Bilateral Ischiofemoral Impingement: A Case Report and Literature Review
Background: Ischiofemoral Impingement (IFI) is rare disease and more common in females than in males. It is characterized by hip and groin pain with abnormalities of the quadratus femoris muscle. The narrowing of ischiofemoral space (IFS) and quadratus femrois space (QFS) are the main causes. It is easy to be missed diagnosis in daily clinical works. Case Report: We report the case of a 16 years old girl without trauma, pain in the right hip region only under loading. In MRI there exist an obvious narrowing IFS and QFS with edema in quadratus femoris muscle. The measurement of the neck-shaft angles is also greater than normal. Conclusions: IFS should be paid more attention when the hip or groin pain occurred. MRI is the best methods for the diagnosis of the IFI. The main treatments include conservative treatment, operation treatment and steroid injection but no ideal one. Further study should be taken to find a better treatment of IFI.
Introduction
Ischiofemoral Impingement (IFI) is rare disease and more common in females than in males. It is characterized by hip and groin pain with abnormalities of the quadratus femoris muscle. Slow onset of the disease and normally without a history of trauma. The narrowing of ischiofemoral space (IFS) and quadratus femrois space (QFS) are the main causes. It is easy to be missed diagnosis in daily clinical works. IFI was first reported by Johnson in 1977 [1]. A clear definition about Ichiofemoral Impingement (IFI) Syndrome was given by Torriani in 2009 [2]. The narrowing of ischiofemoral space (IFS) and quadratus femrois space (QFS) in MRI can be diagnosed as ischiofemoral impingement syndrome.
Case presentation
We report the case of a 16years old girl without trauma, activity football player. The pain about the right hip region continues for 4-5 weeks only under loading without nocturnal pain and rest pain. Since 1 week ago, there is a limitation of motion in football training, appeared 3 times. The physical examination: The patient is in normal gait with slightly limping. The level of pelvic is normal. Lower extremity ante torsion is 15° in both sides. External rotation is 20°. The movement of hips is normal. The treatment included physiotherapy, rest, stopping playing football and 6 weeks following up.
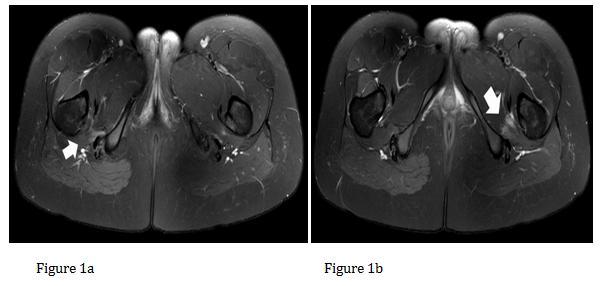
In MRI there exist obvious narrowing IFS and QFS with edema in bilateral quadratus femoris muscle (Table 1, Figure 1 a-b, Figure 2 a-d). The IFS are 23.38 mm on the left side and 20.53 mm on the right side. Results of QFS are 11.40 mm on the left side and 10.07 mm on the right side. The coxavalga is evaluated by neck-shaft angle. The measurement of the neck-shaft angles is also greater than normal, the neck-shaft angles are 144.11° on the left and 144.40° on the right side respectively (Table 1, Figure 3 a- b). Bilateral ischiofemoral impingement was diagnosed on that basis.
| IFS (mm) | QFS (mm) | Neck-shaft angle (°) | |
| Left | 23.38 | 11.40 | 144.11 |
| Right | 20.53 | 10.07 | 144.60 |
Table 1: The measurement results about IFS, QFS and Neck-shaft angle.
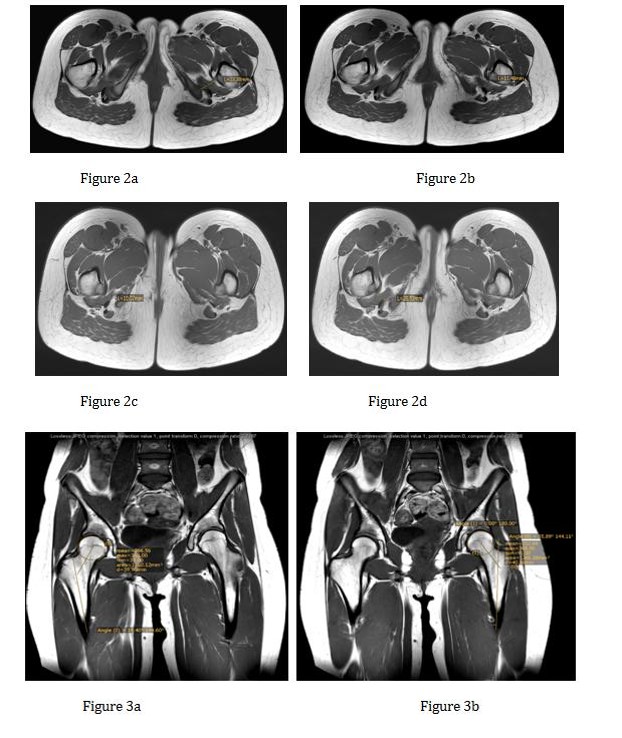
Figure 2 a-d: The measurement of the IFS and QFS in bilateral. (Measured in mm). a. QFS on the left side; b. IFS on the left side; c. QFS on right side; d IFS on right side.
