Arthroscopic Sutures of the External and Internal Meniscus at Ordre De Malte Hospital in Dakar: The Case of 13 Patients
Introduction: The management of traumatic lesions of the menisci is an up to date topic. The treatment has for long remained mutilating and the evolution towards osteoarthritis inevitable. In the light of the original work, important progress has been noted, which now allows conservative arthroscopic treatment in about 20% of cases. The scarcity of data in the West African literature on this topic and the need for a retrospective look at such a treatment which has been practiced at Ordre de Malte Hospital since 2012, motivate this study. Material and Method: This is a retrospective study from 2012 to 2015. A series of 13 meniscal sutures or 10.5% of 124 lesions explored and treated arthroscopically. This exclusive male series whose mean age is 28 years (20 - 49) was followed with a average follow-up of 38 months (23 - 62).<br />Results: The average consultation time was 2 years and for 11 times (85%) the lesion had occurred following an accident during sport, of a contact + / pivot type . The lesions being found 11 times on the right, 9 times on the medial meniscus, 10 times on the posterior segment, and 9 times on the average segment. It was a bucket handle in 9 cases including 4 dislocated cases. The suture was performed "from outside to inside" and was made stable with an average of 2 points with Prolene 2/0. In 3 cases, this suture was associated with ACL DIDT Ligamentoplasty. We noted as complications: a case of intraoperative failure that led to partial regulation, an early superficial infection of the operative site and a thromboembolic event that had evolved well under treatment. At the last follow-up, 11 patients were satisfied or very satisfied compared to 2 disappointed. The average Lysholm score was 94.7 / 100 with 12 good or excellent results; the IKS score was 100% in all patients and the average knee IKS was 95.6 / 100. IKDC clinical evaluation of 10 patients seen at last follow-up reported 07 patients ranked "A" and 03 ranked "B". Anatomically, the MRI and the Arthro-CT found evidence of partial scarring. 9 patients resumed sport, and 4 of them claimed to have achieved their previous performance.Conclusion: The functional results encourage the continuation of this activity with equipment enabling internal reparations.
Introduction
The therapeutic modalities of meniscal lesions have evolved with the progress of arthroscopic surgery and especially with the understanding of anatomy, biomechanics and the importance of meniscus in articular physiology [1, 2]. Meniscectomy is a surgical intervention which used to seduce sportsmen thanks to its immediate and brief surgical follow ups but it doesn’t anymore because it has proved to be deleterious to functions of the knee in the medium and the long term; that’s why, the concept of "meniscus preservation" is becoming more and more important and requires from every surgeon a tendency to preserve the meniscus as long as possible [3, 4]. If European authors are at more than thirty years of meniscal reparations [5], in Africa, Maghreb [6] and South Africa [7] is the top. Data are scarce in sub-Saharan Africa and only one recent study reports on the Nigerian experience with five cases [8]. Arthroscopy has been performed regularly at Ordre de Malte Hospital (CHOM) of Dakar since 2012. Our study aims to report the indications of meniscal suture in our context and to evaluate the therapeutic results.
Patients and Methods
We report our experience through this retrospective, prospective and fully inclusive study of patients treated with arthroscopic meniscal suture from January 2012 to December 2015 at CHOM. During this period, 124 meniscal lesions were explored with arthroscopy (Figure 1) among them 13 or 10.5% required suture by the technique of "outside in" using a G18 needle, a shuttle-relay and prolene 2/0. The other meniscal surgeries performed are represented on (Figure 2).
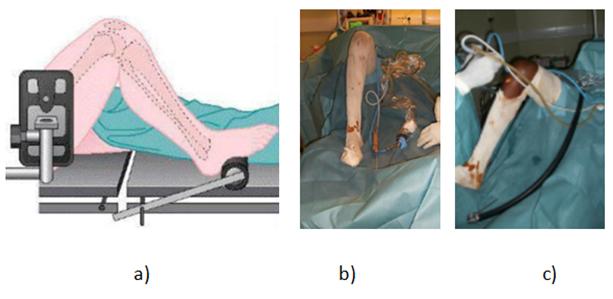
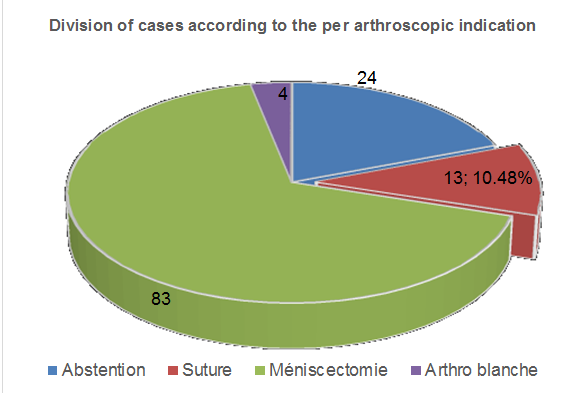
Figure 2: Different arthroscopic meniscus interventions. This exclusive male series, with a mean age of 28-years (22-49) and a mean follow-up of 38 months (23-62) characterized by a telephone-based assessment in 3 cases, a clinical examination in 10 cases, and imaging in three patients with residual symptoms. In so doing, pre- and postoperative clinical and paraclinical parameters as well as per arthroscopic findings have been reported.
