Monteggia Equivalents: Report of a New Variant of Type I- Salter Harris Type One Injury to Proximal Radius Physis and Olecronon Fracture
Introduction: Monteggia fracture dislocation in a child is relatively uncommon injury consisting approximately 1.5%–3% of the elbow injuries in the childhood. Case Presentation: A unique case of a type 1 Monteggia fracture equivalent Fracture of olecronon with Salter-Harris type I physeal injury to proximal radius physis with in a child is reported. We describe the management of this unique fracture and discuss mechanism of injury. Conclusion: This case is a rare combination of injuries. Early recognition and prompt surgical intervention can lead to a satisfactory outcome even in these complex injuries. Fracture of olecronon with Salter-Harris type I physeal injury to proximal radius physis should be included in the current type I Monteggia equivalents. Key Message: The universal principle of examining one joint above and below and including both joints when taking radiographs for suspected long bone fractures must always be followed.
Introduction
While fractures of the distal forearm are quite common in children, the Monteggia lesion remains uncommon. Monteggia fracture dislocations have been complex injuries in the terms of diagnosis, mechanism of injury, treatment and its outcome. Its first description dates back to 1814, when Giovanni Battista Monteggia first observed this entity [1]. Shortly before his death, he has written [2]. “…I unhappily remember the case of a girl who seemed to me to have sustained a fracture of the upper third of the ulna. At the end of a month of bandaging, the head of the radius dislocated when I extended the forearm. I applied a new bandage but the head of the radius would not stay in place…” Bado described ‘true Monteggia lesions’ and classified them into four types [3]. He also classified certain injuries as equivalents to the ‘true Monteggia lesions’ based on their similar radiographic pattern and biomechanism of injury and ‘Monteggia equivalent’ term was used for these patterns. Since then various types and their equivalents have been described in the literature. A unique case of a type 1 Monteggia fracture equivalent Fracture of olecronon with Salter-Harris type I physeal injury to proximal radius physis with in a child is reported. To the best of our knowledge, there have been no reports in the literature of cases with exactly the same combination of injuries.
Case Report
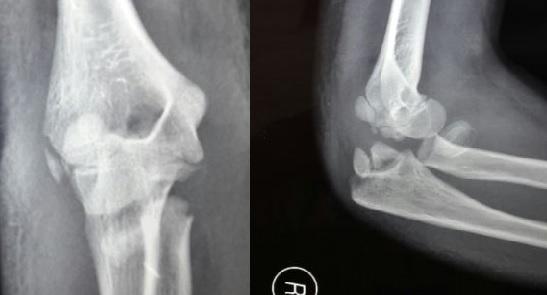
A 12-year-old female sustained a fall from a height of about 4 ft and landed on his outstretched left hand and sustained an injury to the left elbow. He presented to the emergency department approximately 12 hours after sustaining the injury with complaints of swelling, severe pain and restricted motion of left elbow joint. On examination, his vitals were stable and no neurological or vascular deficits were noted. Left elbow displayed gross swelling and deformity. Painful abnormal mobility and crepitus was present elbow. Soft tissue cover was intact. There was no distal neurovascular deficit. Roentgenograms showed a fracture of olecronon with proximal radial type 1 physeal injury with posterior displacement of distal fragments. (Figures 1A and 1B ). The patient was treated with open reduction and internal fixation. Under general anesthesia and in lateral position elbow was exposed by posterior approach. After direct reduction radial physis fracture was stabilized by using 2 mm smooth capitulo-radial kirshner wire and olecronon by tension band wiring using two 1.5 mm smooth kirshner wire and tension bad wire. Postoperatively salb applied for 15 day. After stich removal on 15 day above elbow cast was applied. Both the fractures healed at 6 weeks and here gained the full range of flexion, extension, and supination pronation with bony union at 6 months following physiotherapy. A written informed consent was obtained authorizing treatment, radiological examination and photographic documentation.
