Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
Introduction: Dynamic knee alignment is a key determinant in the planning and success of total knee arthroplasty. Although intraoperative navigation enables assessment of the dynamic phenotype under unloaded conditions, its correspondence with weight-bearing knee function during gait remains unclear. Objective: To evaluate the relationship between dynamic phenotypes obtained passively intraoperatively under unloaded conditions and those measured under active load during gait. Methods: A prospective study was performed on 28 patients undergoing navigated total knee arthroplasty. The dynamic phenotype of each knee was classified into nine categories according to coronal alignment at extension and throughout flexion. Two variables were defined: (1) full-range dynamic phenotype and (2) midflexion dynamic phenotype corresponding to the functional range during gait. Concordance between loaded and unloaded conditions was assessed using Cohen’s kappa coefficient and percentage of agreement. Results: Agreement between unloaded and loaded phenotypes was 57% for full-range and 68% for midflexion. Varus knees showed higher correlation in midflexion, whereas valgus knees demonstrated differences between passive and weight-bearing conditions. Conclusion: Intraoperative passive assessment remains a valuable guide to the knee’s dynamic phenotype, especially in midflexion, yet a functional assessment under loading can express alternative phenotypes that are not always evident in unloaded conditions. Both computer-assisted surgical systemsand preoperative gait analyses provide valuable information for surgical decision-making and may be combined to optimize the characterization of each patient’s dynamic phenotype.
Abbreviations
TKA: Total Knee Arthroplasty; ULC: Unloaded Condition; LBC: Load-Bearing Condition.
Introduction
Total knee arthroplasty (TKA) is one of the most commonly indicated surgical procedures for the treatment of advanced knee osteoarthritis. Its primary goal is to relieve pain and restore joint function while ensuring implant longevity. Traditionally, the success of the procedure has been closely associated with the accurate restoration of a neutral mechanical axis of the lower limb. However, more recent approaches have questioned this paradigm, suggesting that, due to the high inherent variability in the coronal plane, a neutral alignment cannot be considered a universally applicable standard for all patients [1, 2].
The traditional classification into neutral, varus, or valgus alignment does not account for factors such as the orientation of the joint line or its relationship to the overall alignment of the limb and is therefore insufficient to define the various articular phenotypes. To improve postoperative patient satisfaction, new classifications based on functional phenotypes have been proposed. These incorporate additional variables that allow for a more precise characterization of alignment patterns, providing a stronger foundation for surgical planning and the personalization of alignment strategies in TKA [3].
In this context, and in the absence of a universal classification, the CPAK system has been proposed [1]. This system integrates both the hip–knee–ankle angle and the obliquity of the joint line, derived from preoperative imaging studies.
With technological advances, this personalization of surgical planning based on different articular phenotypes has become feasible. Computer-assisted systems such as surgical navigation and robotic assisted surgery have been developed to support this approach. These tools enable real-time quantitative measurement aimed at optimizing both prosthetic alignment and the kinematic profile of the operated limb [4, 5, 6].
Computer-assisted surgery allows the intraoperative acquisition of real-time data for recording joint kinematic information, thereby supporting the surgeon in intraoperative decision-making [5]. However, although this information is dynamic and obtained in real time, it is recorded passively by the surgeon with the patient in the supine position under general anesthesia, and therefore under unloaded conditions. This may compromise its validity for clinical decision-making [7]. During passive intraoperative assessment, the surgeon cannot accurately reproduce the biomechanical environment of weight-bearing, where muscular activation and soft-tissue tension dynamically stabilize the knee joint. The absence of muscle contraction, protective co-contractions, and dynamic ligamentous tension limits the ability of passive evaluation to reflect the functional behavior of the knee during gait.
All current knowledge regarding the biomechanical behavior of the knee under load-bearing conditions is based on gait analysis [8]. At present, gait analysis systems enable a detailed assessment of the forces and movements acting on periarticular and intra-articular knee structures. It has been proposed that the information obtained from such studies not only contributes to a better understanding of the patient’s functional biomechanics but may also be useful for predicting and monitoring anatomical and functional changes occurring postoperatively, as well as the loads transmitted through the articular structures [9].