Results
Patient Characteristics
All our patients were athletes classified according to ARPEGE C3 = 2 cases and L3 = 11 cases. The circumstances of occurrence of the trauma were specified in 11 cases, including 10 soccer-related accidents (PSA) and one Kick-boxing case. The average consultation time was 24.8 months with extremes of 1 week to 12 years.
The Diagnosis
It was suspected on the basis of clinical arguments: functional and physical. The meniscal lesion was confirmed on MRI in 11 cases and in 2 cases the meniscal lesion was discovered arthroscopically respectively in the context of ACL reconstruction using the DIDT technique and exploratory arthroscopy on a symptomatic knee without conclusive MRI. The longitudinal lesions and peripheral siege as shown in (Figure 3) was an excellent indication of meniscal suture.

Operation Data
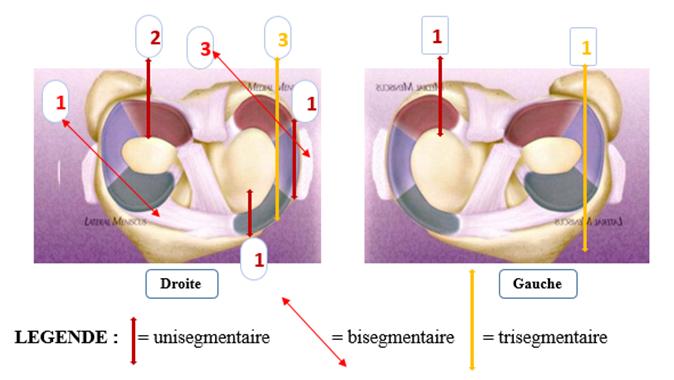
Exploration: The lesion was located in the right knee in 11 cases and in 9 cases the medial meniscus was affected. It was limited to a meniscal segment in 5 cases, bisegmented and trisegmened in 04 cases respectively. It appeared as a bucket handle in 9 cases including 4 dislocated in the intercondylar indentation. The mapping of the sutured lesions is shown in Figure 4.
Postoperative Data
Immediately: An average hospitalization of 3 days (1 - 7) during which a rehabilitation protocol was started, including a discharge and a 90 ° flexion limitation. In the Average Term: the Follow-up during the first 6 months with total discharge for 8 weeks recorded a thromboembolic event in a 49-year-old patient who had recovered well under treatment. He was allowed to resume sport from the 6th month. No local vasculo- neurotic complication has been reported. At the Last Follow-Up: With an average follow-up of 38 months (23 - 62), the functional signs reported were the pain that appeared during intense activities in 3 cases, one of which was associated with episodic joint swelling.
The last physical examination consisted of the evaluations of the different scores.
- LYSHOLM score: The average Lysholm score was 94.7 / 100 with extremes of 75 and 100. Twelve patients (92%) had a good or excellent result.
- IKS score: The subjective rating was: disappointment in 2 cases, and 11 patients were satisfied or very satisfied. The IKS knee score was on average 95.6 / 100 with extremes of 90 and 100 and the IKS function of 100/100 in all our patients.
- IKDC score: out of 10 patients assessed, 07 were rated "A" and 03 "B" Sports Activities: Effective reoperation on 9 patients including: Four who have achieved their previous performance (the professional soccer player, the kick-boxer and the 2 recreational soccer players). Three case whose performances are limited respectively to 50%; 60% and 90% due to symptoms appearing during intense sports activities. Two claiming to have a subjective fear with a psychological limit in their performance for the sport which they consider leisure sport. Anatomo-Radiological Evaluation: It is the Anatomo- radiological evaluation which proves the meniscal healing. It was performed in 4 patients showing: on an MRI control, the continuity of the meniscal tissue post- suture while evoking the existence of a sequential contrast in the form of intestinal hyper signal (Figure 5b).
