Smith-Petersen Osteotomy for the Treatment of Anderson Lesion with Kyphosis in Ankylosing Spondylitis:A Case Report and Literature Review
Andersson lesion (AL) is an uncommon manifestation of ankylosing spondylitis (AS) first described by Andersson in 1937. Few data are available on Anderson lesion in AS because of the lack of proper diagnostic criteria and the differences in the extent of spinal survey undertaken. Multiple types of surgery have been applied in the treatment for AL. However, the most effective and safe surgical procedure for AS-related symptomatic kyphosis is still controversial. We reported a case of surgical strategy with Smith-Petersen osteotomy (SPO) for AL-complicating with AS patient presenting severe kyphosis. The patient acquired excellent clinical results and returned to work without any physical complaints. The Smith-Petersen osteotomy (SPO) surgery may offer a useful choice for AL-complicating AS patients with severe kyphosis deformity.
Introduction
Ankylosing spondylitis (AS) is a kind of chronic inflammatory disease which affects spine and sacroiliac joints, causing pain, stiffness and progressive kyphosis [1]. The annulus fibrosus, anterior longitudinal ligament, flaval ligaments and apophyseal joints demonstrate progressive ossification in the later state of the disease [2]. In 1937, Andersson reported the AS patients may occur progressive vertebra and intervertebral disc injury which was known as Andersson lesion (AL) for the first time [3]. The patients diagnosed as AL may lead to kyphotic deformity with serious pain. It is considered that surgical procedure is the principle management in symptomatic AL patients who fail in the conservative treatment. The main purpose of surgical treatment is to decompress the spinal cord and stabilize the spine lead to spinal fusion in the end. However, few literatures have described surgical procedures such as Smith-Petersen osteotomy (SPO) for the AL patients with severe kyphotic deformity [4, 5, 6]. Herein we report the experience of SPO in a case presenting with serious spinal deformity due to AL-complicating AS.
A 30-year-old man with eight-year history of AS presented progressive intermittent thoracolumbar back pain after a minor trauma three months ago. Physical
examination indicated intense back pain and obvious thoracolumbar kyphosis without neurological deficits. Erythrocyte sedimentation rate and C reactive protein were 4mm/hour and 38.07 mg/L respectively. Rheumatoid factors and antibody resistance O were respectively 42.80IU/L and 19.80 IU/L. The result of human leukocyte antigen-27 (HLA-B27) was positive. Blood counts and other serum chemistries were normal.
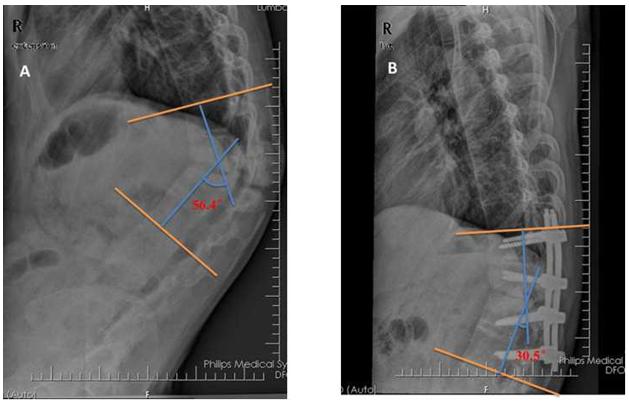
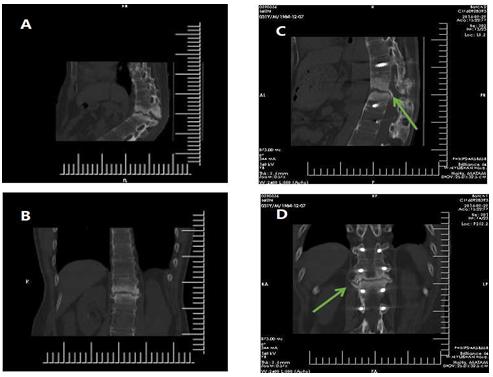
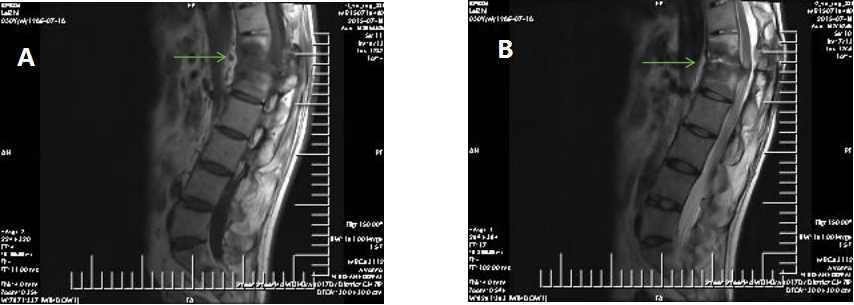
The X-ray of the spine indicated osteoporosis and ankylosing spondylitis (Figure 1A). Computed tomography (CT) showed irregular vertebral or discovertebral osteolysis in T12/L1 with surrounding reactive sclerosis (Figure 2A-B). Slice-like signal intensity with unclear boundary could be seen on T1 and T2- weighted images (Figure 3).
