Dry Arthroscopy of the Shoulder: A Technical Tip for the New Starters to Shoulder Arthroscopy
Backround: Most of the shoulder pathologies can be treated by shoulder arthroscopy. The major problem for the surgeon who has just started the shoulder arthroscopy is the difficulty of finding the joint in the first attempt. This results with uncontrolled fluid leakage to the surrounding soft tissues. Especially in obese patients this condition prolonges the operation duration. To prevent this, the following procedure is recommended. Methods: The technique can be summarized as follows: i. after entering from the posterior portal; the arthroscope is placed on to the three way canula, however the joint is not filled with fluid. ii. An injector is used to inject air from the canula. iii. Pumping the air makes the joint more visible and after dry dioagnostic arthroscopy the fluid can be pumped. Results: This technique enables the surgeon to fill the joint after being sure that the canula is in the joint to prevent unconrolled fluid extravasation. By this procedure the natural view of the joint can also be seen. A diagnostic arthroscopy can easily been done. Discussion and conclusion: We recommend this technique in the first 10 shoulder arthroscopy of the new starter surgeon. It is suggested to apply classical procedures after gaining considerable experience. But the technique can be used for dry diagnostic shoulder arthroscopy also by an experienced surgeon. Level of Evidence: Level V
Introduction
Arthroscopy of the shoulder is a well established and routine procedure. Most of the shoulder pathologies can be treated by shoulder arthroscopy. It has become a popular therapeutic and diagnostic procedure during the past two decades. The major problem for the surgeon who has just started the shoulder arthroscopy is the difficulty of finding the joint in the first attempt. This results with uncontrolled fluid leakage to the surrounding soft tissues. Especially in obese patients this condition prolonges the operation duration [1]. In other fields of surgery, such as laparoscopy, water is not used to maintain the optic cavity; instead carbon dioxide is used. Levin et al devised a balon for this purpose when dissecting in soft-tissue planes [2]. Other researchers have used traction from the soft tissues to develop the optic cavity when raising flaps [3, 4]. To summarize, water is neither crucial nor necessary to see inside any given cavity. This article presents our experience with more than 200 cases in the technique of dry arthroscopy of the shoulder which is still being used by some shoulder surgeons.
Surgical Technique
All surgical procedures are performed with the patient in the seated beach-chair position under general anesthesia. Routine portals are used. Steps can be summarized as follows: After entering from the posterior portal; the arthroscope is placed on to the three way canula however the joint is not filled with fluid. An injector is used to inject air from the three way canula. After pumping the air manually with a 50 cc injector, the joint becomes more visible (Figure 1). The remaining steps of the joint exploration do not vary from the wet technique. This method enables the surgeon to fill the joint after being sure that the canula is in the joint. By this procedure the natural view of the joint and the pathology can easily be seen without a fluid effect of blurring with some bleeding (Figure 2).
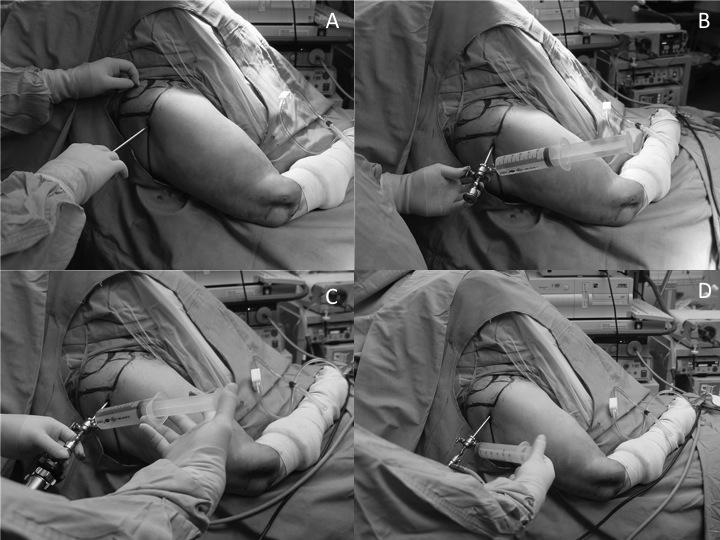
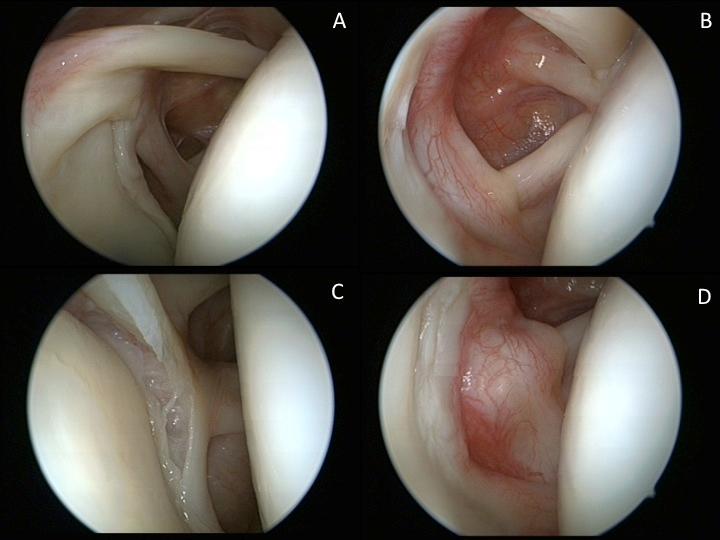
Figure 2: Biceps tendon (A) and SLAP lesion (D) in dry technique, visible capillary circulation and hyperemic areas in the joint (B,C) Our recommendation is to avoid too close to the scope tip when examining the tissues to avoid splashes. If there is a minor splash onto the scope’s tip it can be removed by gently rubbing the tip on the local soft tissue. This will clear the view sufficently.