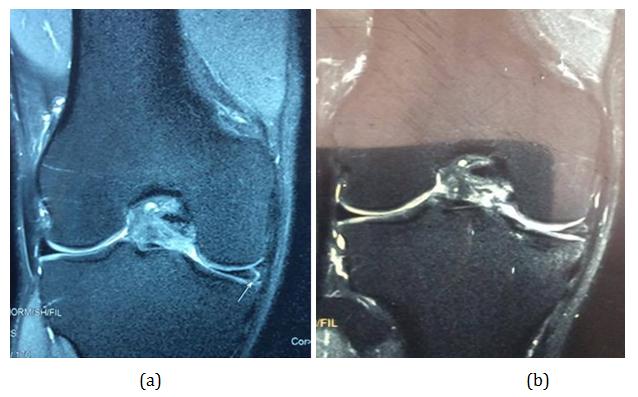
according to HENNING criteria (Figure 6 a-b)

Discussion
This retrospective and prospective study of an exclusively male series of 13 meniscus sutures from outside to inside is, together with the Babalola series [8], the only and recent data available in West African literature on this type of treatment. Note that these two series have several points in common: the male exclusivity, the suture technique used with 2nd generation equipment, the type of sutured lesion, the seat of lesions to name but a few.
Indeed, health care in the West African sub-region shares the same difficulties. This is evidence which confirms the relative delay in our countries in following technological developments in the medical field [5]. Surgeons often face increasing demands for care from patients who are very informed about certain issues without health policies being really attentive to this type of care. courageous initiatives with the available equipment are very often the effective way which is not only going to satisfy patients who cannot afford a medical evacuation outside the continent but also it is going to encourage decision-makers to strengthen the technical platforms. This local and sub-regional reality is not an obstacle to the discussion of our results with data from countries with advanced technology because the safety measures and the satisfaction expected from the patients remain the same. So the overall rate of meniscal repair in our service remains low compared to the theoretical rate of 20% proposed by Rodineau [9]. Our repair rate despite the small size of our series is much higher than the 3% of Our average of 24.8 months (1 week - 12 years) is a witness of the chronicity of the repaired lesions, it is comparable to the data from all around literature (Table 1). The meniscal ligament lesions are known for their long delay of consultation even in the countries with advanced technology. So biomechanically, one can affirm that on lax knees, some meniscal lesions observed during the repair are not concomitant of the initial accident. On the other hand, they appear or they are worsened by the hyper- solicitation of the medial meniscus to supplement broken ACL as well as episodes of knee dislocation. However, the prognosis would be better when the repair takes place in the first 3 months [10].
suture reported by BENHIMA in his series of 120 athletes in Morocco [6]. In France, the first meniscal sutures dates back to more than 30 years but the progression has long remained below the theoretical proportion of RODINEAU increasing from 2.5% to 12.05% between 2006 and 2012 [3] according to the ATIH.
Consultation Delay
| Series | Number of cases | Average delay in month | Extremes |
|---|---|---|---|
| Charrois [11] (2003) | 203 | - | 8,7-14,2 months |
| Accadbled [12] (2006) | 52 | 12 | - |
| Gadeyne [13] (2006) | 156 | 31,6 | 0-91,3 months |
| Raji [14] (2009) | 126 | 23,6 | 1 day-12 years |
| Jan [15] (2016) | 132 | 4 | 1 week-30 yeas |
| Babalola [8] (2017) | 5 | 10 | - |
| Our Series (2017) | 13 | 24,8 | 1 week-12 years |
Table 1: Comparative delays with different authors Table 1: Comparative delays with different authors
Diagnosis
All our patients had preoperative MRIs. MRI is the inevitable morphological examination on virgin knee according to several authors [16, 17, 18, 19]. Its prescription is ideal before any meniscal action to reduce the frequency of white arthroscopies (3% in our service). On the other hand, certain special realities, such as the fact that surgical procedures are taken into account by insurance companies, to the detriment of diagnostic assistance examinations that are on the responsibility of the patient, often lead to arthroscopy for diagnostic purposes as reported by THAUNAT [17]. Suture itself: the technique ‘from outside to inside’ is cheap because it is done with the help of 2nd generation equipment in a context of insufficient resources. This material adapted to the repair of the lesions of the anterior and middle segments of the meniscus [1] does not make the surgeon more comfortable since with this method he is going to be confronted with more posterior lesions and therefore will expose the patient to vascular- nervous complications. This technique should be associated with a 3rd generation for the majority of bucket loop type lesions which was the frequently repaired type in our series. This could explain the 2 cases of intraoperative difficulties reported in our study and thus justifies a recommendation to acquire this additional material to optimize the results. As for the dominant seat in the medial meniscus and frequent in the posterior and middle segments, the same findings have been reported by CHARROIS [11] in his retrospective and prospective series. All this corroborates the work on TRILLAT mechanisms lesions [20]. The