Journal of Orthopedics & Bone Disorders
Given the history of AS, a progressive thoracolumbar kyphosis at the intravertebral pseudarthrosis of T12/L1and the classical radiological appearance, the patient was diagnosed as AL-complicating AS in the end and received Smith-Petersen osteotomy. Under general anesthesia, the patient was given prone position with face and eye protection. Surgical plan included pedicle screw placement from T11 to L2 by freehand technique and T12-L1 spinous process, vertebral plate and little processus articularis removed. All pedicle screws nail were polyaxial pedicle screw in order to avoid nail extracted and broken resulted from the concentration of correction forces. Install the pre-bent titanium rods and rectify kyphosis deformity. The bone segment obtained from the osteotomy site that involved lamina and fused facet joint were cut into pieces and put into intertransverse bone graft bed for intertransverse process fusion. The operation time was 180 min and blood loss was 575cc. The patients had dural tears with cerebrospinal fluid leakage, which was controlled 10 days after surgery. The VAS scores decreased from preoperative 6 to at final follow-up 2. The Cobb’s angle decreased from 56.4 degrees to 30.5 degrees (Figure. 1B). The patient acquired oral medicine treatment under the guidance of department of rheumatology postoperation, with the Oswestry Disability Index (ODI) increasing scores from 42 to 32. The patient used well-molded thoracolumbosacral brace to ensure solid immobilization during the first three months.
Discussion
Anderson lesion is a well-known complication of AS with reported prevalence range from 1.5% to 28% [7]. However, the exact etiology is not yet clear. That’s why many different terms have been used to refer to these lesions such as “discovertebral lesion”, “vertebral lesion”, “destructive vertebral lesion”, “spondylodiscitis” or “discitis” [8, 9]. It is mainly believed that inflammatory and mechanical stress may contribute to the lesions at present [10]. Kabasakal suspected that vertebra and intervertebral discitis is not only the main cause of Andersson lesion which can occur in multiple vertebrae especially involved intervertebral discs but also the special pathological changes resulted from AS inflammatory erosion of the vertebral and intervertebral discs [11]. However, a slight trauma may also lead to Andersson lesion due to vertebral osteoporosis and increased bone fragility of the spine in the late stage of AS [12, 13]. In this study, we believe that trauma is the possible origin of Andersson lesions in consideration of a history of trauma at the time of onset of persistent back pain. Anderson lesion is easily misdiagnosed as spinal tuberculosis in the clinical practice owing to the similar X-
ray and MRI imaging performances [14]. Urmila Dhakad reported a case of Andersson lesion patient who was misdiagnosed as spinal tuberculosis and failed in empirical antituberculous treatment [15]. In terms of clinical symptoms, patients with spinal tuberculosis have low fever, night sweats, fatigue, and loss of appetite, anemia and other systemic tuberculosis poisoning symptoms. Besides, paraspinal or psoas muscle abscess around lesions are usually seen in spinal MRI images of tuberculosis patients, which can be regarded as characteristic feature. In addition, the sagittal CT reconstructed image indicated thoracolumbar fractures which implicated the three columns and resulted in severe pain, instability and kyphotic deformity. To sum up, the pathogenesis and imaging manifestation in this case were in line with AL characteristics instead of spinal tuberculosis. Conservative treatment can be regarded as the first step treatment for Andersson lesion. Non-steroidal anti- inflammatory drugs (NSAIDs) such as celecoxib are usually used in the acute stage of Andersson lesion to control pain. What’s more, plaster immobilization and Halo-jacket immobilization are also efficient especially in mobile cervical and thoracolumbar levels by obtaining stabilization [12]. However, some researchers pointed out that only inflammatory AL has good response to drugs while traumatic AL usually requires surgical intervention because the minimal persistent motion at the Andersson lesion caused by trauma might prevent fracture healing and union without solid fixation [3, 16]. Surgical treatment has been applied in patients with unbearable pain, progression of the symptoms, kyphotic deformity or neurological deficits. Although most researches have reached a consensus that the purpose of the surgery is to achieve a successful arthrodesis of pseudarthrosis and to restore spinal stability [17]. Although different surgical procedures including instrumented and non- instrumented stabilization through anterior, posterior or combined approach have been introduced in previous studies, the optimal surgical procedure is still in debate [18]. Wang [6] randomly divided 8 patients with Anderson lesions associated with ankylosing spondylitis into two groups and received posterior instrumentation with lesion curettage and anterior bone graft and posterior instrumentation without lesion curettage and anterior bone graft respectively. The results showed that there was no evidence of nonunion was observed in any patient at last follow-up which indicated that lesion curettage and anterior bone graft was not necessary for AL patients. However, other study revealed that posterior correction and fixation of the AL by an anterior opening wedge osteotomy may be considered for patients with a progressive thoracolumbar kyphotic deformity [17]. Zhang advocated transpedicular subtraction and disc resection osteotomy for kyphotic correction and achieved satisfactory clinical results [5]. In this report, the patient received SPO, posterior instrumentation and posterolateral autograft. Although without anterior lesion curettage and bone graft, the sagittal reconstructed CT images of 14 months after the surgery revealed consecutive callus formation as well. It was believed that solid immobilization achieved by posterior instrumentation should be the key point of the treatment of Anderson lesions with ankylosing spondylitis. Comparing to additional anterior lesion curettage and bone graft, the SPO significantly improved surgical results with less blood loss, shorter operation time and fewer postoperative complications.