Figure 3 a-b: The measurement of the Neck-shaft angels. (Measured in mm) a. Right side results of Neck-shaft angles. b. Left side results of Neck-shaft angles.
Discussion
IFI was first reported by Johnson in 1977 [1]. He reported 3 patients with continuous pain after the hip operations. The x-ray showed that the distance between ischial tuberosity and the femoral lesser trochanter was obviously narrowed due to the hip operations. After the femoral lesser trochanter resection of these three patients, the pain was completely relief. Thus we recognized that the abnormal impingement between ischial tuberosity and the femoral lesser trochanter may cause the hip pain. A clear definition about Ichiofemoral Impingement (IFI) Syndrome was given by Torriani in 2009 [2]. The narrowing of ischiofemoral space (IFS) and quadratus femrois space (QFS) in MRI can be diagnosed as ischiofemoral impingement syndrome. The quadratus femoris muscleis a falt, quadrilateral skeletal muscle. It is a strong external rotator and adductor of the thigh, and also acts to stabilize the femoral head in the acetabulum [3]. It is located on the posterior side of the hip joint, between the ischiofemoral spaces. Normally the space between ischial tuberosity and the femoral lesser trochanter is enough, when the narrowing of ischiofemoral space occurred; the quadratusfemoris would experience a repeated friction by ischial tuberosity and the femoral lesser trochanter and get injured. The normal distance between ischial tuberosity and the femoral lesser trochanter is approximately 20mm [1]. In order to evaluated the space between ischial tuberosity and the femoral lesser trochanter more accurately. We need to measure the IFS (Ischiofemoral Space) and QFS (quradratus femoris space) [2, 4, 5, 6, 7]. There are many research focuses on their point to the IFS and QFS measurement. A meta-analysis with 217 IFI shows that cases of IFI showed significantly smaller IFS and QFS compared to controls (14.91 ± 4.8 versus26.01 ± 7.98 and 9.57 ± 3.7 versus 15.97 ± 6.07, respectively) [8]. In our study, the IFS are 23.38 mm on the left side and 20.53 mm in the right side. And the QFS is11.40 mm on the left side and 10.07 mm on the right side Coxavalga is considered play an important role in IFI, especially in adolescent case [9]. The femoral neck inclination (femoral neck-shaft angle) is also known as Center-Collum-Diaphysis angle (CCD angle), it is greater in newborns (approximately 150°) and smaller in adulthood (approximately 120°) [10]. Normally in 15 years old, the neck-shaft angle is nearly 130°. In our case, the neck-shaft angles are 144.11° on the left and 144.40° on the right side. A higher prevalence of extra-articular impingement has been found for coxavalga. Patients with IFI show increased femoral neck-shaft angle compared with controls, suggesting that increased femoral neck- shaft angle may lead to the narrowing of the IFS [9, 11, 12, 13]. MRI now is the best methods for the diagnosis of the IFS. In the recent researches, the ultrasound has been proved to have the similar measurements results with MRI [14]. And ultrasound-guided injections can also relief the pain of hip [15]. However, the MRI findings of IFI not only include a narrowed space between the lesser trochanter of the femur and the ischial tuberosity but also the edema or atrophy in the quadratus femoris muscle. The most important is that we can evaluate the whole hip joint and given a clearness result. The main causes for the narrowing of the ischiofemoral space are postural, congenital and acquired reason. Postural reason means when patient in a position like internal/extort rotation, adduction/ abduction and flexion/ extension, the different position will cause the narrowing of the IFS [2, 11]. Compared to male, the anatomy structure of the female pelvis has a longer transverse diameter, a shorter anteroposterior diameter and a wider ischial tuberosity, so the IFS is smaller and with less tolerance for further narrowing [16]. The acquired reason are common in operation which can influence the femoral lesser trochanter, serious osteoarthritis of the hip and tumor [1, 5, 6, 17]. For the treatment of the IFI, there was also lack of efficient treatment. According to the symptom of the patient we can choice conservative treatment or operation treatment. CT-guided/Ultrasound-guided steroid injection was also mentioned in some reports. The conservative treatment included rest, physiotherapy, NSAIDs, and limitation the activity of the patient [17, 18], and normal used in the mild case. For this patient, our treatment included physiotherapy, rest, stopping playing football and 6 weeks following up. The operation treatment included opening operation and arthroscopy operation. The main aim is to get more space between ischium and the femur through the resection of femoral lesser trochanter. But the operation will cause the hip flexor weakness and the relevant operation complication [4, 16, 19]. New researches of treatments focus more on the temporary relief of the pain.