extent of the lesion defines the number of points that can stabilize it. Thus our average number of points was 2 (1- 3) similar to that reported by JAN [15]. Nevertheless, the number of bucket handle lesions in our series confronted with JAKOB’s assertion [4]: "it is not possible to fix a longitudinal fracture of 4 cm length with 3 points to imply that the number of our points were sometimes insufficient due to the difficulties to reach the posterior segment with our instruments. Treatment of associated lesions: Three times the suture was associated with ligamentoplasty type DIDT ACL. This double repair is recommended by ROCHCONGAR [21] because he says, the effect is synergistic. So for him 80% of these double lesions should be repaired once at a time to optimize the final result. Therapeutic results: The meniscal suture is performed to enable the healing of the meniscus and to avoid the pejorative effects of meniscectomy on the function of the knee on the short-term and the cartilage in the medium and long term. BEAUFILS has issued criteria of assessment by stipulating that the legitimacy of such an intervention supposes [1]. That his functional results correspond to those of a meniscectomy: our subjective result reported 11 patients (85%) satisfied and very satisfied with the intervention with resumption of sport in 9 of them. This was supported, on the one hand, by the improvement of preoperative symptoms, which persisted at a reduced intensity only in 3 patients and, on the other hand, by the different functional and objective scores obtained at the last follow-up: Lysholm score (12 patients, ie 92%). good and excellent results); IKS score of 100/100 function in all our patients. BEAUFILS [1] reported that the overall results of meniscal repair vary in the literature with 70 to 90% of good clinical results for medium and long term studies. Also the resumption of sport activities in 9 cases seems to us an objective argument. Our results are comparable to those of other authors (Table 2).
| Series | Number of cases | Average | IKDC (A+B) | LYSHOLM (very good + good) |
| IKS | ||||
| Katabi [22] (2003) | 203 | - | 97% | - |
| Fazilleau [23] (2012) | 39 | - | - | 65% |
| Our Series (2017) | 13 | 95,6 | 10/10 assessed | 92% |
Table 2: Final results of other authors Table 2: Final results of other authors That the rate of secondary meniscectomy, proof of
Table 2: Final results of other authors Table 2: Final results of other authors That the rate of secondary meniscectomy, proof of failure of the repair is not too high: No case of secondary meniscectomy in our series where the most recent surgery has a total of 2 years of follow-up. The absence of secondary meniscectomy could be considered as evidence of suture success because in the literature secondary meniscectomies are observed in about 15 to 20% of cases (9) and 83% of these failures occur in the first two years of life. [10]. However, the small size of our sample is a real limit. That the reality of meniscal healing after repair is demonstrated: this healing needs to be proven in clinical practice only in front of the persistence of annoying symptoms. All our symptomatic patients at the last follow-up do not have a discomfort which requires a reoperation and present to Arthro-CT at least a partial healing. That the gesture of meniscal repair is not deleterious in itself in case of failure: Our two reported difficulties are attributable unambiguously to the material which limits our suture indications [24].
Conclusion
This short experience allowed us to treat meniscal lesions locally with modest equipment according to the concept of "meniscal preservation". Future medico- technical efforts and early care when dealing with suspected meniscal lesions will expand our indications and optimize our results.
References
-
Beaufils P, Boisrenoult P, Charrois O, Jouve F, Pujol N, et al. (2011) Meniscal repair and replacement. Maîtrise Orthopédique 209: 21.
-
Clavert P, Kempf JF, Kahn JL (2006) Anatomical reconstruction of the anterior cruciate ligament. Rev Chir Orthopédique Réparatrice Appar Mot 92(5): 172-174.
-
Lutz C, Dalmay F, Ehkirch FP, Cucurulo T, Laporte C, et al. (2015) Méniscectomie versus réparation méniscale : résultats radiocliniques à 10 ans des lésions verticales sur genou stable. Rev Chir Orthopédique Traumatol 101(8): S301-305.