Conclusion
In summary, it is suggested that SPO could achieve satisfactory kyphosis correction, good fusion and favorable clinical outcomes with less blood loss and fewer postoperative complications, implying a safe and feasible option for treatment for AL-complicating with AS patients with severe kyphosis deformity.
Disclosure of interest
The authors declare that they have no competing interest.
Reference
1. Qian B P, Qiu Y, Wang B, Xu Sun, Ze-zhang Zhu, et al.
(2012) Pedicle subtraction osteotomy through pseudarthrosis to correct thoracolumbar kyphotic deformity in advanced ankylosing spondylitis.. European Spine Journal 21(4): 711-718.
2. Royen B J V, Dijkmans B A C (1978) Ankylosing
Spondylitis Diagnosis and Management. Lancet 1(8059): 339-340.
| Andersson O (1937) Röntgenbilden vid | |
|---|---|
| spondylarthritis ankylopoetica. Nord Med Tidskr 14: | |
| 2000-2002. |
4. Fang D, Leong JC, Ho EK, FL Chan, SP Chow (1988)
Spinal pseudarthrosis in ankylosing spondylitis. Clinicopathological correlation and the results of anterior spinal fusion. Journal of Bone & Joint Surgery British Volume 70(3): 679-688.
5. Zhang X, Yao W, Bing W, Hu W, Zhang Z, et al. (2016)
Treatment of Andersson lesion-complicating ankylosing spondylitis via transpedicular subtraction and disc resection osteotomy, a retrospective study. European Spine Journal 25(8): 2587-2595.
6. Wang G, Sun J, Jiang Z, Cui X (2011) The surgical treatment of Andersson lesions associated with ankylosing spondylitis. Orthopedics 34(7): e302-e306.
7. Kabasakal Y, Garrett S L, Calin A (1996) The
epidemiology of spondylodiscitis in ankylosing spondylitis-a controlled study. British Journal of Rheumatology 35(7): 660-663.
8. Chan F L, Ho E K, Fang D, Hsu LCS, Leong JCY, et al.
(1987) Spinal pseudarthrosis in ankylosing spondylitis. Acta Radiologica: Diagnosis 28(4): 383- 388.
9. Langlois S, Cedoz J P, Lohse A, Toussirot E, Wendlig D
(2005) Aseptic discitis in patients with ankylosing spondylitis: a retrospective study of 14 cases. Joint Bone Spine Revue Du Rhumatisme 72(3): 248-253.
10. Bron J L, Vries M K D, Snieders M N, Irene E van der Horst-Bruinsma, Barend J van Royen (2009) Discovertebral (Andersson) lesions of the spine in ankylosing spondylitis revisited. Clinical Rheumatology 28(8): 883-892.
11. Kabasakal Y, Garrett S L, Calin A (1996) The
epidemiology of spondylodiscitis in ankylosing spondylitis-a controlled study. British Journal of Rheumatology 35(7): 660-663.
12. Hitchon PW, From AM, Brenton MD, John A Glaser,
James C Torner (2002) Fractures of the thoracolumbar spine complicating ankylosing spondylitis. Journal of Neurosurgery 97(97): 218-222.
13. Geusens P, Vosse D, Van d L S. (2013) Osteoporosis
and vertebral fractures in ankylosing spondylitis. Current Opinion in Rheumatology, 19(4): 335-339.
14. Dave BR, Ram H, Krishnan A (2011) Andersson lesion:
Are we misdiagnosing it? A retrospective study of clinico-radiological features and outcome of short segment fixation. European Spine Journal, 20(9): 1503-1509.
