Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results
Introduction: Treating surgical site infection (SSI) remains a challenge for surgeons in sub-Saharan Africa and the West. This study aimed to present the surgical indications and results obtained in managing SSI in orthopaedics and traumatology in a developing country.Patients and Method: This was a descriptive cross-sectional study carried out in the orthopaedics and traumatology department of a teaching hospital in the city of Yaounde over 5 years. It included all patients who had presented with postoperative infection after orthopaedic or traumatological surgery and who had undergone surgical management. The Student's t-test was used for the comparison of quantitative variables, and the Chi-Square or Fisher's Exact test for qualitative data.Results: Of the 65 cases collected, 61 cases (94%) had deep and 4 cases (6%) superficial SSIs. Pus was found in 98% of cases.The surgical indications were DAIR (Debridement Antibiotic Implant Retention) in 21 cases (32%), DAIEX (Debridement Antibiotic Implant Exchange) in 17 cases (26%) and DROM (Debridement and Removal of Osteosynthesis Material) in 18 cases (28%), DAIS (Debridement Antibiotic Implant Sterilization) in 5 cases (8%). Four patients did not undergo surgery. Culture was positive in 95% of cases, and 104 germs were isolated. The main ones were Staphylococcus aureus (23%),Klebsiella pneumoniae (14%), Enterobacter Cloacae (13%) and Escherichia coli (11%). The postoperative course of patients was marked by recovery without sequelae in 43 cases (66%), with sequelae in 13 cases (20%), and recurrence of infection in 9 cases (14%). There was no association between the type of surgical indication and recurrence of infection.Conclusion: The key to curing SSI is early diagnosis, with timely management combining surgery and antibiotic therapy.
Muluem OK¹, Nyankoue MF², Nyekel JR³, Elomo A², Tsiagadigui JG², Guemse ME² and Handy ED¹
¹Department of surgery, Yaounde General Hospital, Cameroon ²Department of surgery, Yaounde 1 University, Cameroon ³Department of surgery, Douala University, Cameroon
Abbrevations
DAIR: Debridement Antibiotic Implant Retention; DAIEX: Debridement Antibiotic Implant Exchange; DROM:
Debridement Removal of Osteosynthesis Material; DAIS: Debridement Antibiotic Implant Sterilisation; SSI: Surgical site infection; FLIPS: French-language Infectious Pathology Society; ROM: Removal of Osteosynthesis Material.
Introduction
Surgical Site Infection (SSI) in orthopaedics and Traumatology is defined as an infection occurring within 30 days of surgery, or within one year in the presence of implants, prostheses or prosthetic devices [1]. Their prevalence in sub-Saharan Africa varies between 9% and 12% [2, 3, 4, 5], yet according to the US National Research Council, the acceptable rate should be less than 5% [6]. SSI is a major concern for surgeons and one of the most dreaded surgical complications. Although relatively rare, SSI in orthopaedic surgery is often serious [7, 8]. When they do occur, they can call into question the benefits of an operation designed to improve function or repair the consequences of trauma, even if, in some cases, they are not life-threatening [9].
Although the diagnosis and identification of risk factors for SSI are easy, management is still difficult, depending on the context, and often requires rigorous treatment combining surgery and antibiotic therapy. In fact, in countries with limited resources, it is sometimes difficult for the patient to pay for all the laboratory biological tests, and sometimes the germ found is only sensitive to injectable antibiotics, increasing the length of hospital stay. The French Language Infectious Pathology Society (FLIPS) has defined recommendations for clinical practice with regard to osteoarticular infections on equipment [10].
Thanks to this work, they have proposed diagnostic and therapeutic approaches to osteoarticular infections on osteosynthesis equipment. Even though the protocols are well defined, their implementation remains a problem in developing countries, due to insufficient diagnostic means and lack of financial resources, as social security or health insurance is not accessible to the majority [11].