-
Jakob R (1992) Les lésions des ménisques du genou et leur traitement actuel. Expansion Scientifique 111- 132.
-
Seil R, VanGiffen N, Pape D (2009) Thirty years of arthroscopic meniscal suture: What’s left to be done? Orthop Traumatol Surg Res 95(8): 85-96.
-
Benhima MA, Bouyarmane H, Arssi M, Gourram H, Fnini S, et al. (2008) Lésions méniscales isolées chez le sportif. À propos de 120 cas. J Traumatol Sport juin 25(2): 86-90.
-
Kruger N, McNally E, Al-Ali S, Rout R, Rees JL, et al. (2016) Three-dimensional reconstructed magnetic resonance scans: Accuracy in identifying and defining knee meniscal tears. World J Orthop 7(11): 731-737.
-
Babalola R, Laiyemo E, Itakpe S, Madubueze C, Shodipo O (2017) Arthroscopic outside-in meniscal repair: A short-term clinical experience. Afr J Med Health Sci 16(1): 1-5.
-
Rodineau J (2014) « Conférences d’expert » et « controverses » en traumatologie. J Traumatol Sport Juin 31(2): 121-126.
-
Djian P (2006) Lésion méniscale latérale sur genou stable: réparation ou méniscectomie. Rev Chir Orthopédique Réparatrice Appar Mot 92(5): 175-177.
-
Charrois O (2004) Présentation des deux séries du symposium. Rev Chir Orthopédique Réparatrice Appar Mot 90(8): 57-59.
-
Accadbled F, Bergerault F, Cassard X, Knorr J (2007) Traitement conservateur des lésions méniscales traumatiques : étude rétrospective. Rev Chir Orthopédique Réparatrice Appar Mot 93(6): 107-108.
-
Gadeyne S, Besse JL, Galand-Desme S, Lerat JL, Moyen B (2006) Lésions méniscales constatées lors de la reconstruction du ligament croisé antérieur. Rev Chir Orthopédique Réparatrice Appar Mot 92(5): 448-454.
-
Raji A (2009) Le traitement des lésions méniscales sous arthroscopie : à propos de 126 cas. Expérience du service de traumatologie-orthopédie de l’HMIM V de Rabat. Thèse de doctorat d’état Med. Faculté de Médecine et de pharmacie-Rabat, pp: 65.
-
Jan N, Fayard JM, Chambat P, Sonnery-Cottet B, Thaunat M (2015) Résultats des sutures tout en dedans par abord postéromédial des lésions du ménisque médial lors de la reconstruction du LCA au recul moyen de 24 mois. Rev Chir Orthopédique Traumatol 101(8): e1.
-
Barber BR, McNally EG (2013) Meniscal Injuries and Imaging the Postoperative Meniscus. Radiol Clin North Am Mai 51(3): 371-391.
-
Thaunat M (2007) Beyond the miracle. Voyage d’étude à Cape Town. N°167.
-
Bellaiche L, Charousset C, Duranthon LD, Grimberg J, Petrover D (2006) Imagerie du genou : quel examen pour quelle pathologie? Rev Rhum Juin 73(6): 617- 624.
-
Weber-Donat G, Pons-Ukkola E, Labrunye C, Teriitehau C, Baccialone J, et al. (2012) Place de l’IRM dans la prise en charge des lésions méniscales instables. Feuill Radiol 52(6): 307-313.
-
Trillat A (1962) les lesions traumatiques du ménisque interne du genou: classification anatomique et diagnostic clinique. Rev Chir Orthop 48: 551-560.
-
Rochcongar G, Cucurulo T, Ameline T, Potel JF, Dalmay F, et al. (2015) Meniscal survival rate after anterior cruciate ligament reconstruction. Orthop Traumatol Surg Res 101(S8): S323-S326.
-
Katabi M (2003) Réparation méniscale: les résultats globaux. SFA 3: 59-62.
-
Fazilleau F, Clavé A, Poirier N, Le Nen D, Dubrana F (2012) Lésions isolées du ménisque latéral sur genou stable opérées : étude fonctionnelle à 10ans de suivi. J Traumatol Sport 29(4): 184-191.
-
Pujol N, Beaufils P (2016) Les nouvelles lésions méniscales réparables. E-Memoires Académie Natl Chir 15(1): 29-33.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results