At present, it remains unknown whether a strong correlation exists between the results obtained from gait analysis (where the patient actively moves the knee while engaging all structures involved in locomotion, that is, under load-bearing conditions) and the measurements obtained intraoperatively passively under unloaded conditions. Should significant differences be confirmed, this would have direct and substantial clinical implications, as all current navigation and robotic systems rely, to varying degrees, on intraoperative kinematic information displayed to the surgeon during the procedure for the analysis of flexion and extension gaps, as well as for decision-making regarding the need for additional bone cuts or soft-tissue releases [5].
The aim of this study is to compare dynamic coronal knee motion phenotypes obtained intraoperatively under unloaded conditions with those obtained from preoperative dynamic gait analysis under load- bearing conditions, to establish comparable patterns and assess the degree of correlation between them.
Materials and Methods
A prospective, single-center study was conducted on a population of patients diagnosed with knee osteoarthritis who, after conservative treatment, continued to experience symptoms severe enough to indicate total knee arthroplasty (TKA). Consecutive patients aged 18 to 89 years who were listed for surgery with a scheduled intervention within six months were included, applying the following exclusion criteria:
- Neurological disorders, otorhinolaryngologic (vestibular or balance) disorders, or visual
- impairments that prevented completion of the preoperative gait study on a treadmill.
- Inability to complete the gait study due to pain or any other physical limitation.
- TKA performed using a manual technique.
- Previous TKA on the contralateral knee.
Sample Size Calculation
For the calculation of the required sample size, an expected sensitivity of 80% (p = 0.8), a confidence level of 95% (α = 0.05), and a total confidence interval width of 26% (precision of 13%) were assumed. This calculation yielded a required sample of 37 patients.
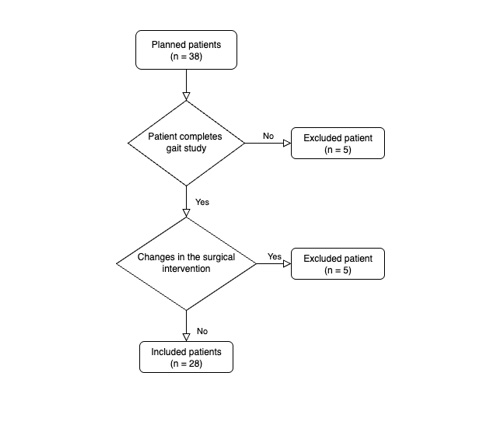
A total of 38 consecutive patients meeting the inclusion and exclusion criteria were recruited. Ultimately, 28 patients were included in the final analysis, as 5 were unable to complete the preoperative gait study due to pain during the procedure, and another 5 underwent modifications to the initially planned surgical intervention, as shown in (Figure 1). This loss of study subjects resulted in a change in the margin of error from ±13% to approximately ±15.3% for the same expected sensitivity (80%) and confidence level (95%). These margins were considered acceptable for the purposes of the study. Therefore, no additional patients were recruited to reach the initially calculated sample size.
The variables collected, along with their corresponding demographic distribution, are presented in (Table 1).
| Variable | Mean ± SD / n (%) |
|---|---|
| Age (years) | 73.1 ± 7.6 |
| Sex | Female: 17 (60.7%) |
| Male: 11 (39.3%) | |
| BMI (kg/m2) | 30.7 ± 5.1 |
| aHKA (degrees º) | 5.9 ± 7.0 |
Table 1: Baseline characteristics of the patients (n = 28). Data are expressed as frequency (n (%)) or as mean ± standard deviati
BMI: body mass index. aHKA: arithmetic hip-knee-ankle angle.
Note: By convention, positive aHKA values indicate varus alignment, whereas negative values indicate valgus alignment. Therefore, an average aHKA of +5.9° corresponds to a mild varus alignment of the cohort. The aHKA was measured on standardized weight-bearing radiographs.
Intraoperative Dynamic Phenotype
The surgical procedure consisted of a primary total knee arthroplasty performed with navigation assistance (Orthopilot version 6.1; B. Braun Aesculap, Tuttlingen, Germany). In all patients, VEGA® posterior-stabilized knee prostheses (B. Braun Aesculap, Tuttlingen, Germany) were implanted.
After patient registration and through a standard anterior knee approach, infrared (IR) optical trackers were placed on the femur and tibia. The centers of rotation of the hip, knee, and ankle were required to determine coronal, axial, and sagittal alignment. The hip and knee centers were identified using a kinematicm method, by rotating the hip and performing flexion-extension movements of the knee. This allowed the navigation system to accurately determine the centers of motion. The ankle center was calculated anatomically using the most prominent points of the medial and lateral malleoli, together with the anterior joint line. Kinematic data were recorded from 0° to 90° of neutral knee flexion, prior to any soft-tissue release or bone cuts.