15. Dhakad U, Das SK (2013) Andersson lesion in ankylosing spondylitis. Bmj Case Reports 2013(2013): 1357-1357.
16. Chang KW, Tu MY, Huang HH, Chen HC, Chen YY, Lin
CC (2006) Posterior correction and fixation without anterior fusion for pseudoarthrosis with kyphotic deformity in ankylosing spondylitis. Spine 31(13): E408-E413.
17. Kim KT, Lee SH, Suk KS, Lee JH, Im YJ (2007) Spinal
pseudarthrosis in advanced ankylosing spondylitis with sagittal plane deformity: clinical characteristics and outcome analysis Spine 32(15): 1641-1647.
18. Fox M W, Onofrio B M, Kilgore J E (1993) Neurological
complications of ankylosing spondylitis. Journal of Neurosurgery 78(6): 871-878.
References
-
Qian B P, Qiu Y, Wang B, Xu Sun, Ze-zhang Zhu, et al. (2012) Pedicle subtraction osteotomy through pseudarthrosis to correct thoracolumbar kyphotic deformity in advanced ankylosing spondylitis.. European Spine Journal 21(4): 711-718.
-
Royen B J V, Dijkmans B A C (1978) Ankylosing Spondylitis Diagnosis and Management. Lancet 1(8059): 339-340. [INLINE_TABLE:3:0]
-
Fang D, Leong JC, Ho EK, FL Chan, SP Chow (1988) Spinal pseudarthrosis in ankylosing spondylitis. Clinicopathological correlation and the results of anterior spinal fusion. Journal of Bone & Joint Surgery British Volume 70(3): 679-688.
-
Zhang X, Yao W, Bing W, Hu W, Zhang Z, et al. (2016) Treatment of Andersson lesion-complicating ankylosing spondylitis via transpedicular subtraction and disc resection osteotomy, a retrospective study. European Spine Journal 25(8): 2587-2595.
-
Wang G, Sun J, Jiang Z, Cui X (2011) The surgical treatment of Andersson lesions associated with ankylosing spondylitis. Orthopedics 34(7): e302-e306.
-
Kabasakal Y, Garrett S L, Calin A (1996) The epidemiology of spondylodiscitis in ankylosing spondylitis-a controlled study. British Journal of Rheumatology 35(7): 660-663.
-
Chan F L, Ho E K, Fang D, Hsu LCS, Leong JCY, et al. (1987) Spinal pseudarthrosis in ankylosing spondylitis. Acta Radiologica: Diagnosis 28(4): 383- 388.
-
Langlois S, Cedoz J P, Lohse A, Toussirot E, Wendlig D (2005) Aseptic discitis in patients with ankylosing spondylitis: a retrospective study of 14 cases. Joint Bone Spine Revue Du Rhumatisme 72(3): 248-253.
-
Bron J L, Vries M K D, Snieders M N, Irene E van der Horst-Bruinsma, Barend J van Royen (2009) Discovertebral (Andersson) lesions of the spine in ankylosing spondylitis revisited. Clinical Rheumatology 28(8): 883-892.
-
Kabasakal Y, Garrett S L, Calin A (1996) The epidemiology of spondylodiscitis in ankylosing spondylitis-a controlled study. British Journal of Rheumatology 35(7): 660-663.
-
Hitchon PW, From AM, Brenton MD, John A Glaser, James C Torner (2002) Fractures of the thoracolumbar spine complicating ankylosing spondylitis. Journal of Neurosurgery 97(97): 218-222.
-
Geusens P, Vosse D, Van d L S. (2013) Osteoporosis and vertebral fractures in ankylosing spondylitis. Current Opinion in Rheumatology, 19(4): 335-339.
-
Dave BR, Ram H, Krishnan A (2011) Andersson lesion: Are we misdiagnosing it? A retrospective study of clinico-radiological features and outcome of short segment fixation. European Spine Journal, 20(9): 1503-1509.
-
Dhakad U, Das SK (2013) Andersson lesion in ankylosing spondylitis. Bmj Case Reports 2013(2013): 1357-1357.
-
Chang KW, Tu MY, Huang HH, Chen HC, Chen YY, Lin CC (2006) Posterior correction and fixation without anterior fusion for pseudoarthrosis with kyphotic deformity in ankylosing spondylitis. Spine 31(13): E408-E413.
-
Kim KT, Lee SH, Suk KS, Lee JH, Im YJ (2007) Spinal pseudarthrosis in advanced ankylosing spondylitis with sagittal plane deformity: clinical characteristics and outcome analysis Spine 32(15): 1641-1647.
-
Fox M W, Onofrio B M, Kilgore J E (1993) Neurological complications of ankylosing spondylitis. Journal of Neurosurgery 78(6): 871-878.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results