Despite this difficult context and working environment, some authors have taken an interest in the management of SSI in orthopaedics in sub-Saharan Africa, which has led to satisfactory results and improved patient prognosis. These include Handy D, et al. [12], Fokam, et al. [4], in Cameroon, Ayouba G, et al. [3] in Togo and Mba Mba C, et al. in Gabon [5]. The Handy, et al. study has the disadvantage of a small sample size (n=4 for 68 operated patients) and a 6-months follow-up, whereas the Fokam study focused solely on the prevalence and risk factors of SSI. F or this reason, we undertook this study, aimed at describing the different methods of treating SSI in orthopaedics-traumatology in the city of Yaounde, using a larger sample and presenting the results to improve the prognosis of these patients. We hypothesized that the treatment of SSI, according to recommendations, would improve patient prognosis in the short and medium term.
Patients and Method
Patients
These were consenting patients over 15 years of age who presented with SSI after clean orthopaedic or trauma surgery with or without the use of an implant. These patients were operated on, medically treated with antibiotics, followed up and reassessed to affirm their cure.
Method
This was a cross-sectional, retrospective, descriptive study conducted in the orthopaedic and traumatology departments of two hospitals in the city of Yaounde. The study was conducted over 5 years and 4 months, from January 2018 to April 30, 2023. It included all consenting patients who had initially undergone clean surgery with or without an implant in orthopaedics or traumatology and who had presented a postoperative infectious complication.
When reviewing the files, the diagnosis of infection on osteosynthesis material was based on the criteria of the 2018 AO consensus, which established an international definition of infection on osteosynthesis material according to two types of criteria [1].
Objective Criteria: Fistula to implant; purulent discharge; the presence of germ confirmed by histopathology on at least two samples.
Suggestive criteria requiring the search for an objective criterion: pain-redness-warmth-swelling; fever associated with persistent discharge from the surgical wound or effusion in the vicinity of an osteosynthesis material; elevated VS and CRP; bone lysis around the implant, non- union, sequestration or periosteal reaction [13].
The variables studied were socio demographic (age, sex), clinical (comorbidities, site of lesion, type of surgery prior to SSI, implant used), therapeutic (surgical technique used to treat SSI) or bacteriological (germ identified, antibiotic therapy and duration) and prognostic (recovery time, complications).
The surgical technique used in the operating room was researched according to the procedure performed. We therefore identified the following techniques: • DAIR (Debridement Antibiotic Implant Retention) when the infection occurred on osteosynthesis material before 30 days.
• DAIEX (Debridement, Antibiotic Implant Exchange) when infection occurred on osteosynthesis material after 30 days.
• DAIS (Debridement Antibiotic Implant Sterilization) if the implant was removed, sterilized and then re- implanted.
• ROM (Removal of Osteosynthesis Material) combined with debridement when the fracture was consolidated on infected material.
• Simple debridement when infection occurred in the absence of material.
• The Masquelet Technique (filling the bone void with a cement spacer) when debridement was accompanied by loss of bone substance.
• Limb amputation in cases of diffuse bone infection with soft-tissue necrosis.
During surgery, a sample was taken for bacteriological analysis, and probabilistic antibiotic therapy was prescribed pending bacteriological results. Depending on the bacteriological flora and antibiotic sensitivity, monotherapy, bitherapy or tritherapy was prescribed.
Between 6 - 60 months, patients were invited for a final evaluation. Complete healing was achieved when the patient showed no clinical signs of infection (fistula), negative biology (CRP and VS normal) and consolidation on follow-up radiography.
Data were analyzed using SPSS (Statistical Package for Social Sciences) version 26. Qualitative variables were expressed as headcount and frequency, while quantitative variables were expressed as means (standard deviations) in the case of a normal data distribution, or as medians (interquartile ranges) in the case of an asymmetric distribution.
Quantitative variables were compared using Student’s T-test for independent data in the case of normal distribution, or the Mann Whitney-U test for non-parametric data. For qualitative data, the chi-square test or Fisher’s exact test was used.
Results
The series
Sixty-five patients participated in the study. The median age of the patients was 42.35 ± 13.37 years, with extremes of 20 and 75 years. There were 43 men and 22 women, giving a M/F sex ratio of 1.95.