Based on these data, each knee was classified into one of nine dynamic alignment phenotypes according to the behavior of coronal alignment from full extension through the flexion arc. These nine phenotypes are illustrated in (Figure 2).
- Varus–Varus: varus in extension that remains varus throughout flexion.
- Varus–Neutral: varus in extension that transitions to neutral during flexion.
- Varus–Valgus: varus in extension that transitions to valgus during flexion.
- Neutral–Neutral: neutral in extension that remains neutral throughout flexion.
- Neutral–Varus: neutral in extension that transitions to varus during flexion.
- Neutral–Valgus: neutral in extension that transitions to valgus during flexion.
- Valgus–Varus: valgus in extension that transitions to varus during flexion.
- Valgus–Neutral: valgus in extension that transitions to neutral during flexion.
- Valgus–Valgus: valgus in extension that remains valgus throughout flexion.
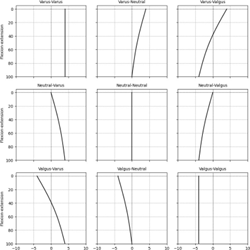
The X-axis represents the coronal alignment (mechanical HKA (mHKA) angle), with valgus alignment plotted to the left and varus alignment to the right, neutral alignment is defined as ±2°. The Y-axis represents the degrees of knee flexion–extension.
This variable was designated as the “full-range dynamic phenotype”. The entire series was independently segmented by three investigators with experience in knee surgery and alignment analysis, in order to minimize the subjective component of the classification process. Interobserver agreement was subsequently quantified using Cohen’s kappa coefficient, allowing the degree of concordance among evaluations to be objectively assessed and the reproducibility of the method to be determined. Fleiss’ kappa values were 0.64 for the unloaded condition and 0.77
for the loaded condition, indicating substantial interobserver reliability [10]. In this way, it was ensured that although the classification might involve an interpretative element, its consistency and reliability were appropriately verified.
Dynamic Phenotype Under Load-Bearing Conditions
The preoperative dynamic behavior of the knee was evaluated through gait analysis performed within 48 hours prior to surgery. The standard protocol commercialized by Emovi Inc., Canada, using the KneeKG™ system, was followed. This protocol analyzes the three-dimensional kinematics of the knee while the patient walks on a conventional treadmill at self-selected comfortable walking speed. This assessment knee motion during both the stance phase (loaded/weight- bearing) and the swing phase (unloaded/non weight- bearing), reflecting the dynamic functional behavior of the joint throughout the entire gait cycle.
The complete study protocol lasts approximately 30 minutes. First, the system is calibrated by placing infrared optical trackers at three anatomical locations: the sacrum (to estimate pelvic and hip motion), the tibia, and the knee (the latter using an exoskeleton designed to adapt to the morphology of the patient’ limb and improve accuracy of measures). Additionally, an infrared emitter–receiver camera (Polaris Vega, NDI, Canada) is positioned laterally to the treadmill to record, in real time, the displacement of the trackers.
During the calibration phase, the patient performs guided movements that allow the system to recognize individual kinematics and adjust the three-dimensional capture of the gait motion. This step is conceptually similar to the registration phase in surgical navigation systems: the center of rotation of the hip is estimated using a circumduction movement, while the anatomical reference of the ankle is derived from the position of the medial and lateral malleoli (mid-malleoli landmark), allowing accurate definition of the lower limb.
These calibration procedures ensure precise alignment and tracking of knee motion in all three planes during gait [11]. Subsequently, free walking cycles of 45 seconds are performed on the treadmill, during which the system records joint motion in all three spatial dimensions. In total, approximately three minutes of continuous data are collected, from which the most reproducible gait cycles are selected for analysis, according to the KneeKG™ protocol criteria (Figure 3).

The investigators responsible for conducting the study received the necessary training and certification in the procedure, thereby ensuring the consistency and reliability of the tests performed. Accuracy, reliability and reproducibility of this device were summarized in a previous publication [12].
Each knee was classified into one of the previously described dynamic phenotypes, using as reference only the alignment behavior at the angle of maximum flexion during gait.