Discussion
Monteggia fracture dislocation in child is uncommon injury [3] consisting approximately 1.5%–3% of the elbow injuries in childhood. A unique case of a type IV Monteggia fracture equivalent Fracture of olecronon with Salter-Harris type I physeal injury to proximal radius physis with in a child is reported. We describe the management of this unique fracture and discuss the possible mechanism of injury. Previously reported cases includes type III Monteggia injury with ipsilateral distal radius and ulna fractures [4]; olecranon fracture and distal radial epiphysis [5]; type II Monteggia fracture with fracture separation of the distal radial physis [6]; type IV Monteggia injury with distal diaphyseal fracture of the radius [7]; 11 cases of Monteggia fracture dislocation with fracture of the ipsilateral radius and ulna [8]; three epiphyseal fractures (distal radius and ulna and proximal radius) and a diaphyseal ulnar fracture in the same forearm [9, 10, 11, 12]. Asheesh Sood et al. [13] reported a case with complete fracture of the olecran on with a fracture of the radial neck, and a Salter-Harris type II fracture of the distal radius and ulna with complete displacement [3]. With extensive review of literature our case was found unique and unreported. Properly assessing the nature of this injury in a timely fashion is imperative in order to prevent permanent disability or limb dysfunction [2, 14, 15, 16]. It is usually very difficult to determine the exact mechanism of injury in a very young child, who is usually not able to provide precise details of the sequence of injury [10]. However, the position of the forearm when the child is first presents, the position of the distal radius on radiograph, the direction of dislocation of radial head, and the direction of angulation of ulnar fracture, provide indirect clues about mechanism of injury [17]. The most widely accepted theories are that isolated Monteggia fracture dislocation is caused by hyperpronation described by Evans [18]. However, According to Tompkins theory hyperextension of the elbow plays significant role in causing this injury [19]. In our case, probably both of these indirect mechanisms, hyperextension as well hyperpronation, were involved considering the facts that there was presence of anterior angulation in olecronon fracture and forearm was in attitude of pronation when patient presented to us. The patient having suffered a fall on the outstretched hand, in apposition of hyper pronation on impact, it seems logical to believe that the load transmission from distal to proximal and from radius to ulna resulted initially in distal radius physeal injury and distal the ulnar fracture. The continuing hyperextension force across the interosseous membrane which usually resulted in ulna fracture at junction of proximal third to middle third and type 2 radial physeal lesion [20, 21]. The excessive forces acting in and around a joint may result in capsulo-ligamentous or bony failure. Instead of anterior dislocation of radial head or the radial neck fracture, there is type 1 physeal injury to proximal radius with anterior angulation of radius (Figures 2 & 3).

![Figure 3: Post Operative Xray. Essentially, Monteggia the lesion consists of dislocation of the head of the radius with a fracture of ulnaat various levels. Bado, in series of 40 patients, described 4 patterns and classified them according to direction of dislocation of the radial head [3]. He suggested that these injury types should be referred to as “Monteggia lesions” [3,4] (Table 1).](/fulltextimages/897/fig_3.jpeg)
Figure 3: Post Operative Xray. Essentially, Monteggia the lesion consists of dislocation of the head of the radius with a fracture of ulnaat various levels. Bado, in series of 40 patients, described 4 patterns and classified them according to direction of dislocation of the radial head [3]. He suggested that these injury types should be referred to as “Monteggia lesions” [3, 4] (Table 1).
| Ulna fracture | Mechanism of injury | Incidence | |
|---|---|---|---|
| Type I Anterior | Anterior angulation, usually midshaft | Hyperextension, Hyperpronation, Direct blow (?) | ~70% |
| Type II Posterior | Posterior angulation, diaphyseal or metaphyseal | Hyper flexion | ~3%–5% |
| Type III Lateral or anterolateral | Lateral angulation, Metaphyseal, usually greenstick | Hyperextension, Lateral varus stress | ~23%–26% |
| Type IV Anterior, with fracture radius shaft at same level or distal to ulna fracture | Diaphyseal | Hyperpronation | <1% |
Table 1: Various Monteggia lesions and proposed mechanism of injury.
Table 1: Various Monteggia lesions and proposed mechanism of injury. Bado also supplemented his classification to accommodate some unusual varieties, ‘Monteggia like lesions’ [3]. He described three equivalents (all type I equivalents), which included(1) isolated radial head dislocation (with plastic deformation of ulna), (2) fracture of proximal ulna with fracture of the radial neck and (3) both-bone proximal third fractures with the radial fracture more proximal than the ulnar fracture [5] (Table 2).
Our patient sustained hyperextension and hyperpronation injury resulting in fracture of olecronon with Salter-Harris type I physeal injury to proximal radius physis. Considering this Fracture of olecronon with Salter- Harris type I physeal injury to proximal radius physis should be included in current ‘equivalents’or ‘Monteggia like lesions’.
- • Isolated anterior dislocation of radial head (with plastic deformation of
- • Pulled elbow syndrome
- • Fracture of the ulnar diaphysis with fracture of radial neck
- • Fractures of both bones in forearm (wherein, the radial fracture is above
- Type I [11] the junction of the proximal and the middle third)
- • Fracture of ulnar diaphysis with anterior dislocation of radial head and an olecranon fracture
- • Fracture of ulnar diaphysis (at proximal and middle third junction) with proximal radius
- Type II
- Monteggia equivalent :Posterior elbow dislocation in children
- Monteggia equivalent [11, 21]:
- Oblique fracture of ulna (with varus mal alignment) with displaced fracture
- Type III
- Monteggia equivalent [11, 12]:
- Distal humerus fracture with proximal third ulnar diaphysis fracture and distal radial metaphyseal fracture with anterior dislocation of radial head
- Type IV
Table 2: Various fracture pattern under “Monteggia equivalents”
displaced extension type supracondylar fracture of humerus? Fracture of olecronon with Salter-Harris type I physeal injury to
- • Isolated anterior dislocation of radial head (with plastic deformation of
- • Pulled elbow syndrome
- • Fracture of the ulnar diaphysis with fracture of radial neck
- • Fractures of both bones in forearm (wherein, the radial fracture is above
- Type I [11] the junction of the proximal and the middle third)
- • Fracture of ulnar diaphysis with anterior dislocation of radial head and an olecranon fracture
- • Fracture of ulnar diaphysis (at proximal and middle third junction) with proximal radius
- Type II
- Monteggia equivalent :Posterior elbow dislocation in children
- Monteggia equivalent [11, 21]:
- Oblique fracture of ulna (with varus mal alignment) with displaced fracture
- Type III
- Monteggia equivalent [11, 12]:
- Distal humerus fracture with proximal third ulnar diaphysis fracture and distal radial metaphyseal fracture with anterior dislocation of radial head
- Type IV
Table 2: Various fracture pattern under “Monteggia equivalents”
Conclusions
Our case report has highlighted a rare combination of injuries. While it is true that such injuries occur rarely, one must always rule out associated wrist injuries while dealing with elbow trauma. Thorough clinical and radiological examination is the key to avoid missing such injuries. We would like to emphasise that the mechanism of injury needs to be taken into consideration at all times. The universal principle of examining one joint above and below and including both joints when taking radiographs for suspected long bone fractures must not be forgotten. Fracture of olecronon with Salter-Harris type I physeal injury to proximal radius physis should be included in current ‘equivalents’or ‘Monteggia like lesions’.