Comorbidities were frequent in 26 cases (31%), dominated by arterial hypertension 13 cases (20.0%), HIV
5 cases (8%), and diabetes mellitus 3 cases (5%). Patients had undergone surgery for open fracture in 36 cases (55%), closed fracture in 24 cases (37%) and arthroplasty in 3 cases (5%). Internal osteosynthesis was the main surgical technique used (74%), with nails (31%) or plates (21%). The lower limb was the most frequent anatomical site, at 91%, dominated by the leg (46%). SSIs occurred both in hospitalized and outpatients.
The median duration of onset of the first symptoms characteristic of SSI was 20 [5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45] days, with extremes of 1 and 214 days. Local clinical examination revealed a skin fistula and discharge in all cases, and sometimes dehiscence of the surgical wound with exposure of the implant (figure 1B). Of the 65 cases collected, surgical site infections were deep in 58 cases (89%) and superficial in 7 (11%).
Biological aspects were characterized by anaemia (83%) and positive CRP in 82% of cases. Standard radiography was the only morphological examination performed and was not systematic. It revealed implant loosening (4%) followed by dislocation of the prosthesis (3%).
| Variable | Number (n) | Frequency (%) |
|---|---|---|
| Surgical technique | ||
| DAIR | 21 | 32 |
| DAIEX | 17 | 26 |
| DROM | 18 | 28 |
| DAIS | 5 | 8 |
| Non operated | 4 | 6 |
| Total | 65 | 100 |
Table 1: ** Surgical Treatment.
DAIR: Debridement Antibiotic Implant Retention DAIEX: Debridement Antibiotic Implant Exchange DROM: Debridement Removal of Osteosynthesis Material DAIS: Debridement Antibiotic Implant Sterilisation Table 1: Surgical Treatment.
Surgical treatment of SSI (Table 1)
The majority of surgical interventions were elective in 31 cases (48%) for SSI diagnosed late. All operations were performed in the operating theatre under anaesthesia. Pus was found in 98% of cases, and necrotic tissue in 58%. Debridement was performed in all patients (100%).
In the presence of an implant, DAIR was performed in 21 patients (32%), DAIEX in 17 (26%), DAIS in 5 (8%) and debridement combined with ROM in 18 (28%) patients. Of the 17 patients who underwent DAIEX, 10 (59%) were operated on using the Masquelet technique (Figure 1A-1E).
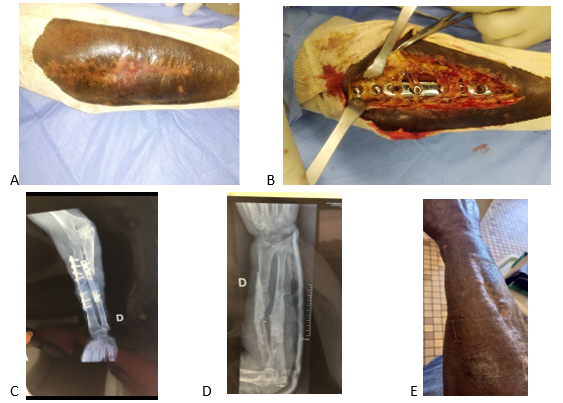
A. Presence of a fistula B. Presence of pus and plate intraoperatively C. Debricolage of material in infectious environment D. Material removal + 1st Masquelet step E. Wound and infection healing Figure 1: Chronic Screw-Plate Infection of Both Forearm Bones.