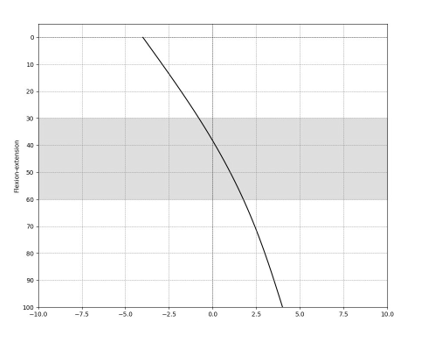
Dynamic Phenotype at Midflexion
Additionally, a second variable was defined, termed the “midflexion dynamic phenotype”, which characterizes the behavior of coronal knee alignment throughout a functional flexion range between 30° and 60° in the unloaded intraoperative assessment. This parameter enables a more specific evaluation of the dynamic alignment pattern within the most representative segment of physiological motion, allowing comparison between gait and intraoperative conditions. Recent findings also suggest that preoperative knee kinematics correlate with intraoperative medial and lateral gap measurements at 30° and 60°, with dynamic alignment showing the strongest influence in midflexion [13] (Figure 4).
Statistical Analysis
For the statistical analysis, the degree of agreement between the dynamic phenotype obtained under load- bearing conditions (through gait analysis) and that obtained under unloaded intraoperative conditions was evaluated using Cohen’s kappa coefficient. While a kappa value between 0.4 and 0.6 is considered as a moderate agreement, a value greater than 0.6 is considered indicative of substantial agreement and therefore deemed clinically relevant [14]. Interobserver reliability was further assessed using Fleiss’ kappa, which yielded values of 0.64 for the unloaded condition and 0.77 for the loaded condition, confirming substantial consistency among observers.
All statistical analyses were performed using IBM SPSS Statistics version 22.0 (IBM Corp., released 2017; Armonk, NY, USA).
Ethical Considerations
Informed consent was obtained from all participants included in the study. Approval was granted by the Ethics Committee for Research of Hospital Universitario Infanta Leonor (Spain). All procedures were conducted in accordance with the ethical standards of the institutional and national research committee and with the 1964 Declaration of Helsinki and its subsequent amendments or comparable ethical standards.
Results
Table 2 presents the distribution of the dynamic alignment phenotypes identified in the dynamic study performed under load-bearing conditions using the KneeKG™ software (LBC, Load-Bearing Condition), and their correspondence with the dynamic phenotypes identified in the intraoperative study performed under unloaded conditions using the Orthopilot software (ULC, Unloaded Condition), both for the full flexion range and more specifically for the midflexion portion.
| LBC | ULC | ULC | |
|---|---|---|---|
| Dynamic Phenotype | KneeKG™ full flexion range | Orthopilot full flexion range | Orthopilot midflexion range |
| (n) | (n with same behavior, | (n with same behavior, | |
| % agreement, [Kappa ± SD]) | % agreement with full range LBC, [Kappa ± SD]) | ||
| Varus-Varus | 17 | 9 (53%) | 15 (88%) |
| Varus-Neutral | 1 | 1 (100%) | 0 (0%) |
| Varus-Valgus | 0 | - | - |
| Varus in extension | 18 | 10 (56%) | 15 (83%) |
| Neutral-Varus | 1 | 1 (100%) | 0 (0%) |
| Neutral-Neutral | 2 | 1 (50%) | 2 (100%) |
| Neutral-Valgus | 0 | - | - |
| Neutral in extension | 3 | 2 (67%) | 2 (67%) |
| Valgus-Varus | 2 | 1 (50%) | 0 (0%) |
| Valgus-Neutral | 4 | 3 (75%) | 1 (25%) |
| Valgus-Valgus | 1 | 0 (0%) | 1 (100%) |
| Valgus in extension | 7 | 4 (57%) | 2 (29%) |
| Total | 28 | 16 (57%) [0.42 ± 0.22] | 19 (68%) [0.47 ± 0.22] |
Table 2: Distribution of dynamic alignment phenotypes.
The first column shows the classification of dynamic phenotypes from the LBC study conducted with the KneeKG™ protocol. The second column displays the number of matching cases and their corresponding percentages (agreement rate) when comparing the LBC phenotype with that of the ULC obtained from the Orthopilot protocol. The third column shows the number of matches and percentages (agreement rate) when comparing the LBC phenotype in full range with the ULC phenotype in midflexion range (knee flexion of 30–60°). Cohen’s kappa coefficient was calculated for the overall analysis.