References
-
Peltier LF (1957) Eponymic fractures: Giovanni Battista Monteggia and Monteggia’s fracture. Surgery 42(3): 585-591.
-
Monteggia GB (1814) Instituzioni chirurgiche Milan Maspero 5: 130.
-
Bado JL (1967) The Monteggia lesion. Clin Orthop Relat Res 50: 71-86. of the lateral condyle of humerus
-
Sinha S, Chang WR, Campbell AC, Hussein SM (2003) Type III Monteggiainjury with ipsilateral distal radius and ulna fracture. The Internet Journal of Orthopaedic Surgery 1(2).
-
Papavasiliou H, Neuropoulos B (1993) Ipsilateral injuries of the elbow and forearm in children. J Pediatr Orthop 6(1): 58-60.
-
Kristiansen B, Erikson AF (1986) Simultaneous type II Monteggia lesion and fracture separation of the lower radial epiphysis. Injury 17: 51-52.
-
Rodgers WB, Smith B (1993) A type IV Monteggia injury with a distal diaphyseal radius fracture in a child. J Orthop Trauma 7(1): 84-86.
-
Theodorou SD, Ierodiaconou MN, Roussis N (1988) Fracture of the upper end of the ulna associated with dislocation of the head of the radius in children. Clin Orthop Relat Res 228: 240-249.
-
Osada D, Tamai K, Kuramochi T (2001) Three epiphyseal fractures (distal radius and ulna and proximal radius) and a diaphyseal ulnar fracture in a seven-year-old child's forearm. J Orthop Trauma 15(3): 375-377.
-
Blasier R (1995) Ipsilateral radial head dislocation and distal forearm fractures of both forearm bones in a child. Am J Orthop 24(6): 498-500.
-
de la Garza JF(2006) Monteggia fracture-dislocation in children. In: Beaty JH, Kasser JR (Eds.) Rockwood and Wilkin’s Fracturesin Children 6th (Edn.) Lippincott Williams & Wilkins, Philadelphia, pp: 491- 528.
-
Arazi M, Ogun TC, Kapicioğlu MI (1999) The Monteggia lesionand ipsilateral supracondylar humerus and distal radius fractures. J Orthop Trauma 13: 60-66.
-
Asheesh S, Osman K, Tajesh B (2008) Simultaneous Monteggia type I fracture equivalent with ipsilateral fracture of the distal radius and ulna in a child: a case report. Journal of Medical Case Reports 2: 190.
-
Beutel BG (2012) Monteggia fractures in pediatric and adult populations. Orthopedics 35(2): 138-44.
-
Wiley JJ, Galey JP (1985) Monteggia injuries in children. J BoneJoint Surg Br 67(5): 728-731.
-
Bhandari N, Jindal P (1996) Monteggia lesions in a child: variant of a Bado type-IV lesion. A case report. J Bone Jt Surg Am 78(8): 1252-1255.
-
Evans EM (1949) Pronation injuries of the forearm with special reference to the anterior Monteggia fracture. J Bone Joint Surg Br 31: 578-588.
-
Tompkins DG (1971) The anterior Monteggia fracture: observations on etiology and treatment. J Bone Joint Surg Am 53: 1109-1114.
-
Dormans JP, Rang M (1990) The problem of Monteggia fracture dislocation in children. Orthop Clin North Am 21(2): 251-256
-
Terry Canale (2003) Fractures and dislocations in children. In: Terry Canale S (Eds.) Campbell’s Operative Orthopaedics 10th(Edn.) Mosby, Philadelphia, 2: 1391-1568.
-
Ravessoud F (1985) Lateral condyle fracture and ipsilateral ulnar shaft fracture: Monteggia equivalent lesions. J Pediatr Orthop 5(3): 364-366.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results