Bacteriological profile of SSI
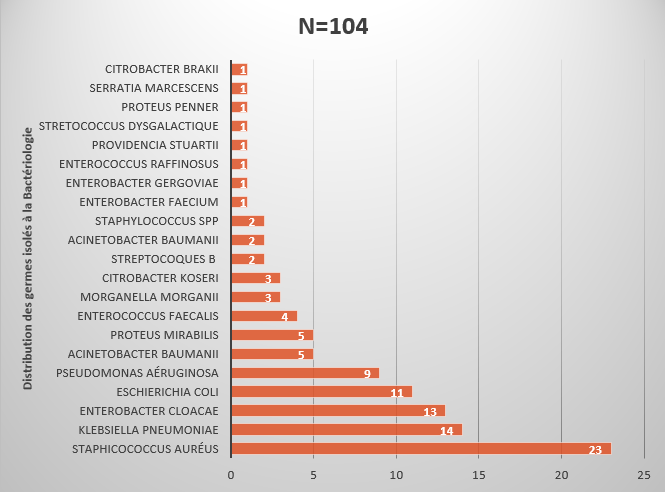
After bacteriological analysis, 35 patients had a poly- microbial infection (54%) and 30 had a mono-microbial infection (46%). A total of 104 germs were isolated, the main ones being: Staphylococcus aureus 23 (23%), Klebsiella pneumoniae 14 (14%) and Enterobacter cloacae 12 (13%) (Figure 2).
According to antibiotic sensitivity, monotherapy was prescribed for 5 patients (8%), dual therapy for 31 (48%) and triple therapy for 29 (44%) patients. The most commonly prescribed antibiotics were gentamicin (35.4%), amikacin (26.2%), imipenem (21.5%), ciprofloxacin (20%) and ofloxacin (16.9%).
The duration of antibiotic therapy varied according to chronicity, severity of infection and disappearance of the inflammatory biology syndrome. The duration was less than 20 days in 3 cases (5%), 20-40 days in 29 cases (45%), 40-60 days in 19%, 60-80 days in 15 cases (23%) and more than 80 days in 6 cases (9%).
Post-operative course
The median hospital stay was 5 [2, 3, 4, 5, 6, 7, 8, 9, 10] days, with extremes of 2 and 30 days. Post-treatment evolution was marked by recovery without sequelae in 43 cases (66%), with sequelae in 16 cases (24,6%), and persistent infection in 9 cases (14%). On the other hand, we had 16 (24.6%) cases of healing with sequelae, including 10 (16.4%) of unsightly scarring, 2 (3.3%) of amputation and 4 (6.6%) of stiffness.
Discussion
This study reports on the surgical and medical management of SSI in a developing country. It is limited by its retrospective nature, which prevented us from recruiting a larger sample.
In our series, the median age of patients was 42.35 ± 13.37 years, with 66% being male. Many African authors have found similar results [3, 4, 5, 14]. This age group represents the proportion of patients more prone to trauma, surgery and SSI.
Patients had undergone fracture surgery in 92% of cases, of which 55% were open fractures, 37% closed fractures and 5% arthroplasty. The lower limb was the most frequent anatomical site at 97%, dominated by the leg at 46%. Indeed, road traffic accidents are the leading cause of trauma in developing countries requiring orthopaedic surgery. In addition to the risk factors associated with the working environment and the technical platform, factors such as skin opening and the complexity of fracture lines in the case of high-energy trauma increase the risk of infection [15, 16, 17]. These results are similar to those of Ngaroua, et al. [18], who found a frequency of 57.9% for open fractures, of which 40.6% involved the leg. Other authors such as Ide Garba. et al, Malick. et al, Madougou. et al, have also reported a predominance of SSI after osteosynthesis of fractures in the proportions 82.1% ;75.23%; and 88.72% respectively [2, 19, 20].
Diagnosis of SSI was primarily clinical, with local examination showing a skin fistula or discharge from the surgical wound in all cases. The aetiology was identified on bacteriological examination. Most of these clinical signs were related to deep infection, especially in the presence of an implant. These signs accounted for 89% in our study, rates comparable to those of Ide Garba et al, who found 85% deep infection in 2018 in Cotonou [2].
The main germs found were Staphylococcus aureus at 23.1%, Klebsiella Pneumoniae at 13.5% and Enterobacter cloacae at 12.5%, Escherichia coli at 10.6% and Pseudomonas aeruginosa at 8.7%. In 53.8% of cases, the infections were polymicrobial. Staphylococcus aureus is a commensal germ found on the skin and nostrils. It is the most frequent germ in orthopaedic SSIs, both in Africa [2, 3, 4, 5, 12, 21, 22] and in the West [23, 24, 25]. The association with other Gram-negative and Gram-positive germs is sometimes the result of hospital contamination (nosocomial infection). This is constant in other series but at different rates.
