Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
Introduction: Locked intramedullary nailing is the gold standard for the treatment of tibial shaft fractures. The use of a locked humeral nail for this technique is rare and scarcely reported in the literature. This approach was precisely the one employed in the present case. Case Report: A 57-year-old woman was admitted for a closed left leg injury. The radiological and clinical examination revealed a closed leg fracture (42A1 according to the AO classification). It was associated with skin damage (Tscherne-Götzen stage 1). The patient was of small stature (1.48 meters, shoe size 32) due to a growth anomaly related to poliomyelitis in childhood. An emergency locked intramedullary nailing was performed in the tibia. It was done with a 260mm long humeral nail (due to the unavailability of tibial nails of this small size), and the impossibility to place a screw plate due to skin suffering. A posterior plaster boot splint was applied postoperatively, without weight-bearing for six weeks. Rehabilitation was prescribed. At a four-month follow-up, the clinical, radiological and functional results were satisfactory. Conclusion: This surgical procedure can be considered in exceptional cases, particularly in patients with short limb segments, with satisfactory clinical and radiologic outcomes at four months of follow-up.
Abbreviation
IMN: Intramedullary Nailing
Introduction
Locked intramedullary nailing (IMN) is currently considered the gold standard for the treatment of tibial shaft fractures [1]. This status has resulted from continuous advancements, beginning with Gerhard Küntscher’s original concept and progressing to the development of modern locking systems, notably driven by the Strasbourg school [2, 3]. Despite technical advancements, mechanical complications such as delayed union or nonunion, displacement, or breakage of the osteosynthesis material may still occur. These complications can lead to residual pain, permanent functional impairment [4], and often require surgical reintervention (in 12% to 60% of cases) [5]. Recently, several studies have reported the possibility of using small-sized locked nails such as the humeral nail for femoral fixation in selected adolescent patients [6]. Regarding fractures of the bones of the lower leg, very few studies have described the use of a locked humeral nail for tibial shaft osteosynthesis [7, 8]. The authors report the exceptional use of a humeral nail due to the intraoperative unavailability of a suitable tibial implant in a patient who also exhibited mild skin compromise contraindicating plate fixation case involving a 57-year-old patient with a short limb segment, who provided informed consent for publication. This case-report was written in accordance with SCARE guidelines [9].
Case Report
The patient was a 57-year-old woman of short stature (1.48 meters, wearing size 32 shoes), with growth abnormalities secondary to childhood poliomyelitis. Her trauma history included a left subtalar arthrodesis performed 34 years earlier for a poliomyelitic foot. She was admitted to the emergency department one hour after sustaining a closed injury to the left lower leg, following an indirect rotational mechanism caused by a ground-level fall.
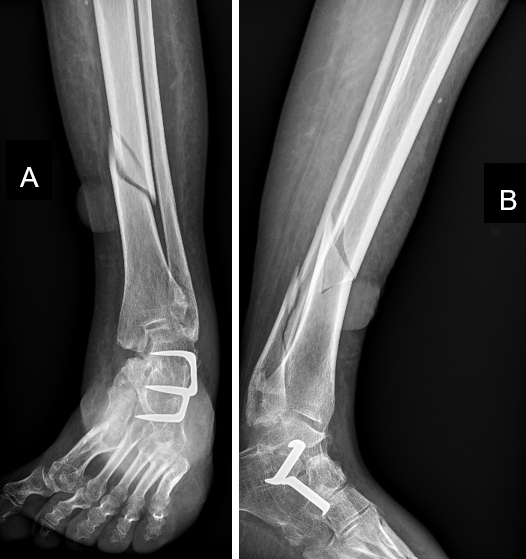
The initial clinical examination revealed a malposition of the lower limb in abduction and external rotation, with the lateral border of the foot resting on the bed and the patella oriented upward. Palpation of the distal third of the leg elicited sharp pain. A 5×5 cm blister was observed on the anteromedial aspect of the leg, indicating evolving skin compromise. Distal toe sensation and motor function were preserved. Distal peripheral pulses were well palpated and regular. The remainder of the examination was normal. Anteroposterior (Figure1A) and lateral (Figure1B) radiographs of the left leg showed a spiral fracture of the distal third of the left tibial diaphysis, with a suprafocal fracture line. It was associated with a supratubercular fracture of the ipsilateral lateral malleolus. The clinical and radiologic assessment indicated a closed fracture of the left leg, classified as AO type 42A1 and Tscherne–Götzen grade 1.
Urgent surgical fixation with a locked intramedullary nail of the left tibia was indicated. The procedure was initially planned using a Depuy Synthes® Expert Tibial Nail, whose proximal lateral curvature facilitates insertion and helps prevent loss of reduction during placement. Because of the compromised skin overlying the fracture site, plate- and-screw fixation was contraindicated due to the risk of skin necrosis.