Discussion
Traditionally shoulder arthroscopy has been performed with water in an attempt to maintain the optic cavity; however, as shown in other areas of the body (abdomen, thorax) or when raising flaps, water is not required [2, 3, 4]. Water has inherent disadvantages. It runs out through portals, causing loss of vision, and may cause some complications. Fluid extravasation has been reported associated with uncontrolled pressure of the joint. Excessive extravasation to avoid neurologic injury and respiratory problems requiring agressive airway management is also reported [1, 5, 6, 7]. Repeated entering to the shoulder may cause different portals that leads to fluid extravasation. The dry technique is an easy method for new starters to shoulder arthroscopy in being sure that the canula is in the joint cavity. On the other hand the technique enables the surgeon to see the natural view of the tissues in the joint which is a preferred method for some surgeons [8]. For example it is difficult to see a hyperemic area under pumps pressure. Sometimes fluid makes it difficult to see inside because of the blurring due to the bleeding in the cavity. This is usually not a problem for the experienced surgeon. But a new starter needs time to see and overcome this blurring with more fluid leakeage to the tissues. Although we do not have any experience, the dry technique is probably inappropriate when using thermal or laser probes. The generated heat cannot dissipate by air alone and, in our opinion, there is a risk of widespread, uncontrollable soft tissue and/or chondrocyte burning. For this reason we do not advise using this type of device without water running through the area. Also, some signs and findings differ from those found in the wet technique. For example the inflamed synovium will not float, it will stick to the capsule: its redness and hypertropy will point to the existance of synovitis.
Conclusion
We recommend this technique in the first 10 shoulder arthroscopy of the new starter surgeon. But an experienced surgeon can still use the technique to see the natural structure of the joint such as hyperemic areas in the joint.
References
-
Berjarno P, Gonzalez BG, Olmedo JF, Perez-Espana LA, Munilla MG (1998) Complications in arthroscopic shoulder surgery. Arthroscopy 14(8): 785-788.
-
Levin LS, Rehnke R, Eubanks S (1995) Endoscopic surgery of the upper extremity. Hand Clin 11(1): 59- 70
-
Friedlander L, Sundin J (1994) Minimally invasive harvesting of the latissimus dorsi. Plast Reconst Surg 94(6): 881-884.
-
Venkataramakrishnan V, Southern SJ (1997) Endoscopic rectus harvest: a simplified sheath-saving technique. Ann Plast Surg 39(6): 573-577.
-
Borgeat A, Bird P, Ekatodramis G, Dumont D (2000) Trackeal compression caused by periarticular fluid accumulation. A rare complication of shoulder surgery. J Shoulder and Elbow Surg 9(5): 443-445.
-
del Pinal F, Garcia-Bernal FJ, Pisani D, Regalado J, Ayala H, et al. (2007) Dry arthroscopy of the wrist: surgical technique. J Hand Surg Am 32(1): 119-123.
-
Hynson JM, Tung A, Guevara J (1993) Complete airway obstruction during arthroscopic shoulder surgery. Anesth Analg 76(4): 875-878.
-
Rupenian P (2013) Dry arthroscopy of the shoulder. Arthrosc Tech 2(4): e437-e440.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results