The antibiotics most prescribed after culture results were gentamicin (35.4%), amikacin (26.2%), imipenem (21.5%) and ciprofloxacin (20.0%). These results are similar to those of Ousmane A et al, who found the same sensitivity rates for the aminoglycosides tested (Amikacin 26.1%, Gentamicin 38.9%) (10). These results lay a problem ; As aminoglycosides can only be prescribed for less than 10 days, combination therapy with another molecule is often recommended [10].
The aim of treatment of infections on osteosynthesis equipment is to eradicate the infectious site, so as to obtain a pain-free, healed joint or bone [26]. According to the literature, there are four approaches to surgical treatment: definitive removal of the implant, debridement with the implant in place, debridement with one-stage implant replacement, and two-stage implant replacement [27, 28, 29].
Surgically, debridement was performed in all surgical patients with SSI, thus ensuring detersion of the infected site before antibiotics were prescribed. This is in line with recommendations for the management of SSI [29]. Implant retention was performed in 32% of cases, and implant replacement in 26%. This result is significantly lower than that of Rodham, et al. [30], who reported a 72.2% rate of DAIR in a retrospective study of the long-term outcome of the treatment of post-fracture limb osteitis.
In fact, the rate of early diagnosis of SSI and immediate surgical management is higher in Western countries, where the majority of patients are covered by social security, than in developing countries, where the diagnosis and treatment of SSI is sometimes delayed, contraindicating the DAIR technique. All other techniques, such as DAIEX, DROM and DAIS, were used in cases of late infection. DAIS is a new concept that we have developed in our working environment for hip prosthesis infections. Indeed, when DAIEX had to be performed, and in the event of difficulty in acquiring a new implant (prosthesis), we would remove the primary prosthesis and ensure its decontamination and sterilization; then re-implant it on the patient during the same operation. This technique prolonged operating time but enabled optimal debridement.
The median operating time was 60 minutes, with extremes of 45 and 150 minutes. These ranged from simple debridement to removal or replacement of osteosynthesis material. This operating time was significantly shorter than that of Zhou CH, et al. [31], who in a study published in Guangzhou in 2021 found an operating time of 124 min for one-stage treatment and 257 min for two-stage treatment. In addition, the two-stage procedure included an additional bone transfer procedure, which we did not include in our series.
In our study, the median hospital stay was 5 [2, 3, 4, 5, 6, 7, 8, 9, 10] days, with extremes of 2 and 30 days. This can be explained by the fact that patients treated with ROM were observed for 24 to 48 hours. Those treated with DAIR and DAIEX were hospitalized for 5 to 7 days, with extremes of 10 days. Longer hospital stays were mainly in patients with infectious recurrence, comorbidity, amputees and the financially constrained.
In the medium term, 66% of patients recovered without any sequelae. Nevertheless, this rate is lower than that reported by Rodham et al. and Hu Zhang et al., who found a cure rate of 75% and 92.5%, respectively [30, 32]. Indeed, there is an advent of multi-resistant germs in our hospitals, sometimes leading to the use of expensive antibiotics that are not accessible to all patients, which can influence compliance with treatment. What’s more, in Western countries, prescribing antibiotics for osteoarticular infections is a matter of concertation between infectiologists, biologists and orthopedists. The aim is to ensure that antibiotic therapy is properly administered and that the patient is cured [33]. Such concertation is rare in our environment, which may justify the recurrence rate of 14% in our study, whereas the cure rate is considered acceptable when recurrences are less than or equal to 5%.
Conclusion
SSI remains a worrying reality in orthopaedic and traumatology surgery departments in Yaounde. It requires early diagnosis and management to reduce the risk of recurrence and sequelae. Despite the above-average cure rate, much remains to be done in collaboration with other specialties to reduce the recurrence rate to an acceptable level. Primary and secondary prevention require compliance with asepsis rules, knowledge of SSI risk factors by all hospital personnel, and good compliance to avoid the advent of bacterial strains resistant to standard antibiotics.