The distribution of intraoperative alignment phenotypes was consistent with findings from previous studies [4]. Among the 28 knees analyzed, 18 (64%) began in varus alignment, 3 (11%) in neutral, and 7 (25%) in valgus.
Overall Results (n = 28) Of the 28 knees analyzed, 16 (57%) showed moderate concordance between the load- bearing condition (LBC) and the unloaded intraoperative condition (ULC) across the full flexion range, with a Cohen’s kappa coefficient of [0.42 ± 0.22] at a 95% confidence interval. A total of 19 knees (68%) demonstrated concordance between LBC and ULC in midflexion, with a kappa coefficient of [0.47 ± 0.21] at a 95% confidence interval. Genu Varum (n = 18) • Varus–Varus: 17 knees. Of these, 9 (53%) presented the same phenotype under unloaded conditions across the full flexion range, while 15 (88%) maintained it in midflexion. • Varus–Neutral: 1 knee, which showed full concordance (100%) with the unloaded phenotype in the full range but not in midflexion. • Varus–Valgus: no cases were recorded. In total, for knees starting flexion in genu varum, 10 knees (56%) showed concordance in the full range and 17 knees (83%) in midflexion.
Genu Neutral (n = 3) • Neutral–Varus: 1 knee, which showed full concordance (100%) across the full range but not in midflexion. • Neutral–Neutral: 2 knees, of which 1 (50%) coincided in the full range, and both (100%) coincided in midflexion. • Neutral–Valgus: no cases were recorded. In total, for knees starting flexion in genu neutral, 2 knees (67%) coincided in the full range and 2 (67%) in midflexion.
Genu Valgum (n = 7) • Valgus–Varus: 2 knees, of which 1 (50%) coincided in the full range but none (0%) in midflexion. • Valgus–Neutral: 4 knees, of which 3 (75%) coincided in the full range and only 1 (25%) in midflexion. • Valgus–Valgus: 1 knee, which did not show concordance in the full range (0%) but did in midflexion (100%).
In total, for knees starting flexion in genu valgum, 4 knees (57%) showed concordance in the full range and 2 knees (29%) in midflexion.
Discussion
The most relevant finding of this study is that the intraoperative dynamic phenotype determined under unloaded conditions, through passive mobilization of the knee, exhibits moderate correlation compared with the dynamic phenotype recorded under load-bearing conditions through gait analysis. This finding suggests that intraoperative evaluation, even in the absence of physiological load, provides a reliable approximation of the knee’s kinematic behavior during functional activity, particularly in varus knees, and therefore constitutes a dependable tool for intraoperative decision-making when using navigation and robotic-assisted systems.
For the characterization of the knee’s kinetic phenotype, the full range of motion achievable by each patient was analyzed. However, it is important to note that functional load-bearing conditions do not require the use of the complete range of knee motion. During common daily activities such as level walking, the knee operates efficiently within an approximate flexion range of 60°, without the need to reach maximal accurately reflecting how the knee behaves in daily life. Only in more demanding activities (such as stair climbing or descending, standing up from a seated position, or performing athletic movements) are higher degrees of flexion required, but even in these cases the joint rarely reaches its maximal physiological range [15, 16].
In this regard, it is noteworthy that 68% of the knees demonstrated correlation at midflexion of the ULC, and in cases of more severe deformities (varus–varus or valgus– valgus), an almost complete correlation was documented between the phenotypes under unloaded and load-bearing conditions. We were able to observe that the dynamic behavior of the knee differs notably depending on the mHKA axis in extension. In knees with varus alignment, a greater correlation is seen at the midflexion angle; however, the unloaded (intraoperative) study provides complementary information in the last degrees of flexion, where deviations toward neutral or greater varus become evident, allowing for a more precise characterization of the knee’s kinematic profile. In contrast, valgus knees show lower correlation at the midflexion angle, although their behavior becomes better defined when the complete curve is analyzed under unloaded conditions. This difference could be related to the type and magnitude of the existing deformity.