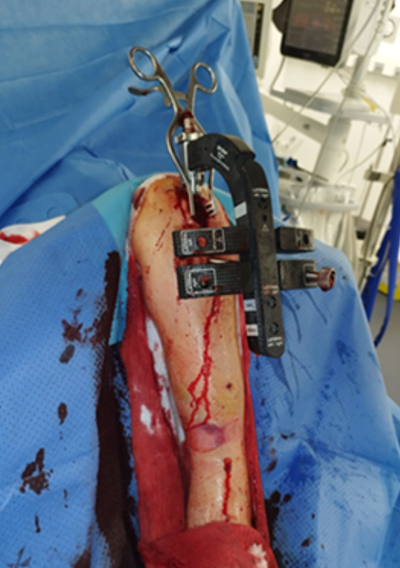
Surgical Procedure
The patient was positioned and operated on a standard table using the conventional technique. After insertion of the reaming guide, the intraoperative measurement of the definitive implant length was 260 mm. However, the locked tibial nails available in the operating room had a minimum length of 285 mm. Given the relatively short tibia and the fact that the patient was already in surgery, a Stryker® T2 humeral nail was chosen (Figure 2). This nail also features a proximal lateral curvature similar to that of the Expert tibial nails. The implant measured 260 mm in length with an 8 mm diameter. It was then proximally locked with two 5 mm diameter screws, measuring 40 mm and 45 mm, respectively, and distally locked with a 4 mm anteroposterior screw, 36 mm in length Figures 3A and 3B. A posterior plaster splint was applied postoperatively, with non-weight-bearing for six weeks. Rehabilitation began on the first postoperative day with maintenance of knee range of motion, isometric contraction exercises, and quadriceps strengthening according to pain tolerance. Staples were removed on postoperative day 15. The patient was then seen in follow- up at six weeks and four months. At six weeks, the leg was painless and the clinical examination was satisfactory. Anteroposterior (Figure4A) and lateral (Figure4B) radiographs showed early callus formation, allowing the resumption of weight-bearing. At four months, clinical progress was satisfactory. Follow-up radiographs confirmed bone consolidation. Gait anteroposterior (Figure5A) and lateral (Figure5B) was normal, and full functional recovery was achieved.
The chronological sequence of events is summarized in Table 1.
| Date/Period | Event | Details |
|---|---|---|
| Day of the trauma | Closed left leg injury | Severe left leg pain associated with complete functional impairment of the left lower limb |
| Same day: one hour after the injury | Physical and radiological examination | Closed leg fracture (42A1 according to the AO classification), with skin damage (Tscherne-Götzen stage 1) |
| Same day: two hours after the injury | Preoperative assessment | Normal |
| Same day: surgery (five hours after the injury) | Tibial locked intramedullary nailing | The definitive implant length measured intraoperatively was 260 mm; however, the shortest tibial nails available in the operating room were 285 mm. |
| Given the patient’s relatively short tibia, the inability to use a screw plate due to compromised skin, and the unavailability of appropriately sized tibial nails, the procedure was performed using a 260 mm humeral nail. | ||
| Postoperative period | Rehabilitation | A posterior plaster splint was applied postoperatively, and the patient remained non-weight-bearing for six weeks. |
| Rehabilitation started on the first postoperative day, focusing on maintaining knee range of motion, performing isometric exercises, and strengthening the quadriceps according to pain tolerance. | ||
| Complete skin healing was observed two weeks after surgery. | ||
| Six weeks post-surgery | Follow-up | Patient painless with satisfactory clinical examination |
| Radiographs showed early callus formation, allowing the resumption of weight-bearing. | ||
| Four months post- surgery | Follow-up | Radiographs confirmed bone consolidation |
| Normal gait and full functional recovery |
Table 1: Timeline of clinical events.



Discussion
As early as 1939, Gerhard Küntscher, considered the father of modern intramedullary nailing, proposed the closed insertion of an antegrade intramedullary rod with the aim of achieving a stable and strong construct that allowed rapid functional recovery, immediate mobilization, and early weight-bearing of the lower limb [10]. The locking concept, developed by the Strasbourg school, improved Küntscher’s original technique by preventing telescoping and rotational instability [11]. Over time, advancements in nail design have made locked intramedullary nailing (IMN) increasingly effective [12].
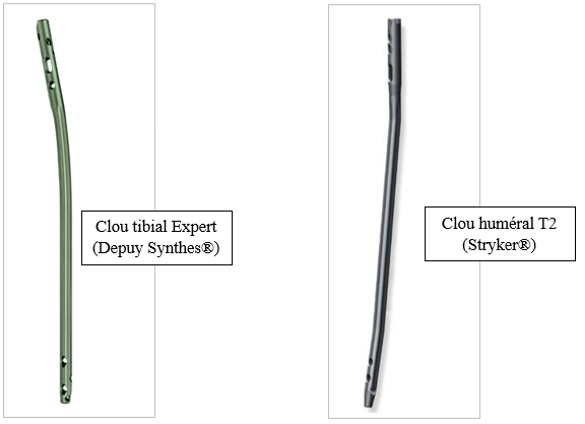
The locked nails available in the operating room included tibial nails (Expert nails from Depuy Synthes®) and humeral nails (T2 nails from Stryker®), all made of Type II anodized titanium alloy (Ti6Al4V). The Expert tibial nail (Figure 6A) also contains 6% aluminum and 7% niobium. Its length ranges theoretically from 255 to 465 mm in 15 mm increments, with a diameter of 8 to 13 mm in 1 mm increments. Nails with diameters of 9 to 13 mm accept 5 mm locking screws, whereas 8 mm nails accept 4 mm distal screws and 5 mm proximal screws.