Conflict of Interest
Advent.
References
-
Berríos-Torres SI, Umscheid CA, Bratzler DW, Leas B, Stone EC, et al. Madougou S, Tchomtchoua AS, Gandaho H, Essoun S. (2010) Measuring surgical site infection after femur and tibia centromedullary nailing osteosynthesis at the CNHU of Cotonou (BENIN). Le Bénin Médical N°44- (2017) Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection. JAMA Surg 152(8): 784‑791.
-
Idé G, Wahab MA, Hama Y, Habibou DMM, Hans-Moevi A (2018) Surgical Site Infection in Ortho-Traumatological Surgery at the CNHU-HKM in Cotonou. Health Sci Dis 19(2).
-
Ayouba G, Bakriga B, Dellanh, Kombate NK, Towoezim YYTH, Akloa KEK, Abalo A (2022) Infections on Osteosynthesis Material in Orthopaedics: Problems of Management at the Sylvanus Olympio University Hospital, Lomé. Health Sci Dis 23(6): 77-81
-
Fokam P, Mvodo A, Handy E, Nana TC, Ngowe MN (2022) Prevalence and predictive risk factors of surgical site infection following orthopaedic surgery in Yaoundé. Rev Médecine Pharm 11(2): 1247‑50.
-
Mba Mba C, Nguiabanda L, Okome Obiang IM, Nguema Enzengue F, Nteph JP, et al. (2023) Osteosynthesis Material Infections at Owendo University Hospital (Gabon): Epidemioclinical, Bacteriological and Therapeutic Aspects. Health Sci Dis 24(10): 78-82
-
National Rsearch Council Post-operative wound infection. Ann Surg 160(2): 1-192.
-
Uçkay I, Agostinho A, Stern R, Bernard L, Hoffmeyer P, et al. (2011) Occurrence of fever in the first postoperative week does not help to diagnose infection in clean orthopaedic surgery. Int Orthop 35(8):1257‑1260.
-
Vallet B, Mignon L, Bordy O (2008) Nosocomial infections, practitioner responsibility and patient information. Press kit.
-
Despales N (2000) Nosocomial infections in orthopaedic surgery. Encycl Méd Chir Elsevier Musculoskeletal System 14-016-B-10, UK, pp: 11.
-
Guery B, Roblot F, Schmit J-L, Strady C, Varon E (2009) Recommendations for clinical practice. Osteoarticular infections on material (prosthesis, implant, osteosynthesis. French Society of Infectious Pathology, pp: 62.
-
Walla A, Abalo A, James EY, Ayouba G, Amakoutou K, Dossim AM (2014) Chronic osteomyelitis in adults: problems of lesion diagnosis and treatment in an under-equipped environment. J Rech Sci Univ, Lomé (Togo), 16(2): 437-441.
-
Handy D, Kingue TN, Bayiha JE, Nanfack C (2016) Surgical Site Infections in Orthopaedic Surgery: Clinical presentations, etiologies and management. Journal of Medicine and Pharmacy 6.
-
Metsemakers W, Morgenstern M, McNally MA, Moriarty TF, McFadyen I, et al. (2018) Fracture-related infection: A consensus on definition from an international expert group. Injury 49(3): 505510.
-
Doutchi M, Harissou A, Lawali Y, Lawan O, Magagi IA, et al. (2020) Surgical Site Infections at Zinder National Hospital, Niger: Epidemiological and Bacteriological Aspects. European Scientific Journal 16: 576-589.
-
(2001) Nosocomial infections in orthopaedic surgery. Thesis N 202/2001/Casablanca
-
Chauvet J, SavorninCI, Tripon PH, Casanova G, Gandon F (1986) Diaphyseal septic pseudarthrosis. Current treatment guidelines based on a series of 80 cases. Ann chir 40: 633-640.
-
Cirotteau BJ, Huard Y, Tomeno B (1974) Critical study of failures in the treatment of femoral shaft fractures: 330 cases. Rev chir orthop 60: 465-483.