The most marked discrepancies are observed in knees with more severe deformities, where the soft tissues are more stretched or altered. In such cases, the behavior under load may differ significantly from what would be expected from passive mobilization, as tissue and muscular tensions play a more determining role in dynamic stability and alignment. Under this premise, valgus deformities (by generating more pronounced imbalances in knee biomechanics [17, 18, 19] may exhibit poorer correlation between the loaded and unloaded phenotypes, since the influence of soft tissues becomes particularly relevant in this context. In these cases, it is important to complement intraoperative information with dynamic analysis methods under physiological load conditions.
The comparison in ULC between full range of motion and midflexion further suggests that midflexion analysis captures more consistently the LBC pattern, while full-range analysis provides complementary information regarding the last degrees of flexion. Together, both approaches offer a more comprehensive characterization of the knee’s kinematic profile, allowing for the identification of specific behavioral patterns and improving understanding of the relationship between intraoperative dynamic alignment and functional performance.
We consider that the practical implications of this work are twofold. On one hand, navigation and robotic systems provide valuable intraoperative kinematic information that offers a useful approximation of knee behavior during functional loading. Yet, considering the moderate agreement (κ = 0.47), these findings suggest that while intraoperative data are informative, they may not entirely capture the complexity of weight-bearing dynamics, hence a potential value for pre-operative kinematic assessment. On the other hand, centers that do not have access to navigation or robotic systems may use preoperative gait analysis studies such as KneeKG™ to inform the dynamic phenotype, thereby providing valuable information for surgical planning and procedure personalization [20].
The main limitation of this study is that the calculated sample size permits only a descriptive comparison between dynamic phenotypes under loaded and unloaded conditions, thereby limiting the statistical power to detect subtle differences between them or to improve the intergroup kappa correlation. Some patients initially included in the protocol chose not to complete certain phases of the study (either due to pain, discomfort during gait analysis, or changes in surgical indication) which required adjusting the beta error of the sample.
Another limitation to be acknowledged is the potential lack of representativeness of the sample, as it consists of patients selected from a single center. This may influence the generalizability of the results to other populations or clinical settings.
Finally, although gait analysis was performed following a standardized protocol and by formally trained and certified investigators, a certain margin of error in data collection cannot be completely excluded.
Variability in anatomical landmark localization may occur due to individual morphology—particularly in patients with higher BMI—which can make precise sensor placement more challenging.
However, previous validation studies comparing the KneeKG™ system with the EOS Imaging System in patients with elevatedmBMI have demonstrated high measurement accuracy, supporting the reliability of the present dataset [21]. Likewise, the unfamiliarity of some patients with treadmill walking may have led to a gait pattern differing slightly from their usual one (typically slower and more cautious) which could influence the final interpretation of the results.
Nevertheless, we believe that the aforementioned limitations do not invalidate the clinical applicability of our findings, as they provide surgeons with sufficient confidence in decision-making regarding flexion and gap-balancing, even when measurements are obtained under unloaded conditions.
Conclusion
The dynamic phenotype obtained through intraoperative passive mobilization of the knee under unloaded conditions represents, in most cases, a reliable approximation of the dynamic phenotype observed under functional loading conditions during gait.
These findings support the validity of intraoperative passive assessment as a useful tool for surgical planning in total knee arthroplasty (TKA) and suggest that the integration of dynamic analysis methods under loaded conditions may provide complementary information, particularly in cases with complex deformities or mixed phenotypes.
Overall, the results indicate that both computer-assisted surgical systems and preoperative gait analyses provide valuable information for surgical decision-making and may be combined to optimize the characterization of each patient’s dynamic phenotype.
Conflict of Interest
Bianca Marois, Alix Cagnin, and Alex Fuentes are employees of Emovi ICS. Michael Utz is an employee of Aesculap AG. The remaining authors declare no financial interests or conflicts of interest.
References
-
MacDessi SJ, Griffiths-Jones W, Harris IA, Bellemans J, Chen DB (2021) Coronal Plane Alignment of the Knee (CPAK) classification: a new system for describing knee phenotypes. The Bone & Joint Journal 103-B(2): 329- 337.
-
Howell SM, Howell SJ, Kuznik KT, Cohen J, ML Hull (2013) Does A Kinematically Aligned Total Knee Arthroplasty Restore Function Without Failure Regardless of Alignment Category? Clinical Orthopaedics & Related Research 471(3): 1000-1007.
-
Hirschmann MT, Moser LB, Amsler F, Behrend H, Leclerq V, et al. (2019) Functional knee phenotypes: a novel classification for phenotyping the coronal lower limb alignment based on the native alignment in young non-osteoarthritic patients. Knee surg sports traumatol arthrosc 27(5): 1394-1402.