For example, CT-guided steroid and local anesthetic injection around the quadratus femoris can relief the pain temporary [16], but was not recommended as a first choice. Ultrasound-guided corticosteroid injection of the quadratus femoris muscle cans also relief the pain of the hip. However, the long term following up is also needed [15]. Other new treatment like prolotherapy with polyeoxy ribonucleotide are also reported useful, but also lack long term following up and repeatability [20].
Conclusion
IFS should be paid more attention when the hip or groin pain occurred. MRI is the best methods for the diagnosis of the IFI. The main treatments include conservative treatment, operation treatment and steroid injection but no ideal one. Further study should be taken to find a better treatment of IFI.
References
-
Johnson K (1977) Impingement of the lesser trochanter on the ischial ramus after total hip arthroplasty. Report of three cases. JBJS 59(2): 268- 269.
-
Torriani M, Souto SC, Thomas BJ, Ouellette H, Bredella MA (2009) Ischiofemoral impingement syndrome: an entity with hip pain and abnormalities of the quadratus femoris muscle. AJR American journal of roentgenology 193(1): 186-190.
-
Kahle W, Leonhardt H, Platzer W, Palmer E, Platzer W (2004) Color atlas and textbook of human anatomy. Vol. 1, Locomotor system: Thieme.
-
Hatem MA, Palmer IJ, Martin HD (2015) Diagnosis and 2-year outcomes of endoscopic treatment for ischiofemoral impingement. Arthroscopy: The Journal of Arthroscopic & Related Surgery 31(2): 239-246.
-
Schatteman J, Vanhoenacker F, Somville J, Verstraete K (2015) Ischiofemoral impingement due to a solitary exostosis. Journal of the Belgian Society of Radiology 98(1): 39-42.
-
Papoutsi D, Daniels J, Mistry A, Chandraseker C (2016) Ischiofemoral impingement due to a lipoma of the ischiofemoral space. BMJ case reports 2016: bcr2015213210.
-
Palczewski P, Sułkowska K, Świątkowski J, Kocoń H, Gołębiowski M (2015) Ischiofemoral impingement syndrome: a case report and a review of literature. Polish journal of radiology. 80: 496-498.
-
Singer AD, Subhawong TK, Jose J, Tresley J, Clifford PD (2015) Ischiofemoral impingement syndrome: a meta-analysis. Skeletal radiology 44(6): 831-837.
-
Stenhouse G, Kaiser S, Kelley SP, Stimec J (2016) Ischiofemoral Impingement in Children: Imaging With Clinical Correlation. AJR American journal of roentgenology 206(2): 426-430.
-
Gujar SM, Vikani S, Parmar J, Bondre K (2013) A correlation between femoral neck shaft angle to femoral neck length. International Journal of Biomedical and Advance Research 4(5): 295-298.
-
Tosun O, Algin O, Yalcin N, Cay N, Ocakoglu G, et al. (2012) Ischiofemoral impingement: evaluation with new MRI parameters and assessment of their reliability. Skeletal radiology 41(5): 575-587.
-
Bredella MA, Azevedo DC, Oliveira AL, Simeone FJ, Chang CY, et al. (2015) Pelvic morphology in ischiofemoral impingement. Skeletal radiology 44(2): 249-253.
-
Hernando MF, Cerezal L, Perez-Carro L, Canga A, Gonzalez RP (2016) Evaluation and management of ischiofemoral impingement: a pathophysiologic, radiologic, and therapeutic approach to a complex diagnosis. Skeletal radiology 45(6): 771-787.
-
Finnoff JT, Johnson AC, Hollman JH (2016) Can Ultrasound Accurately Assess Ischiofemoral Space Dimensions? A Validation Study. PM&R 9(4): 392- 397.
-
Backer MW, Lee KS, Blankenbaker DG, Kijowski R, Keene JS (2014) Correlation of ultrasound-guided corticosteroid injection of the quadratus femoris with MRI findings of ischiofemoral impingement. American Journal of Roentgenology 203(3): 589-593.
-
Ali AM, Whitwell D, Ostlere SJ (2011) Case report: imaging and surgical treatment of a snapping hip due to ischiofemoral impingement. Skeletal radiology 40(5): 653-656.
-
Patti JW, Ouellette H, Bredella MA, Torriani M (2008) Impingement of lesser trochanter on ischium as a potential cause for hip pain. Skeletal radiology 37(10): 939-941.
-
Tosun O, Çay N, Bozkurt M, Arslan H (2012) Ischiofemoral impingement in an 11-year-old girl. Diagn Interv Radiol 18(6): 571-573.
-
Safran M, Ryu J (2014) Ischiofemoral impingement of the hip: a novel approach to treatment. Knee Surgery, Sports Traumatology, Arthroscopy 22(4): 781-785.
-
Kim WJ, Shin HY, Koo GH, Park HG, Ha YC, et al. (2014) Ultrasound‐guided Prolotherapy with Polydeoxyribonucleotide Sodium in Ischiofemoral Impingement Syndrome. Pain Practice. 14(7): 649- 655.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results