-
Ngaroua, Ngah JE, Bénet T, Djibrilla Y (2016) Incidence of surgical site infections in sub-Saharan Africa: systematic review and meta-analysis. Pan Afr Med J 24(171).
-
Malik MHA, Harwood P, DiggleP, Khan SA (2004) Factors affecting rates of infection and nonunion in intramedullary nailing. JBone Joint Surg [Br] 86-B: 556- 560.
-
Madougou S, Tchomtchoua AS, Gandaho H, Essoun S (2010) Measuring surgical site infection after femur and tibia centromedullary nailing osteosynthesis at the CNHU of Cotonou (BENIN). Le Bénin Médical N°44-.
-
Traoré T, Diallo M, Moussa AK, Amossouf, Chigblo P, et al. (2020) Surgical site infection (SSI) in orthopedic surgery at Sikasso Hospital. Mali médical, pp: 6-20.
-
Abdoulaye O, Amadou MLH, Amadou O, Adakal O, Larwanou HM, et al. (2018) Epidemiological and bacteriological aspects of surgical site infections (SSI) in surgical departments at Niamey National Hospital (NNH). Pan Afr Med J 31: 33.
-
Laffosse JM, Reina N, Gaudias J, Coudane H, Mabit C, et al. (2012) Early surgical site infection in adult trauma. Retrospective results and identification of risk factors. Rev Chir Ortho et Traum 98(6): 612-619.
-
Bonnevialle P, Bonnomet F, Philippe R, Loubignac F, Rubens-Duval B, et al. (2012) Early surgical site infection in adult extremity trauma: a prospective multicenter survey. Rev de Chir Ortho et Traum 98(6): 605-611.
-
Morgenstern M, Erichsen C, Militz M, Xie Z, Peng J, et al. (2021) The AO trauma CPP bone infection registry: Epidemiology and outcomes of Staphylococcus aureus bone infection. J Orthop Res 39(1): 136-146.
-
Borens O, Nussbaumer F, Baalbaki R, Trampuz A (2009) Diagnosis and treatment of orthopaedic implant infections. Rev Med Suisse 5: 2563-2568.
-
Govaert GAM, Kuehl R, Atkins BL, Trampuz A, Morgenstern M, et al. (2020) Diagnosing Fracture-Related Infection: Current Concepts and Recommendations. J Orthop Trauma 34(1): 817.
-
Moriarty TF, Kuehl R, Coenye T, Metsemakers W-J, Morgenstern M, et al. (2016) Orthopaedic device- related infection: current and future interventions for improved prevention and treatment. EFORT Open Rev 1(4): 8999.
-
Zeller V, Lhotellier L, Kitzis MD, Ziza JM, Mamoudy P, et al. (2004) Treatment of bone infections caused by foreign material. The Infectiologist’s Newsletter -Tome XIX - n° 6(12): 204-216.
-
Rodham P, Panteli M, Qin C, Harwood P, Giannoudis PV (2023) Long-term outcomes of lower limb post- traumatic osteomyelitis. Eur J Trauma Emerg Surg 49(1): 539‑549.
-
Zhou CH, Ren Y, Song HJ, Ali AA, Meng XQ, et al. (2021) One-stage debridement and bone transport versus first- stage debridement and second-stage bone transport for the management of lower limb post-traumatic osteomyelitis. J Orthop Transl 28: 21‑27.
-
Zhang H, Zhao X, Yang X, Zhang X, Chen X, et al. (2023) Comparison of internal and external fixation after debridement in the Masquelet technique for Cierny- Mader type IV tibial post-traumatic osteomyelitis. Injury 54(2): 422‑428.
-
Metsemakers W-J, Morgenstern M, Senneville E, Borens O, Govaert GAM et al. (2020) General treatment principles for fracture related infection: recommendations from an international expert group. Arch Orthop Trauma Surg 40(8): 10131027.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Management of Complications from Traditional Treatment of Locomotor System Injuries at the National Hospital of Niamey: A Report of 220 Cases