-
Larrainzar-Garijo R, Murillo-Vizuete D, Garcia-Bogalo R, Escobar-Anton D, Horna-Castiñeiras L, el al. (2017) Dynamic Alignment Analysis in the Osteoarthritic Knee Using Computer Navigation. J Knee Surg 30(09): 909- 915.
-
Deep K, Picard F, Baines J (2016) Dynamic knee behaviour: does the knee deformity change as it is flexed—an assessment and classification with computer navigation. Knee surg sports traumatol arthrosc 24(11): 3575-3583.
-
McClelland JA, Webster KE, Feller JA (2007) Gait analysis of patients following total knee replacement: A systematic review. The Knee 14(4): 253-263.
-
Jenny JY, Dillmann G, Gisonni V, Favreau H (2019) Noninvasive navigated assessment of the lower limb axis prior to knee arthroplasty: a feasibility study. Eur J Orthop Surg Traumatol 29(4): 855-860.
-
Freeman MAR, Pinskerova V (2003) The movement of the knee studied by magnetic resonance imaging. Clin Orthop Relat Res 410: 35-43.
-
Minns RJ (2005) The role of gait analysis in the management of the knee. The Knee 12(3): 157-162.
-
Albakkosh I (2024) Using Fleiss’ Kappa Coefficient to Measure the Intra and Inter-Rater Reliability of Three AI Software Programs in the Assessment of EFL Learners’ Story Writing. IJESA 3(1): 69-96.
-
Hagemeister N, Parent G, Van De Putte M, St-Onge N, Duval N, et al. (2005) A reproducible method for studying three-dimensional knee kinematics. Journal of Biomechanics 38(9): 1926-1931.
-
Lustig S, Magnussen RA, Cheze L, Neyret P (2012) The KneeKG system: a review of the literature. Knee Surg Sports Traumatol Arthrosc 20(4): 633-638.
-
Ranger P, Marois B, Cagnin A, Kazouiny El, Fuentes A (2025) Preoperative dynamic coronal alignment markers are associated with intraoperative gaps in handheld robotic-assisted total knee arthroplasty: Pilot analysis. presentado en ISTA 2025. International Society for Technology in Arthroplasty, Rome.
-
Landis JR, Koch GG (1977) The Measurement of Observer Agreement for Categorical Data. Biometrics 33(1): 159.
-
Kadaba MP, Ramakrishnan HK, Wootten ME (1990) Measurement of lower extremity kinematics during level walking. Journal Orthopaedic Research 8(3): 383- 392.
-
Wimmer MA, Nechtow W, Schwenke T, Moisio KC (2015) Knee Flexion and Daily Activities in Patients following Total Knee Replacement: A Comparison with ISO Standard 14243. BioMed Research International pp: 1-7.
-
Huang J, Sun H, Li D, Wang Y, Xu J, et al. (2023) Knee valgus deformity and lateral bone defects affect the function of superficial medial collateral ligament: A finite element analysis. Journal of Orthopaedics 40: 17- 22.
-
Khou SB, Saki F, Tahayori B (2024) Muscle activation in the lower limb muscles in individuals with dynamic knee valgus during single-leg and overhead squats: a meta-analysis study. BMC Musculoskelet Disord 25(1): 652.
-
Clarke HD, Fuchs R, Scuderi GR, Scott WN, Insall JN (2005) Clinical Results in Valgus Total Knee Arthroplasty With the “Pie Crust” Technique of Lateral Soft Tissue Releases. The Journal of Arthroplasty 20(8): 1010-1014.
-
F Bensalma, Nicola H, Alix C, Youssef O, Nathalie J, et al. (2022) Biomechanical markers associations with pain, symptoms, and disability compared to radiographic severity in knee osteoarthritis patients: a secondary analysis from a cluster randomized controlled trial. BMC Musculoskelet Disord 23(1): 896.
-
Clément J, De Guise JA, Fuentes A, Hagemeister N (2018) Comparison of soft tissue artifact and its effects on knee kinematics between non-obese and obese subjects performing a squatting activity recorded using an exoskeleton. Gait Posture 61: 197-203.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results
- Management of Complications from Traditional Treatment of Locomotor System Injuries at the National Hospital of Niamey: A Report of 220 Cases