The Stryker humeral nail, (Figure 6B) in contrast, ranges from 140 to 320 mm in length in 10 mm increments, with a diameter of 7 to 9 mm in 1 mm increments. The lateral curvature of the nails (10° for the tibial nail and 6° for the humeral nail) facilitates insertion, minimizes the risk of loss of reduction during placement, and ensures a more anatomical position within the medullary canal. At the time of the procedure, the available tibial nails ranged from 285 to 420 mm in length, while all sizes of humeral nails were available. However, the intraoperative measurement indicated a required length of 260 mm. In the absence of an appropriately sized tibial nail, the most practical solution during surgery was to use a T2 humeral nail. Very few authors in the literature have reported the potential use of locked humeral nails for the treatment of tibial diaphyseal fractures [7, 8]. One of the advantages of the humeral nail is its availability in smaller diameters and shorter lengths, making it particularly suitable for the tibial anatomy of patients with a narrow medullary canal and a short limb segment [7]. From a biomechanical standpoint, both types of nails are made, among other materials, of Type II anodized titanium (Ti6Al4V), which provides excellent mechanical strength and high biocompatibility. In this clinical case, the clinical, radiologic, and functional outcomes at four months postoperatively were satisfactory.
Conclusion
Locked intramedullary nailing of tibial diaphyseal fractures can, in exceptional cases, be performed using humeral nails, particularly in patients with short limb segments, yielding satisfactory clinical and radiologic outcomes.
Authors Contributions
• Bizolé Balepna DY: conceptualization of the first draft, literature review, case analysis, alignment with the SCARE guidelines and manuscript writing. • Petit H and Handy ED: critical review, final proofreading and overall project supervision. • All authors have read and approved the final manuscript.
Conflict of Interest
The authors declare that no conflicts of interest exist.
Highlights
- This case provides valuable insight into a rare but practical intraoperative solution when the implants typically used for intramedullary nailing of tibial shaft fractures are not available.
- It shares a surgical experience that may help guide other orthopedic surgeons facing similar intraoperative constraints.
References
-
Xia L, Zhou J, Zhang Y, Mei G, Jin D (2014) A meta- analysis of reamed versus unreamed intramedullary nailing for the treatment of closed tibial fractures. Orthopedics 37(4): e332-338.
-
Küntscher BG (1958) The Küntscher method of intramedullary fixation. J Bone Jt Surg Am 40: 17-26.
-
Kempf I, Grosse A, Lafforgue D (1978) L’apport du verrouillage dans l’enclouage centromédullaire des os longs. Rev Chir Orthop 64: 631-651.
-
Duan X, Al‐Qwbani M, Zeng Y, Zhang W, Xiang Z (2012) Intramedullary nailing for tibial shaft fractures in adults. Cochrane Database of Systematic Reviews (1): CD008241.
-
Tay WH, De Steiger R, Richardson M, Gruen R, Balogh ZJ (2014) Health outcomes of delayed union and nonunion of femoral and tibial shaft fractures. Injury 45(10): 1653-1658.
-
Sa-ngasoongsong P, Saisongcroh T, Angsanuntsukh C, Woratanarat P, Mulpruek P (2017) Using humeral nail for surgical reconstruction of femur in adolescents with osteogenesis imperfecta. World J Orthop 8(9): 735-740.
-
Phupate A, Vashishtha A, Kale A, Godse A (2024) Modified Use of Humerus Nail for Management of Tibia Diaphyseal Fracture–Rare Case Report. J Orthop Case Rep 14(9): 152-156.
-
Pradeep H, Pillai AG, Ravikumar AS (2022) Humerus nail for tibial reconstruction in adolescent with osteogenesis imperfecta - A rare surgical case report. Indian J Orthop Surg 8: 236-239.
-
Kerwan A, Al-Jabir A, Mathew G, Sohrabi C, Rashid R, et al. (2025) Revised surgical CAse REport (SCARE) guideline: an update for the age of artificial intelligence. Premier J Sci 10: 100079.
-
Ehlinger M, Adam P, Taglang G, Lefevre C, Bonnomet F (2012) Techniques chirurgicales de l’enclouage centromédullaire des os longs. EMC-Tech Chir Orthop Traumatol 7(4): 1-12.
-
Amossou LF, Goukodadja O, Padonou A, Chigblo P, Djagbé M, et al. (2024) Locked Centromedullary Nailing of the Tibia and Femur Without a Brilliance Amplifier in Benin: A Report of 180 Cases. Health Sci Dis 25(4): 59-63.
-
Inal S, Inal C, Taspinar B (2015) Presentation of a Humeral Shaft Fracture Treated by Locked Intramedullary Nailing With Unlocked Technique. Trauma Mon 20(3): e19452.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results
- Management of Complications from Traditional Treatment of Locomotor System Injuries at the National Hospital of Niamey: A Report of 220 Cases