982) Subtalar of the foot. J Bone Joint Surg 64: 433-437.
-
Prada-Canizares A, Martin IA, Rico JV (2016) Juan Pretell Mazzini. Subtalar dislocation: management and prognosis for an uncommon orthopedic condition. Int Orthop 40: 999-1007.
-
Inokuchi S, Hashimoto T, Usami N (1997) Posterior Subtalar dislocation. J Trauma 42 (2): 310-313.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results
- Management of Complications from Traditional Treatment of Locomotor System Injuries at the National Hospital of Niamey: A Report of 220 Cases